
Abstract
Purpose
Little is known about the prevalence of mental health problems among adolescents in Sub-Saharan Africa. Research consistently determined violence and maltreatment to be important risk factors. In this study, we examined the prevalence of mental health problems among adolescents in Tanzania, as well as the association with exposure to violence and maltreatment.
Methods
We administered a set of questionnaires (e.g., strength and difficulties questionnaire; conflict tactic scale) to a nationally representative sample of 700 Tanzanian secondary school children (52% girls; age 14.92 years, SD = 1.02) and 333 parents or primary caregivers (53% females; age 43.47 years, SD = 9.02).
Results
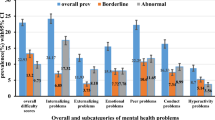
41% of the students reported an elevated level of mental health problems (emotional problems 40%, peer problems 63%, conduct problems 45%, hyperactivity 17%) in the past 6 months. Concordantly, 31% of parents reported observing an elevated level of mental health problems in their children (emotional problems 37%, peer problems 54%, conduct problems 35%, hyperactivity 17%). After controlling for other risk factors, we found significant associations between physical violence by parents and adolescent’s mental health problems reported by students (β = 0.15) and their parents (β = 0.33).
Conclusions
Our findings suggest a high prevalence of mental health problems using screening tools among secondary school students in Tanzania as well as an association between physical violence by parents and adolescents’ mental health problems. Our findings emphasize the need to inform the population at large about the potentially adverse consequences associated with violence against children and adolescents.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Mental health problems among children and adolescents in low-income countries
Mental health problems are the leading cause of behavioral adjustment difficulties among children worldwide [1, 2]. Mental health problems can result in a child being unable to successfully perform mental functions, possibly resulting in reduced productivity, reduced success in developing fulfilling relationships with others, and an inability to change or cope with adversity [3]. Approximately 10–20% of the world’s children and adolescents experience mental health problems each year [4,5,6,7]. However, most of the findings on the prevalence have been reported for high-income countries [8, 9].
The few studies available indicate that mental health problems in children across low and middle-income countries are prevalent. For example, a study by Patel et al. [4] indicated that mental health problems were common in 27% of minors in Brazil, 18% in Ethiopia, and15% in South Africa. From Sub-Saharan Africa, a meta-analysis of ten studies with a sample of 9713 children from 5 countries indicated that one in seven children and adolescents reported significant mental health difficulties, with one in ten children having a specific psychiatric disorder [10].
In Tanzania, studies by Hermenau et al. [11, 12] reported depressive symptoms, posttraumatic stress symptoms, and aggressive behaviors in orphaned children. Moreover, Hecker et al. [13, 14] found internalizing and externalizing problems in a sample of primary school children. Studies from secondary school children [15, 16] also indicated prevalence of delinquent behavior, aggression and, conduct problems. However, these findings are based on at-risk or non-representative samples, and there is to date no nationally representative prevalance data of mental health problems of children available.
Risk factors for mental health problems of children and adolescents
Research findings worldwide have linked mental health problems in children and adolescents with different risk factors inside and outside the family [17, 18]. However, a large body of literature, mostly from high income countries, indicated maltreatment by parents or caregivers as one of the main predictors of mental health problems in children [19,20,21]. Studies emphasized that maltreatment and violence are associated with aggression, conduct disorder, anxiety disorders, and depression [21, 22]. For example, exposure to physical violence was highly associated with externalizing behavior outcomes both in toddlerhood and in later ages [19]. Furthermore, Weaver et al. [23] added that experiencing physical violence by age 10 predicted violent behavior and delinquency in adolescence ages.
In Sub-Saharan Africa, studies from Burkina Faso [24] and from Uganda [25] found a significant relation between mental health problems and parental violence in school-aged children. In Tanzania, studies by Hermenau et al. [12, 26] reported that physical and emotional violence in orphaned children was associated with mental ill-health and aggressive behavior problems. Moreover, Hecker et al. [13, 14] reported strong associations between harsh discipline, internalizing problems and externalizing problems in school children. However, all these findings are based on at-risk or non-representative samples.
There is also no doubt that also other factors contribute to the development of mental health problems in children, including biological, familial or social factors. For example, peer violence has strong associations with different mental health problems in minors [27]. Moreover, children’s age and gender seem also to contribute to the degree of mental health problems in minors [28]. Additionally, parental age and gender are reported in different studies to be associated with behavior problems in children [29]. Furthermore, other studies reported strong associations between parental stress, household income, and other familial factors to mental health problems of children [17, 30].
Objectives
In this study, we assessed Tanzanian secondary school students and their parents in a nationally representative sample. Our first aim was to examine the prevalence of mental health problems of secondary school students in Tanzania. We expected a high prevalance of mental health problems (i.e., conduct problems, hyperactivity, emotional symptoms, and peer problems) among Tanzanian secondary school students.
Our second aim was to investigate the association between violence and maltreatment by parents and mental health problems of adolescents. We hypothesized that violence by parents would be associated with adolescents’ mental health problems. We controlled for other potential influential factors, including personal and family factors, and violence outside of the family.
Methods
Design and sampling
The study included 6 (of 25) regions in Tanzania. Five regions were selected randomly. Additionally, the largest city of the country, Dar es Salaam, was intentionally selected. In each region one mixed-day secondary school from the regional capital was randomly selected. Similarly, one rural district was randomly selected from which a single mixed-day secondary school was also randomly selected. In Dar es Salaam, one of the cities’ municipals was randomly chosen, from which one mixed-day secondary school was selected at random. Within each selected school, 120 students in the 8th and 9th year of formal schooling were stratified by gender and then randomly selected.
Procedure
The study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The University of Dar es Salaam on behalf of Tanzanian Commission for Science and Technology and the Ethical Review Board of the University of Konstanz approved the study. Only parents who gave their informed consent in written form and adolescents with written parental informed consent and who freely provided assent themselves were included in this study. Prior to data collection, a letter explaining the study’s aims and procedures was sent together with an informed consent form to the parents or caregivers to seek parental consent. In total, 63% of the forms were returned. Students filled out questionnaires in groups of 3–5 on the school grounds under supervision of a research assistant. The completion of questionnaires took an average of 45 min.
The parents were contacted through letters and phone calls. Of the 700 parents contacted in all schools, 333 (48%) parents were willing and able to participate. Parents were invited to come to the respective schools. They were asked to sign an informed consent document and each parent filled out the questionnaire in a one-on-one interview setting within an average completion time of 30 min. A compensation of approximately three USD was given to each attending parent.
Participants
A total sample of 700 students participated in the study (see Table 1). In total, 54% (n = 376) of the students lived with both parents, 28% (n = 197) with one parent, 18% (n = 124) with other relatives and/or in other facilities. The 333 participating parents or primary caregivers had a mean of 7.69 years (SD = 2.66) of formal education. Parent or caregiver types of employment ranged from formal 13% (n = 42), non-formal but reliable 33% (n = 110), non-formal and unreliable 44% (n = 146) to no employment 10% (n = 35). The majority of parents reported a low monthly household income pursuant to the government analysis of monthly household income for Tanzanian families which was around 25 USD as per year 2001 to 2007 [31].
Measures
Following established international guidelines [32] all instruments were translated into Swahili and back translated to English in a blind written form. The first part of the questionnaire gathered demographic information, such as age, gender, and living conditions of students and parents, respectively.
Exposure to violence
Students’ experiences of violent punishment both at home and at school in the year preceding the investigation were assessed with items from the parent–child version of the Conflict Tactics Scale (CTSPC) [33] which were filled out by both students and parents. For the purpose of the present study, participating students completed this questionnaire twice: first referring to violence and neglect they experienced from their parents or caregivers and second referring to the violence by teachers. Parents filled out in respect to violence they apply to their participating child. The items of the scales are rated on seven answer categories from “never” (0) to “more than 20 times” (25) and are then summed up to one score per subscale. The CTSPC comes with low to moderate psychometric properties for the two subscales of interest, indicating Cronbach’s alpha coefficients of α = 0.55 for physical violence and α = 0.60 for emotional violence. The mangling alpha reliability can be explained by the fact that the items of the scale measure rather rare events, and that the correlation between items, which is the basis of alpha, are low due to extreme skewness [33]. Nonetheless, CTSPC has been used worldwide and its validity has been underscored by numerous studies [34].
In addition, we assessed peer violence using three items of the Maltreatment and Abuse Chronology of Exposure [35]. The items in this sections were: Has any peer in your whole life ever … (1) “called you names or said hurtful things more than a few times a year?”, …(2) “said things behind your back, posted derogatory messages about you, or spread rumors about you?”, …(3) “hit you so hard or intentionally harmed you in such a way that you were injured?” These items were answered in two categories which are Yes (1) or No (0).
Adolescents’ mental health
Adolescents’ mental health problems were assessed using the Strengths and Difficulties Questionnaire (SDQ) [36] for parents and the SDQ self-report version for children. The SDQ consists of five subscales of five items each, which are answered in three categories from “not true” (0), “somehow true” (1) to “certainly true” (2). The sum of all items except the ones from the prosocial behavior subscale represents a total difficulty score (SDQ score; range 0–40). Values of 17 or higher on the SDQ score indicate severely elevated levels of mental health problems [37]. Cut-off values for the four subscales of interest can be found in Table 2. The SDQ comes with good psychometric properties (SDQ score: α = 0.83) and has been repeatedly used in different countries [37], including Tanzania [12, 26].
Data analysis
To test the hypothesis that violence and neglect by parents are associated with mental health problems among adolescents, hierarchical multiple regression analysis was carried out. Preliminary analyses confirmed the tenability of all assumptions for linear regression models. Missing values made up 0.07% (n = 26) of the children’s data and 0.01% (n = 2) of the parents’ data, and were deleted listwise. The assumption of normal distribution of the residuals of the dependent variable following West, Finch, and Curran [38] could be uphold in both samples. Multicollinearity between predictor variables could be ruled out. No outliers were detected. Linearity, homoscedasticity, and independence of residuals were tenable. Effect sizes were calculated using Cohen’s f2, with f2 ≥ 0.02 indicating a small effect, f2 ≥ 0.15 a medium effect, and f2 ≥ 0.35 a large effect. Analyses were performed with IBM SPSS Statistics Version 23. Level of significance was set to an alpha of 0.05 and analyses were calculated one-tailed in case of directional hypotheses.
Results
Descriptive results
Table 1 displays children’s and parents’ descriptive statistics as indicated in their self-report. Table 2 displays the prevalence of mental health problems of both students’ self-report and the reports of their parents. 41% of children reported elevated levels of mental health problems in the past 6 months. Moreover, 31% of parents reported elevated levels of mental health problems of their children.
Association between exposure to violence and mental health problems
Students’ self-reports
The first step of the regression analysis showed that children’s demographic variables age, gender, and whether their parents were still alive or not (step 1) were significantly related to students’ self-reported mental health. Adding peer violence (step 2) improved the model further. Additionally, adding physical and emotional violence by teachers (step 3) improved the model significantly. By adding physical and emotional violence, and neglect by parents (step 4), the model was further improved. The full model explained 22% of the variability of students’ mental health problems. As indicated in Table 3, students’ gender, exposure to peer violence, to emotional violence by teachers, and to physical violence by parents were positively related to students’ self-reported mental health problems.
Report of parents
Parents’ demographic factors age, gender, and household income (step 1) were not significantly associated with students’ mental health problems. Adding parental stress (step 2) improved the model significantly. Adding the emotional and physical violence applied by parents (step 3) improved the model further. The full regression model of reports of parents explained 20% of the variance of students’ mental health problems. As indicated in Table 4, parents’ stress and physical violence by parents were strongly related to adolescents’s mental health problems.
Discussion
Prevalence of mental health problems among Tanzanian adolescents
Based on our nationally representative sample of secondary school students, we found a prevalence rate of self-reported mental health problems of 41% in the past 6 months. The report of their parents found a prevalence rate of 31%. With 65% (self-report) or 54% (report of others) peer problems were most prevalent, whereas with 17% (self-report and report of others) the prevalence of hyperactivity was least prevalent. Generally, the self-report of the students and the report of their parents were broadly consistent. Moreover, the current findings indicate that students’ self-report scores were generally higher than parents’ report scores. This is in concordance with previous studies [39, 40] that indicate that reports about experiences of violence and maltreatment as well as about mental health problems differ from low to moderate levels of agreement between adolescents and their parents due to divergent and different perspectives. One explanation in our sample could be that parents may not have been aware of their children’s mental health problems as adolescents rather share their problems with their peers than with their parents. However, we also cannot rule out the possibility that some adolescents may have overemphasized their mental health problems to receive support from the research team.
Generally, our findings are in line with our hypothesis and previous studies in Sub-Saharan Africa [10, 25]. Furthermore, our findings extend previous findings from Tanzania [12,13,14], as these were based on at-risk groups or specific non-representative samples. In contrast, our study is the first to examine the prevalence of mental health problems in Tanzanian adolescents using a nationally representative sample. Our findings imply that mental health problems are a matter of concern among secondary school students in Tanzania.
Though a previous study from Tanzania reported lower clinically relevant levels of peer problems (8%) and emotional problems (9%) in a sample of primary school children [13], these findings may be explained by two main reasons: first, data were assessed via structured interviews and prevalence rates using structured interviews are generally lower than prevalence rates based on self-administered questionnaires. Second, the sample was assessed in the very specific context of a private primary school that may not be representative for Tanzanian primary schools in general. Nonetheless, it is important to consider that the SDQ was selected as a screening tool to determine the prevalence of mental health problems. Per definition, screening tools have a high sensitivity, but a lower specificity. Future studies using structured clinical interviews are needed to replicate our findings. Notwithstanding, the high rate of mental health problems among secondary students in Tanzania as reported in this study calls—at least—for further attention for research and child protection programs in future.
Association between exposure to violence and mental health problems
The second aim of this study was to investigate the association between exposure to violence and maltreatment, and mental health problems. After controlling for the potential influences of students’ age, gender, whether their parents are alive or not, peer violence and violence by teachers, we found an incremental influence of physical violence by parents or primary caregivers on the self-reported mental health problems of adolescents. Yet, emotional violence by parents was not significantly associated with students’ mental health problems. In addition, peer violence and emotional violence by teachers were found to be associated with mental health problems of adolescents. In second step, we aimed to replicate these findings using the report of the students’ parents or primary caregivers. After controlling for the influence of parents’ age, gender, household income, and parental stress, we found a strong association between physical violence by parents and mental health problems of adolescents reported by their parents. In addition, there was a significant association between parental stress and adolescents’ mental health problems. Our findings indicate an agreement between the reports of students and their parents regarding the effects of physical violence applied by parents on adolescents’ mental state, underlining the strong association between physical violence by parents or caregivers with mental health problems among adolescents.
The findings of this study are partly consistent with previous studies, which found associations between physical, emotional, and peer violence, as well as parental stress and mental health problems in children in different countries [18, 25, 41, 42]. However, in contrast to previous findings we only found a positive association between physical but not emotional violence by parents and adolescents’ mental health problems. One explanation could be that physical violence by parents is often accompanied by emotional violence and students may remember and report physical violence rather than emotional violence when they occur together. As a consequence, parts of the effect of physical violence may be also attributed to emotional violence. However, our findings need to be replicated and the hypothesis pointed out here need to be tested further.
Moreover, we found a positive association between emotional—but not physical—violence by teachers and adolescents’ self- reported mental health problems. At first glance this finding is surprising. However, the high prevalence of physical violence by teachers and the fact that almost every student is frequently exposed to physical violence [43] may lead to the problem that adolescents may feel more humiliated and ashamed when experiencing emotional violence in front of their peers. As the self-esteem of adolescents is very much depending on their belonging to a peer-group, the threat of losing one’s status in the peer-group as a consequence of the humiliation in front of the peers may explain our findings. However, this hypothesis needs to be further investigated in future studies.
Considering the previous findings in Tanzania [12, 14, 26], the current study points in a similar direction, but is based on a nationally representative sample of adolescents’ self-reports and the reports of their parents. Previous findings supported the notion that many parents in Tanzania consider harsh discipline as effective in children’s behavioral management [14, 44]. As a consequence, parents continue to use violence when raising their children under the assumption that they are not harming their children—an assumption that does not hold when considering the findings of our study as well as previous findings from other settings [19, 20].
Implications and future research
When people and institutions would become aware of the possible consequences of violence and maltreatment, high costs for the health care system could potentially be avoided [45]. A first step will be to inform parents, social workers, institutions, governmental organizations, and the population at large about the potentially consequences of violence in education. In line with the United Nation’s Sustainable Development Goal Nr. 16.2 [46], there is a strong need to design and implement interventions that prevent children from violence by parents. Parents’ awareness about effective non-violent discipline strategies may be a starting point for interventions. While this study provides first empirical evidence from a nationwide representative sample on the prevalence of mental health problems and the association between violence and mental health problems in Tanzanian adolescents, future studies that replicate our findings are important. Furthermore, longitudinal and prospective studies will be helpful in understanding the causal relations between violence and mental health problems across the lifespan.
Strengths and limitations
There are some limitations that should be noted: first, the cross-sectional study design does not allow for the establishment of causality, however, the consistency with previous findings on the link between exposure to violence and mental health problems suggests that mental health problems can be the consequence of violence in families and elsewhere. Cultural bias might have influenced our findings, for example, due to the fact that some of the items may not always reflect typical life realities of a Tanzanian child. However, we kept this potential bias to a minimum as Tanzanian researchers played a key role in design and implementation of the study. The applicability of the instruments is further supported by the fact that the results were consistent with previous findings in Tanzania and Sub-Saharan Africa. Although information from both children and parents or primary caregivers was targeted, only just over half of the parents or primary caregivers of the attending students were able to participate.
Conclusions
The present study suggests that mental health problems are prevalent among secondary school students in Tanzania and that there is a strong association between physical violence by parents and mental health problems in children. Our findings emphasize the need to inform the population at large about the potentially adverse consequences associated with violence against children and adolescents. There is a need to design and implement interventions that protect children from violence in the family. Educating parents about effective non-violent discipline strategies might be a starting point. Due to the fact that child violence among society members in Tanzania is normed, societal awareness need to be emphasized.
References
Ferguson CJ (2013) Spanking, corporal punishment and negative long-term outcomes: a meta-analytic review of longitudinal studies. Clin Psychol Rev 33:196–208
United Nations (2014) Mental Health Matters: Social Inclusion of Youth with Mental Health Conditions
World Health Organization (2004) Promoting Mental Health: Concepts, Emerging Evidence, Practice. Geneva
Patel V, Flisher AJ, Hetrick S, McGorry P (2007) Mental health of young people: a global public-health challenge. Lancet 369:1302–1313
Kieling C, Baker-Henningham H, Belfer M, Conti G, Ertem I, Omigbodun O, Rohde LA, Srinath S, Ulkuer N, Rahman A (2011) Child and adolescent mental health worldwide: evidence for action. Lancet 378:1515–1525
WHO (2013) Mental Health Action Plan 2013–2020. Geneva
Crocetti E, Hale WW, Dimitrova R, Abubakar A, Gao CH, Pesigan IJA (2015) Generalized Anxiety symptoms and identity processes in cross-cultural samples of adolescents from the general population. Child Youth Care Forum 44:159–174
Savina E, Coulacoglou C, Sanyal N, Zhang J (2011) The study of externalizing and internalizing behaviours in Greek, Russian, Indian, and Chinese children using the Fairy Tale Test. Sch Psychol Int 33:39–53
Yewatkar VD, Pande PD, Bangde AL, Joshi T (2015) Prevalence of attention deficit hyperactivity disorder in children. Int J Res Med Sci 3:274–280
Cortina MA, Sodha A, Fazel M, Ramchandani PG (2012) Prevalence of child mental health problems in Sub-Saharan Africa. Arch Pediatr Adolesc Med 166:276–281
Hermenau K, Eggert I, Landolt MA, Hecker T (2015) Neglect and perceived stigmatization impact psychological distress of orphans in Tanzania. Eur J Psychotraumatol 6:28617
Hermenau K, Hecker T, Elbert T, Ruf-Leuschner M (2014) Maltreatment and mental health in institutional care—comparing early- and late-institutionalized children in Tanzania. Infant Ment Health J 35:102–110
Hecker T, Hermenau K, Salmen C, Teicher M, Elbert T (2016) Harsh discipline relates to internalizing problems and cognitive functioning: findings from a cross-sectional study with school children in Tanzania. BMC Psychiatry 16:118
Hecker T, Hermenau K, Isele D, Elbert T (2014) Corporal punishment and children’s externalizing problems: a cross-sectional study of Tanzanian primary school aged children. Child Abus Negl 38:884–892
Yaghambe RS, Tshabangu I (2013) Disciplinary networks in secondary schools: policy dimensions and children’s rights in Tanzania. J Stud Educ 3:42–56
Semali LM, Vumilia PL (2016) Challenges facing teachers’ attempts to enhance learners’ discipline in tanzania’s secondary schools. World J Educ 6:50–67
Saputra F, Yunibhand J, Sukratul S (2017) Relationship between personal, maternal, and familial factors with mental health problems in school-aged children in Aceh province, Indonesia. Asian J Psychiatr 25:207–212
Infurna MR, Reichl C, Parzer P, Schimmenti A, Bifulco A, Kaess M (2016) Associations between depression and specific childhood experiences of abuse and neglect: a meta-analysis. J Affect Disord 190:47–55
Gershoff ET, Lansford JE, Sexton HR, Davis-Kean P, Sameroff AJ (2012) Longitudinal links between spanking and children’s externalizing behaviors in a national sample of White, Black, Hispanic, and Asian American families. Child Dev 83:838–843
Gilbert R, Widom CS, Browne K, Fergusson D, Webb E, Janson S (2009) Burden and consequences of child maltreatment in high-income countries. Lancet 373:68–81
Herrenkohl TI, Hong S, Klika JB, Herrenkohl RC, Russo MJ (2013) Developmental impacts of child abuse and neglect related to adult mental health, substance use, and physical health. J Fam Violence 28:191–199
Young JC, Widom CS (2014) Long-term effects of child abuse and neglect on emotion processing in adulthood. Child Abuse Negl 38:1369–1381
Weaver CM, Borkowski JG, Whitman TL (2008) Violence breeds violence: childhood exposure and adolescent conduct problems. J Community Pschol 23:1–7
Ismayilova L, Gaveras E, Blum A, To-Camier A, Nanema R (2016) Maltreatment and mental health outcomes among ultra-poor children in Burkina Faso: a latent class analysis. PLoS One 11:1–25
Kinyanda E, Kizza R, Abbo C, Ndyanabangi S, Levin J (2013) Prevalence and risk factors of depression in childhood and adolescence as seen in 4 districts of north-eastern Uganda. BMC Int Health Hum Rights 13:19
Hermenau K, Hecker T, Ruf M, Schauer E, Elbert T, Schauer M (2011) Childhood adversity, mental ill-health and aggressive behavior in an African orphanage: changes in response to trauma-focused therapy and the implementation of a new instructional system. Child Adolesc Psychiatry Ment Health 5:29
Menesini E, Salmivalli C (2017) Bullying in schools: the state of knowledge and effective interventions. Psychol Health Med 22(sup1):240–253
Pankhurst A, Negussie N, Mulugete E (2016) Understanding children’s experiences of violence in Ethiopia: evidence from young lives. Florence; (November)
Tearne JE, Robinson M, Jacoby P, Allen KL, Cunningham NK, Li J (2016) Older maternal age is associated with depression, anxiety, and stress symptoms in young adult female offspring. J Abnorm Psychol 125:1–10
Neece CL, Green SA, Baker BL (2012) Parenting stress and child behavior problems: a transactional relationship across time. Am J Intelllect Dev Disabil 117:48–66
The Poverty Eradication Division of the Ministry of Planning and Economic Affairs of the United Republic of Tanzania, Research on Poverty Alleviation (2009) An analysis of household income and expenditure in Tanzania. Dar Es Salaam
Brislin RM, Lonner WJ, Thorndike RM (1973) Cross cultural research methods. Wiley, New York
Straus MA, Hamby SL, Finkelhor D, Moore DW, Runyan D (1998) Identification of child maltreatment with the Parent-Child Conflict Tactics Scales: development and psychometric data for a national sample of American parents. Child Abuse Negl 22:249–270
Straus MA, Hamby SL (1997) Measuring physical & psychological maltreatment of children with the Conflict Tactics Scales. In: Kaufman Kantor G, Jasinski JL (eds) Out of the darkness Contemporary research perspectives on family violence. Sage Publications, Thousand Oaks
Teicher MH, Parigger A (2015) The “Maltreatment and Abuse Chronology of Exposure” (MACE) scale for the retrospective assessment of abuse and neglect during development. PLoS One 10:1–37
Goodman R, Meltzer H, Bailey V (1998) The strengths and difficulties questionnaire: a pilotstudy on the validity of the self-report version. Eur child Adolesc 7:125–130
Goodman R (2001) Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry 40:1337–1345
West SG, Finch JF, Curran PJ (1995) Structural equation models with normal variables: problems and remedies. In: Hoyle RH (ed) Structural equation modeling: concepts, issues, and applications. Sage Publications, Thousand Oaks, pp 56–75
Duke N, Ireland M, Borowsky I (2005) Identifying psychosocial problems among youth: factors associated with youth agreement on a positive parent-completed PSC-17. Child Care Health Dev 31:563–573
Chan KL (2012) Comparison of parent and child reports on child maltreatment in a representative household sample in Hong Kong. J Fam Violence 27:11–21
Feinstein S, Mwahombela L (2010) Corporal punishment in Tanzania’s schools. Int Rev Educ 56:399–410
Wareham J, Boots DP (2012) The link between mental health problems and youth violence in adolescence: a multilevel test of DSM-oriented problems. Crim Justice Behav 39:1003–1024
Hecker T, Goessmann K, Nkuba M, Hermenau K (2018) Teachers’ stress intensifies violent disciplining in Tanzanian secondary schools. Child Abuse Negl 76:173–183
Nkuba M, Hermenau K, Hecker T (2018) Violence and maltreatment in Tanzanian families—findings from a nationally representative sample of secondary school students and their parents. Child Abuse Negl 77:110–120
Maher EJ, Corwin TW, Hodnett R, Faulk K (2012) A cost-savings analysis of a statewide parenting education program in child welfare. Res Soc Work Pract 22:615–625
United Nations (2015) Transforming our World: the 2030 Agenda for sustainable development. New York
Acknowledgements
This research was supported by the Young Scholar Fund of the University of Konstanz and vivo International. We thank all head of schools and the school counselors for their support in this study. We are very grateful to our research team, including: Getrude Mkinga, Andrew Mtitu, Gloria Mushi, Suzan Ngahyoma, Moyo Osiah Mwaihola, Rehema Mdoe, Simeon Mgode, Sophia Backhaus and Katharina Zepf. In a special way, we are grateful to Thomas Elbert for his support and supervision throughout the project.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interests.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Nkuba, M., Hermenau, K., Goessmann, K. et al. Mental health problems and their association to violence and maltreatment in a nationally representative sample of Tanzanian secondary school students. Soc Psychiatry Psychiatr Epidemiol 53, 699–707 (2018). https://doi.org/10.1007/s00127-018-1511-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-018-1511-4