
Abstract
Purpose
Migrants appear to have a higher risk of mental disorders, but findings vary across country settings and migrant groups. We aimed to assess incidence and prevalence of mental disorders among immigrants and Finnish-born controls in a register-based cohort study.
Methods
A register-based cohort study of 184.806 immigrants and 185.184 Finnish-born controls (1.412.117 person-years) was conducted. Information on mental disorders according to ICD-10 was retrieved from the Hospital Discharge Register, which covers all public health care use.
Results
The incidence of any mental disorder was lower among male (adjusted HR 0.82, 95% CI 0.77–0.87) and female (aHR 0.76, 95% CI 0.72–0.81) immigrants, being lowest among Asian and highest among North African and Middle Eastern immigrants. The incidence of bipolar, depressive and alcohol use disorders was lower among immigrants. Incidence of psychotic disorders was lower among female and not higher among male immigrants, compared with native Finns. Incidence of PTSD was higher among male immigrants (aHR 4.88, 95% CI 3.38–7.05).
Conclusions
The risk of mental disorders varies significantly across migrant groups and disorders and is generally lower among immigrants than native Finns.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Migrants appear to have an increased risk of some mental disorders [1, 2]. Several factors may negatively influence migrants’ mental health: neurodevelopmental problems caused by, e.g., infections or vitamin deficiencies; psychosocial stressors such as traumatic experiences prior to and during migration, and also discrimination, social adversity and minority stress in the recipient country; and risky health behaviours, particularly substance use [3]. However, selective migration and sometimes more favourable health behaviours interplay with the above-mentioned risk factors, and many indicators, such as mortality, show better health among migrants than native populations [4, 5].
Immigrant populations and their countries of origin and residence are also very heterogeneous, and regarding risk of mental illness, it can be erroneous to consider migrants as a uniform group [6]. Compared with labour and other types of migrants, refugees have a particularly increased risk of some mental disorders [7,8,9,10]. Therefore, the profile of the immigrant population, as well as the native population used as comparison may define the observed risk differences.
Many studies on migrants’ mental health have been carried out in Sweden and Denmark [11]. Finland, however, shows worse mental health than its neighbouring Nordic countries in many indicators, such as higher suicide rate and higher level of alcohol use and alcohol-related mortality [12, 13], and has a somewhat stricter humanitarian migration policy than some other Nordic countries [14,15,16]. Therefore, the findings and risk profile found in these studies may not be applicable in the Finnish context. These characteristics and the comprehensive Finnish register-based health information system provide a good setting for examining hypotheses regarding the risk of mental disorders among migrants.
Based on two existing studies on psychological symptoms, the Finnish immigrant population appears to have better mental health than native Finns, with some variation across immigrant groups [17]. Register-based studies have found a higher risk of ADHD [18] and autism [19], and a lower risk of Asperger’s syndrome [20] among children of immigrant parents living in Finland. However, these studies have not assessed psychotic symptoms, diagnoses of psychotic and mood disorders or post-traumatic stress disorder (PTSD), which have all shown an elevated risk among migrants [1, 2, 21].
This study aims at assessing incidence and prevalence of mental disorders among immigrants and Finnish-born controls in a register-based cohort study with a 4-year follow-up. This is the first large-scale study on psychiatric disorders among migrants in Finland. Based on earlier literature, we expect to find increased risk of some mental disorders, such as psychoses, mood disorders and PTSD.
Methods
This cohort study utilises Finnish registers to study prevalence and incidence of mental disorders treated in specialised psychiatric services among immigrants and Finnish-born controls. The study was approved by the Ethics Committee of the National Institute for Health and Welfare (THL) in Finland (589/2013). THL, The Central Population Register and Statistics Finland gave their permissions to use confidential register data in this study.
Sample
Immigrants were identified from the Finnish Central Population Register (FCPR), a national register of Finnish citizens and permanent residents in Finland. The register does not include temporary residents, such as asylum seekers or undocumented migrants. We identified persons who were born abroad, whose mother tongue is not Finnish, and who were at least 15 years old, alive and resident in Finland on 31st December 2010. For each immigrant, a Finnish-born control was identified from the FCPR and matched by background characteristics [22]. The controls were matched by age, so that they were born the same year and month as the migrant (if needed, this timeframe was extended by ±1 month); by place of residence (municipality) on 31st December 2010 and by gender. Additionally, the controls’ mother tongue had to be one of the official languages spoken in Finland (Finnish or Swedish), and they must not be adopted. In case several persons filled all criteria, the control was chosen randomly. The number of both immigrants and their Finnish-born controls was 185.605 leading to a total sample size of 371.210.
However, according to the FCPR, 799 immigrants (0.4%) and 421 controls (0.2%) in the sample had moved to Finland in 2011–2014. It was assumed that they had lived in Finland on 31st December 2010, emigrated without informing their leaving date, and then returned during the follow-up period. Because their actual residence could not be verified, they were omitted from the analyses.
Regional categorization
We categorised countries of birth into nine regions: (1) Finland, (2) Other Nordic countries, (3) Russia and former Soviet Union, (4) Other Western countries (members of the European Union (EU) and/or European Economic Area (EEA), Switzerland, USA, Canada, Australia and New Zealand), (5) Eastern Europe (former or current Eastern European countries that are not members of the EU), (6) North Africa and Middle East, (7) Sub-Saharan Africa, and (8) Asia. The number of immigrants from other countries (mostly Latin American countries and Pacific Islands) was small, so no separate category was formed for them, but they were included in the total number of immigrants. For 1134 foreign-born persons, information on country of birth was missing, but 1031 of them could be classified based on their mother tongue. Those whose mother tongue was unknown or geographically very widely spoken (English, French, Spanish and Portuguese) (n = 103) were excluded from the regional analyses.
Information on mortality
Information on time and causes of death during the follow-up (January 1st 2011 to December 31st 2014) was obtained from the national Causes of Death Register maintained by Statistics Finland. The Finnish system of death reporting is considered very reliable [23].
Outcome variables: mental disorders
Information on mental disorders was obtained from the Hospital Discharge Register, which covers all hospital inpatient care since 1967 and outpatient care in specialised services at the public sector in Finland since 1998, with the exception of a few cities that provide municipal psychiatric outpatient services. All psychiatric diagnoses (ICD-10 codes F00–F99) were included and analysed according to the following categorization: alcohol use disorders F10; other substance use disorders F11–F16 and F18–F19; non-affective psychotic disorders F20–F29; bipolar disorder F30–F31; major depressive disorder F32–F33; other mood disorders F34–F39; anxiety disorders F40–F42; post-traumatic stress disorder F43.1; dissociative and somatoform disorders F44–F45; eating disorders F50 and personality disorders F60.
In addition, information on diagnoses in primary care was obtained from the Care Register on outpatient visits in primary health care (AvoHILMO), where information was available from 2011 onwards. This register contains either ICD-10 or ICPC-2-codes diagnoses set by primary care physicians. Since primary care physicians have limited time and few psychiatric diagnostic tools available, these diagnoses were considered less reliable than those used in specialised health care by psychiatrists, and were not combined to those given in specialised care. They are reported in the category “Any psychiatric contact in primary care (F00–F99)”, including both ICD-10 codes F00–F99 and ICPC2-codes P01–P29 and P70–P99.
Covariates
Sociodemographic factors that were considered potential confounders or mediators and therefore included in the adjusted analyses were age, socioeconomic status (SES) and marital status. Information about age and marital status in the beginning of the study was provided by the FCPR and information about SES was obtained from Statistics Finland. Age was used as a five-categorical variable. Marital status was categorised into three groups: unmarried, married or in a registered partnership, and other (including those who were widowed, separated or divorced). The SES variable provided by Statistics Finland is based on occupation, main type of activity, job status, nature of work and stage in life. In this study, a five-categorical variable was used: entrepreneurs and farmers, upper white collar workers (such as leaders and experts), lower white collar workers (such as office workers), blue collar workers (manual work) and others (people not in employment such as students, homemakers and unemployed people) [24]. Information on education was unavailable for most immigrants, and therefore could not be used.
Statistical analysis
The Cox proportional hazards model was used to analyse risk differences between immigrants and Finnish-born controls in incidence of new-onset mental disorders in each diagnosis group. Participants were followed up from January 1st 2011 until emigration, death, first incidence of the psychiatric diagnosis in question, or 31st December 2014.
To be able to analyse incidence of new-onset disorders, a 4-year washout period was used: for each disorder category, persons who had received a diagnosis from this category during 2007–2010 were excluded from the incidence analysis for that particular category. The washout period was specific to each disorder category. Persons with multiple admissions for different diagnoses were included in the analyses for all the corresponding diagnostic categories.
Sensitivity analyses were carried out excluding those who migrated to Finland during the follow-back time 2007–2010, to account for the fact that the washout period in their case was incomplete.
Also, prevalence of disorders was analysed based on F00–F99 diagnoses received in years 2007–2010 among immigrants and controls. In these analyses, immigrants and native Finns who moved to Finland between 2007 and 2010 were excluded.
Unadjusted and analyses adjusted for available covariates were carried out, with Finnish-born controls as the reference group. Previous literature [25] and preliminary analyses pointed to significant variations in risk differences by sex, and thus incidence and prevalence analyses were carried out separately for men and women.
The proportional hazards assumption was tested on the basis of Schoenfeld residuals [26], and based on this, the covariates (age, marital status and socioeconomic status) were added to the models through stratification.
The results are presented as hazard ratios (HR) and prevalences with their 95% confidence intervals. Stata 14.2 was used for the analyses.
Results
Altogether 184.806 immigrants and 185.184 Finnish-born controls were followed up from 1.1.2011 to 31.12.2014, leading to a total of 1.412.117 person-years (700.243 person-years for immigrants and 718.874 for controls). Finnish-born controls are the reference group in all analyses. Descriptive statistics of the sample are presented in Supplementary Table 1.
Incidence of mental disorders
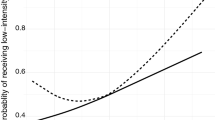
The incidence of any mental disorder was lower among immigrants in men (adjusted HR 0.82, 95% CI 0.77–0.87 in specialised care and aHR 0.90 (0.86–0.93) in primary care) and women (aHR 0.76, 95% CI 0.72–0.81 in specialised care and aHR 0.79, 95% CI 0.76–0.81 in primary care) (Tables 1, 2; Fig. 1a, b). The lowest incidence was observed among Asian immigrants (aHR 0.49, 95% CI 0.42–0.58 in men and aHR 0.47, 95% CI 0.41–0.53 in women), and the highest in immigrants from North Africa and Middle East (aHR 1.17, 95% CI 1.06–1.28 in men and aHR 1.30, 95% CI 1.17–1.45 in women).

Adjusted hazard ratios (aHR) for all mental disorders, major depressive disorder (MDD) and post-traumatic stress disorder (PTSD) according to region of origin in men and women* (*all hazard ratios adjusted for age, marital status and socioeconomic status)
The incidence of psychotic disorders among migrant men was not different than among Finnish men (aHR 0.92, 95% CI 0.79–1.08) and lower among migrant women (aHR 0.82, 95% CI 0.69–0.97). The incidence of bipolar disorders was considerably lower among immigrants (aHR 0.49, 95% CI 0.38–0.63 in men and aHR 0.29, 95% CI 0.24–0.37 in women). Depressive disorders were also less common among immigrants (aHR 0.82, 95% CI 0.75–0.90 in men and aHR 0.77, 95% CI 0.71–0.83 in women), except among immigrants from North Africa and Middle East, who had higher incidence than Finns (Fig. 1c, d).
PTSD was the only disorder where immigrant men had a higher incidence (aHR 4.88, 95% CI 3.38–7.05) and the risk of immigrant women did not differ from native Finns (aHR 1.03, 95% CI 0.81–1.32) (Fig. 1e, f). The incidence was particularly high among immigrants from Eastern Europe, North Africa and Middle East, and in the case of men, Sub-Saharan Africa and Asia. The largest differences in terms of effect size were observed for PTSD.
The incidence of alcohol use disorders (aHR 0.42, 95% CI 0.37–0.48 in men and aHR 0.40, 95% CI 0.34–0.48 in women) and other substance use disorders (aHR 0.73, 95% CI 0.61–0.88 in men and aHR 0.44, 95% CI 0.34–0.58 in women) was lower among immigrants. The difference to Finns was statistically significant in all immigrant groups except for Nordic immigrants.
There was no statistically significant difference in the incidence of dissociative and somatoform disorders and eating disorders among men, when adjusted for covariates, whereas in women the incidence of these disorders was also lower among immigrants (aHR 0.71, 95% CI 0.57–0.90% and 0.55, 95% CI 0.41–0.75%, respectively).
The results of the sensitivity analysis, excluding persons who had migrated into Finland between 2007 and 2010, did not have important differences from those reported here. Among men of North African and Middle Eastern origin and women from Nordic countries, the risk of any mental disorder did not significantly differ from the Finnish-born (HR 1.08, 95% CI 0.97–1.20% and 1.12, 95% CI 0.94–1.32, respectively), as opposed to the elevated risks reported as main results (Supplementary Tables 2-3).
Prevalence of mental disorders
The differences between immigrants and Finnish-born controls in the prevalence of different groups of mental disorders were of similar magnitude as in the incidence (Tables 3, 4). The prevalence of any mental disorder in 2007–2010 among immigrant men was 4.2% (95% CI 4.1–4.5) and among Finnish men 6.4% (95% CI 6.2–6.6). In women, the corresponding figures were 5.5% (95% CI 5.4–5.7) among immigrant women and 7.8% (95% CI 7.6–8.0) among Finnish women.
Nordic (6.4%, 95% CI 5.7–7.3) and Middle Eastern and North African men (6.5%, 95% CI 6.0–7.0) had a similar overall prevalence, and Nordic (9.5%, 95% CI 8.5–10.5) and Middle Eastern and North African women (9.5%, 95% CI 8.9–10.3) had a higher prevalence than the corresponding Finnish-born controls, whereas the other regions had lower prevalence rates of any mental disorder.
The prevalence rates reported are unadjusted and do not account for different age structures between the immigrant and control groups.
Discussion
This large register-based cohort study of incidence and prevalence of mental disorders among immigrants and the native population in Finland showed a generally lower risk of mental disorders among the immigrant population in Finland, and large risk differences by immigrant and disorder group.
The risk of any new-onset mental disorder was lower both among immigrant men (aHR 0.74–0.86) and women (aHR 0.76–0.78) compared with native Finns. This is in contrast to register studies from Sweden [27, 28] and the Netherlands [29], and systematic reviews [1, 2, 30], which have indicated higher incidence and prevalence rates of mental disorders among immigrants. However, in population surveys in the US, first-generation immigrants also had a lower rate of mood, anxiety and personality disorders, compared with native-born Americans [31, 32]. In Spain and Australia, no difference in psychiatric morbidity was found between local population and immigrants [33, 34], and in Canada, immigrants experienced less psychological distress [35]. Also in a Danish register-based study, first- and second-generation immigrants had an increased risk of psychotic disorders, but decreased risk of affective, personality and substance use disorders. The risk of any psychiatric contact was lower for second-generation immigrants and not different from native Danes for first-generation immigrants [11].
Psychotic and bipolar disorders
Among the most consistent findings in previous studies has been an elevated risk of psychotic disorders in first- and second-generation migrants, particularly African immigrants [1]. We failed to find an increased risk of psychotic or bipolar disorder in any of the migrant groups, and overall the risk of both psychotic and bipolar disorders was decreased in migrants compared to the Finnish controls. This unprecedented finding may be due to the high prevalence of psychotic disorders in Finland [36]. For example, the lifetime prevalence of schizophrenia in Finland was 1.0% in a general population survey [36], while the median lifetime prevalence in the world is 0.4% [37]. Moreover, the rate of psychosis among Finnish migrants in Sweden was among the highest in all migrant groups [28]. Although previous studies suggest that the relative incidence of psychotic disorders among immigrants increases as they form a decreasing proportion of the population [1], in Finland, where migrants constitute a small minority, their risk of psychosis does still not exceed that of the native Finns.
Depressive disorders
Immigrants had a lower incidence of major depressive disorder and other mood disorders compared with Finnish-born population. Persons of North African and Middle Eastern origin, however, had a higher risk, and Nordic and Eastern European immigrants had the same risk as Finns did, while immigrants of Russian, Sub-Saharan African and Asian origin had remarkably lower incidence of major depression.
A recent systematic review found a slightly increased risk of depressive disorders among both first- and second-generation migrants [2]. Proposed mechanisms include post-migratory stress, discrimination and isolation. Strong social networks could potentially mitigate this risk, an example being the ‘Latino paradox’ in the US [2]. Finland has relatively small immigrant communities, and it does not appear likely that strong social networks would explain the lower risk of depression in all migrant groups. However, the 12-month prevalence of major depressive disorder in Finland is 7.4%, slightly higher than the global average [38]. Studies from Denmark and the US have also found lower prevalence of depressive disorders and migrants [11, 31]. Globally, the North African and Middle Eastern region has a higher than average prevalence, whereas East Asian region has a lower prevalence [39]. The observed differences in incidence of depression by geographic groups appear to follow these patterns of countries of origin.
PTSD
In this study, post-traumatic stress disorder was the only disorder where immigrants had a higher risk than native Finns (aHR 5.4 for men and 1.4 for women). In particular, the risk of PTSD was increased among immigrants from Northern Africa and the Middle East, Sub-Saharan Africa and Eastern Europe. There were large differences by sex, with men having larger hazard ratios across the geographic groups. Women from Asia and Sub-Saharan Africa did not have an increased risk of PTSD, whereas men from these regions did. In terms of public health relevance, the largest risk differences between migrants and Finns were observed for PTSD, highlighting the need to develop psychosocial services to respond to the needs of immigrants from unstable societies [40].
Compared with other geographic areas, in Finland immigrants from these regions are more frequently refugees than labour migrants [17], and more likely to have been exposed to traumatic events. Globally, the risk of PTSD among refugees is up to tenfold compared with the general population [8], and particularly high among refugees from former Yugoslavia [10]. The gender difference observed in our study is likely related to different exposure to traumatic events: In another Finnish study, 82% of Kurdish men and 72% of Kurdish women living in Finland reported to have experienced a traumatic event, most often war-related [41]. Among Somali immigrants, however, the situation was reversed, with 44% of men and 68% of women reporting traumatic events. In the case of more severe traumatic experiences, the gender difference was wider: 9–33% of men vs. 3–6% of women reported to have experienced torture and 5–41% of men vs. 1–13% of women experienced imprisonment or kidnapping.
Alcohol use disorders
Immigrants as a group and all geographic area groups separately had a lower risk for alcohol use disorders (HR 0.1–0.7), with the exception of persons from Nordic countries. Incidence of other substance use disorders was also lower among both men and women (HR 0.4–0.7). Finland has a high level of alcohol consumption and alcohol use disorders, [42] whereas immigrants in Finland report much lower rates of alcohol consumption than the native population [17], and in a previous Finnish study, lower alcohol-related mortality explained a large share of the lower mortality among immigrants [5]. Similar findings of lower alcohol use disorder prevalence have been reported from the Netherlands and the US [43, 44].
Other mental disorders
The incidence of dissociative and somatoform disorders, which can also be trauma-related [45], did not differ between immigrant and Finnish men, whereas immigrant women had a lower risk. Incidence of anxiety, eating and personality disorders was lower among immigrants. Eating disorders among men were too rare to make meaningful conclusions. In the case of personality disorders, language and cultural barriers as well as lack of information about earlier medical history could influence the low rate of diagnosing these disorders.
Geographic differences
Looking at the geographic categories of immigrants, persons from Nordic countries appear to have a very similar risk as Finns for most disorders, and among women in total a slightly elevated total risk (HR 1.19), whereas among men their risk of psychotic disorders is significantly lower than Finns. This is in line with earlier findings of high psychosis rates among Finnish migrants in Sweden [46]. The largest differences compared with the native population are observed among people of Asian, African and Middle Eastern origin. In these categories, persons from North Africa and Middle East have a higher incidence of all mental disorders than Finns among both men and women, but with large inter-category variations, such that the risk of PTSD, dissociative and somatoform disorders and major depression is increased, whereas the risk of other mental disorders is decreased. People of Asian and Sub-Saharan origin have lower incidence rates overall, with the exception of PTSD in men.
As mentioned above, immigrants from Africa and the Middle East more often have a refugee background than other immigrant groups in Finland: approximately one-third in this group are refugees [17]. However, across groups, family-related reasons, which include refugee family reunification, are the most important reason for migration to Finland (42–67% of migrants in each group). Unfortunately, refugee status is not recorded in the Finnish Central Population Register, so it was not possible to carry out further analyses regarding the impact of refugee status.
Comparison to earlier migrant studies in Finland
Only two recent studies provide information on the mental health of the adult Finnish immigrant population [17, 41]. The Migrant Health and Wellbeing Study interviewed 1846 immigrants of Russian, Somali and Kurdish origin. Using the Hopkins Symptom Checklist (HSCL-25), Russian and Kurdish immigrants reported a high level of psychological symptoms (18 and 36%, respectively, reported severe depressive and anxiety symptoms during the last week), whereas Somali immigrants’ symptom level (8.7%) did not differ from the Finnish general population (8.6%) [41]. Socioeconomic disadvantage, more recent migration and lower language proficiency were associated with more psychological symptoms [25].
In the Survey on Work and Well-being among People of Foreign Origin, including immigrants of varying nationalities, self-reported mental disorder was not more common among immigrants than among the Finnish population, and psychological distress as measured by the Mental Health Index (MHI-5) was less common. Many indicators of wellbeing, such as trust in strangers and the health care system, happiness in the past month or receiving support from neighbours were better compared to the Finnish population across immigrant groups. However, immigrants from North Africa and the Middle East reported significantly higher levels of psychological distress and self-reported psychiatric disorder than Finns [17].
Our results are in line with these studies: immigrants as a group appear to have better mental health than Finns, but some groups, particularly those originating from Africa and Middle East, show worse mental health indicators.
Why do immigrants have better mental health than Finns?
Some possible explanations to our findings emerge from the literature. Many studies have found refugees to be at a higher risk of mental disorders than other types of migrants [7,8,9]. Finland has a relatively restrictive humanitarian migration policy compared with Scandinavian countries [47, 48], and most migrants are either labour migrants or migrated due to personal, family-related reasons, and therefore subject to selective migration. This may explain the notable differences to the findings of neighbouring Sweden, which has been known for its liberal and humanitarian migration policies [7, 48]. On the other hand, Finnish integration policy is characterised as ‘multicultural’ or tolerant, and therefore beneficial to migrant health [49].
However, also methodological considerations related to the use of registers may influence our findings. This study is based on register data from all public health services, which in Finland constitute a large majority of all health care use. Nevertheless, this approach does not consider two groups: those using only private services, and those who do not seek health services. Regarding the use of private services, it is less likely that immigrants would use them more than the Finnish-born, since majority of these services are occupational health services, and unemployment rates among immigrants are higher than native Finns. Therefore, our findings of mostly lower incidence and prevalence are probably not influenced by differences in the use of private and public health services.
The second group, those who do not use mental health services at all, is more problematic. Access and pattern of use of mental health services could differ between migrants and local populations [21, 50]. Since Finland has a universal health care system, all legal migrants have in principle access to the same services as the native population. However, utilisation of services at different levels of health care might still differ. In one Finnish study, the use of specialised mental health services did not differ between immigrants and the general population, with the exception of Kurdish women, who used these services more frequently [51]. However, we cannot exclude the influence of different patterns of health service use on our results. Nevertheless, the observed differences in the incidence of any mental disorder between specialised and primary mental health care were small.
Another suggested explanation for the higher incidence of psychosis among migrants found in previous studies is misdiagnosis. Even though there is some evidence that there might be diagnostic challenges in particular in schizophrenia [52], this is unlikely to explain the frequently observed increased risk of psychosis to a meaningful extent [3]. No culturally specific diagnostic procedures are used in Finland, and there is very little training on cultural competence in health care. It is possible that some psychiatric problems are misdiagnosed, if large cultural differences exist between patients and the Finnish health care professionals. Also, under diagnosis related to communication problems is possible and is another potential contributor to the observed lower rates of mental disorders.
Limitations
In addition to the methodological challenges related to register studies mentioned above, particularly the fact that it was not possible to assess those who have not accessed health services, one additional limitation is the follow-up time and the washout period. Some studies have been able to follow persons from early adolescence, but since the migrant population in Finland is recent, this approach would have resulted in a small sample size. Finally, the FCPR includes only residents in Finland, and therefore asylum seekers and undocumented migrants were not included, even though they might be a particularly vulnerable migrant group.
Conclusion
We found a lower risk of mental disorders among the immigrant population in Finland, with notable differences by immigrant and disorder group. The region of origin significantly influenced the risk of specific mental disorders. Particularly, the risk of PTSD varied according to region of origin of the migrants. The Finnish migrant profile and relatively high psychiatric morbidity of Finns contribute to these findings, which are radically different from many earlier migrant studies. It is vital to understand the heterogeneity of migrant populations, and also of the native comparison populations. Instead of trying to decipher the overall risk of all mental disorders across all migrant groups, it can be much more valuable to study specific risks in specific groups.
References
Bourque F, van der Ven E, Malla A (2011) A meta-analysis of the risk for psychotic disorders among first- and second-generation immigrants. Psychol Med 41(5):897–910. doi:10.1017/S0033291710001406
Mindlis I, Boffetta P (2017) Mood disorders in first- and second-generation immigrants: systematic review and meta-analysis. Br J Psychiatry 210(3):182–189. doi:10.1192/bjp.bp.116.181107
Morgan C, Charalambides M, Hutchinson G, Murray RM (2010) Migration, ethnicity, and psychosis: toward a sociodevelopmental model. Schizophr Bull 36(4):655–664. doi:10.1093/schbul/sbq051
Wallace M, Kulu H (2014) Low immigrant mortality in England and Wales: a data artefact? Soc Sci Med (1982) 120:100–109. doi:10.1016/j.socscimed.2014.08.032
Lehti V, Gissler M, Markkula N, Suvisaari J (2016) Mortality and causes of death among the migrant population of Finland in 2011–2013. Eur J Public Health. doi:10.1093/eurpub/ckw196
Lindert J, Schouler-Ocak M, Heinz A, Priebe S (2008) Mental health, health care utilisation of migrants in Europe. Eur Psychiatry 23(Suppl 1):14–20. doi:10.1016/s0924-9338(08)70057-9
Hollander AC, Dal H, Lewis G, Magnusson C, Kirkbride JB, Dalman C (2016) Refugee migration and risk of schizophrenia and other non-affective psychoses: cohort study of 1.3 million people in Sweden. BMJ (Clin Res) 352:i1030. doi:10.1136/bmj.i1030
Fazel M, Wheeler J, Danesh J Prevalence of serious mental disorder in 7000 refugees resettled in western countries: a systematic review. The Lancet 365(9467):1309-1314. doi:10.1016/S0140-6736(05)61027-6
Lindert J, Ehrenstein OSV, Priebe S, Mielck A, Brähler E (2009) Depression and anxiety in labor migrants and refugees—a systematic review and meta-analysis. Soc Sci Med 69(2):246–257. doi:10.1016/j.socscimed.2009.04.032
Bogic M, Njoku A, Priebe S (2015) Long-term mental health of war-refugees: a systematic literature review. BMC Int Health Hum Rights 15:29. doi:10.1186/s12914-015-0064-9
Cantor-Graae E, Pedersen CB (2013) Full spectrum of psychiatric disorders related to foreign migration: a Danish population-based cohort study. JAMA Psychiatry 70(4):427–435. doi:10.1001/jamapsychiatry.2013.441
Tuori T, Gissler M, Wahlbeck K; the Nordic Reference Group (2007) Mental health in the Nordic countries. In: Health Statistics in the Nordic Countries 2005/Helsestatistik for de nordiske lande 2005. Nordic Medico-Statistical Committee (NOMESCO), Copenhagen
OECD (2017) Suicide rates (indicator). doi:10.1787/a82f3459-en. Accessed 3 July 2017
The Finnish Immigration Service (2016) Statistics on residence permits. http://www.migri.fi/about_us/statistics/statistics_on_residence_permits. Accessed 5 June 2017
The Finnish Immigration Service (2014) Statistics, 2014. http://www.migri.fi/about_us/statistics. Accessed 5 June 2017
Nieminen T, Sutela H, Hannula U (2015) Ulkomaista syntyperää olevien työ ja hyvinvointi 2014 [Survey on work and well-being among persons of foreign origin in 2014]. Statistics Finland. https://www.stat.fi/tup/julkaisut/tiedostot/julkaisuluettelo/yyti_uso_201500_2015_16163_net.pdf. Accessed 15 June 2017
Castaneda A, Jokela S, Koponen P, Pentala O, Koskela T, Koskinen S (2014) Ulkomaista syntyperää olevien työ ja hyvinvointi -tutkimuksen perustulokset [Baseline Report of the Migrant Health and Wellbeing Study]. https://www.terveytemme.fi/uth. Accessed 15 June 2017
Lehti V, Chudal R, Suominen A, Gissler M, Sourander A (2016) Association between immigrant background and ADHD: a nationwide population-based case-control study. J Child Psychol Psychiatry 57(8):967–975. doi:10.1111/jcpp.12570
Lehti V, Hinkka-Yli-Salomäki S, Cheslack-Postava K, Gissler M, Brown AS, Sourander A (2013) The risk of childhood autism among second-generation migrants in Finland: a case–control study. BMC Pediatr 13:171. doi:10.1186/1471-2431-13-171
Lehti V, Cheslack-Postava K, Gissler M, Hinkka-Yli-Salomaki S, Brown AS, Sourander A (2015) Parental migration and Asperger’s syndrome. Eur Child Adolesc Psychiatry 24(8):941–948. doi:10.1007/s00787-014-0643-7
Giacco D, Matanov A, Priebe S (2014) Providing mental healthcare to immigrants: current challenges and new strategies. Curr Opin Psychiatry 27(4):282–288. doi:10.1097/yco.0000000000000065
Rubin DB (1973) Matching to remove bias in observational studies. Biometrics 29(1):159–183. doi:10.2307/2529684
Lahti RA, Penttilä A (2001) The validity of death certificates: routine validation of death certification and its effects on mortality statistics. Forensic Sci Int 115(1–2):15–32
Statistics Finland (1989) Classification of socioeconomic groups. Handbooks 17. https://www.stat.fi/meta/luokitukset/sosioekon_asema/001-1989/kasikirja.pdf. Accessed 14 July 2017
Rask S, Suvisaari J, Koskinen S, Koponen P, Molsa M, Lehtisalo R, Schubert C, Pakaslahti A, Castaneda AE (2016) The ethnic gap in mental health: a population-based study of Russian, Somali and Kurdish origin migrants in Finland. Scand J Public Health 44(3):281–290. doi:10.1177/1403494815619256
Grambsch PM, Therneau TM (1994) Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 81:515–526
Hollander AC, Bruce D, Burstrom B, Ekblad S (2013) The association between immigrant subgroup and poor mental health: a population-based register study. J Nerv Ment Dis 201(8):645–652. doi:10.1097/NMD.0b013e31829dbd64
Westman J, Johansson LM, Sundquist K (2006) Country of birth and hospital admission rates for mental disorders: a cohort study of 4.5 million men and women in Sweden. Eur Psychiatry 21(5):307–314. doi:10.1016/j.eurpsy.2006.02.001
Selten JP, Laan W, Kupka R, Smeets HM, van Os J (2012) Risk of psychiatric treatment for mood disorders and psychotic disorders among migrants and Dutch nationals in Utrecht, The Netherlands. Soc Psychiatry Psychiatr Epidemiol 47(2):271–278. doi:10.1007/s00127-010-0335-7
Bas-Sarmiento P, Saucedo-Moreno MJ, Fernández-Gutiérrez M, Poza-Méndez M (2017) Mental health in immigrants versus native population: a systematic review of the literature. Arch Psychiatr Nurs 31(1):111–121. doi:10.1016/j.apnu.2016.07.014
Salas-Wright CP, Kagotho N, Vaughn MG (2014) Mood, anxiety, and personality disorders among first and second-generation immigrants to the United States. Psychiatry Res 220(3):1028–1036. doi:10.1016/j.psychres.2014.08.045
Breslau J, Aguilar-Gaxiola S, Borges G, Kendler KS, Su M, Kessler RC (2007) Risk for psychiatric disorder among immigrants and their US-born descendants: evidence from the National Comorbidity Survey Replication. J Nerv Ment Dis 195(3):189–195. doi:10.1097/01.nmd.0000243779.35541.c6
Qureshi A, Collazos F, Sobradiel N, Eiroa-Orosa FJ, Febrel M, Revollo-Escudero HW, Andrés E, del Mar Ramos M, Roca M, Casas M, Serrano-Blanco A, Escobar JI, García-Campayo J (2013) Epidemiology of psychiatric morbidity among migrants compared to native born population in Spain: a controlled study. Gen Hosp Psychiatry 35(1):93–99. doi:10.1016/j.genhosppsych.2012.09.010
Sharma S (2012) Psychological distress among Australians and immigrants: findings from the 2007 National Survey of Mental Health and Wellbeing. Advances in Mental Health 10(2):106–116. doi:10.5172/jamh.2011.10.2.106
Setia MS, Quesnel-Vallee A, Abrahamowicz M, Tousignant P, Lynch J (2012) Different outcomes for different health measures in immigrants: evidence from a longitudinal analysis of the national population health survey (1994–2006). J Immigr Minor Health 14(1):156–165. doi:10.1007/s10903-010-9408-7
Perälä J, Suvisaari J, Saarni SI, Kuoppasalmi K, Isometsä E, Pirkola S, Partonen T, Tuulio-Henriksson A, Hintikka J, Kieseppä T, Härkänen T, Koskinen S, Lönnqvist J (2007) Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch Gen Psychiatry 64(1):19–28. doi:10.1001/archpsyc.64.1.19
Saha S, Chant D, Welham J, McGrath J (2005) A systematic review of the prevalence of schizophrenia. PLoS Med 2(5):e141. doi:10.1371/journal.pmed.0020141
Markkula N, Suvisaari J, Saarni SI, Pirkola S, Pena S, Saarni S, Ahola K, Mattila AK, Viertio S, Strehle J, Koskinen S, Härkänen T (2015) Prevalence and correlates of major depressive disorder and dysthymia in an eleven-year follow-up-results from the Finnish Health 2011 Survey. J Affect Disord 173:73–80. doi:10.1016/j.jad.2014.10.015
Ferrari AJ, Somerville A, Baxter AJ, Norman RE, Patten SB, Vos T, Whiteford HA (2013) Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychol Med 43(3):471–481
Lehti V, Antas B, Kärnä T, Tuisku K (2016) The assessment of traumatized refugees: clinical practices at the cultural psychiatry outpatient clinic. Psychiatria Fennica 47:17–31
Castaneda AE, Rask S, Koponen P, Mölsä M, Koskinen S (2012) Maahanmuuttajien terveys ja hyvinvointi - Tutkimus venäläis-, somalialais- ja kurditaustaisista Suomessa [Migrant Health and Wellbeing - Study of persons of Russian, Somali and Kurdish origin in Finland]. vol 61/2012. Tampere
WHO (2014) Global status report on alcohol and health 2014. Luxemburg. http://www.who.int/substance_abuse/publications/global_alcohol_report/en/. Accessed 15 June 2017
Selten JP, Wierdsma A, Mulder N, Burger H (2007) Treatment seeking for alcohol and drug use disorders by immigrants to the Netherlands: retrospective, population-based, cohort study. Soc Psychiatry Psychiatr Epidemiol 42(4):301–306. doi:10.1007/s00127-007-0162-7
Salas-Wright CP, Vaughn MG, Clark TT, Terzis LD, Cordova D (2014) Substance use disorders among first- and second- generation immigrant adults in the United States: evidence of an immigrant paradox? J Stud Alcohol Drugs 75(6):958–967
Roelofs K, Spinhoven P (2007) Trauma and medically unexplained symptoms towards an integration of cognitive and neuro-biological accounts. Clin Psychol Rev 27(7):798–820. doi:10.1016/j.cpr.2007.07.004
Leao TS, Sundquist J, Frank G, Johansson LM, Johansson SE, Sundquist K (2006) Incidence of schizophrenia or other psychoses in first- and second-generation immigrants: a national cohort study. J Nerv Ment Dis 194(1):27–33. doi:10.1097/01.nmd.0000195312.81334.81
World Bank (2017) Refugee population by country or territory of asylum. http://data.worldbank.org/indicator/SM.POP.REFG. Accessed 5 June 2017
Eurostat (2017) First instance decisions by outcome and recognition rates, 4th quarter 2016. http://ec.europa.eu/eurostat/statistics-explained/index.php/File:First_instance_decisions_by_outcome_and_recognition_rates,_4th_quarter_2016.png. Accessed 18 April 2017
Malmusi D (2015) Immigrants’ health and health inequality by type of integration policies in European countries. Eur J Pub Health 25(2):293–299. doi:10.1093/eurpub/cku156
Gil-Gonzalez D, Carrasco-Portino M, Vives-Cases C, Agudelo-Suarez AA, Castejon Bolea R, Ronda-Perez E (2015) Is health a right for all? An umbrella review of the barriers to health care access faced by migrants. Ethnicity Health 20(5):523–541. doi:10.1080/13557858.2014.946473
Koponen P, Rask S, Skogsberg N, Castaneda A, Manderbacka K, Suvisaari J, Kuusio H, Laatikainen T, Keskimäki I, Koskínen S (2016) Suomessa vakituisesti asuvat maahanmuuttajat käyttävät vaihtelevasti terveyspalveluja. Suomen Lääkärilehti 71:907–914
Zandi T, Havenaar JM, Laan W, Kahn RS, van den Brink W (2011) Predictive validity of a culturally informed diagnosis of schizophrenia: a 30 month follow-up study with first episode psychosis. Schizophr Res 133(1–3):29–35. doi:10.1016/j.schres.2011.09.024
Acknowledgements
We are very grateful to Dr. Sebastián Peña for assistance with the graphic design of the figures.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Funding
The study was financially supported by Jalmari and Rauha Ahokas Foundation, the Finnish Psychiatric Association, Emil Aaltonen Foundation and Helsinki University Hospital Research Funds.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

{kind=link}
Cite this article
Markkula, N., Lehti, V., Gissler, M. et al. Incidence and prevalence of mental disorders among immigrants and native Finns: a register-based study. Soc Psychiatry Psychiatr Epidemiol 52, 1523–1540 (2017). https://doi.org/10.1007/s00127-017-1432-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-017-1432-7