
Abstract
Purpose
Males feature prominently in suicide statistics, but relatively little work has been done to date to explore whether endorsement of dominant masculinity norms heightens the risk of or is protective against suicidal thinking. This paper aimed to further knowledge in this area.
Methods
We used baseline data from 13,884 men (aged 18–55) in the Australian Longitudinal Study on Male Health (Ten to Men) cohort. These men filled in self-complete questionnaires in 2013/14 which covered a range of topics, including conformity to dominant masculinity norms and suicidal thinking. We conducted logistic regression analyses to estimate the strength of association between these two variables.
Results
After controlling for other key predictors of suicidal thinking, one characteristic of dominant masculinity—self-reliance—stood out as a risk factor for suicidal thinking (AOR 1.34; 95% CI 1.26–1.43).
Conclusions
It suggests that one particular element of dominant masculinity—being self-reliant—may place men at increased risk of suicidal thinking. This finding resonates with current theories of how suicidal thinking develops and leads to action. It also has implications for the full gamut of suicide prevention approaches that target males in clinical settings and in the general population, and for our broader society. Further work is needed, however, to confirm the direction of the relationship between self-reliance and suicidality, and to unpack the means through which self-reliance may exert an influence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Internationally, suicide statistics are dominated by males. In high income countries the age-standardised male to female ratio is 3.5:1, and in low and middle income countries it is 1.6:1 [1]. Various explanations for the excess suicide rate among males have been proffered, including that males choose more lethal suicide means [2], are more reluctant to seek help [3], and are heavier users of drugs and alcohol [4]. In addition, males and females are known to react differently to stressful life events, with males being more likely to withdraw, respond aggressively and/or experience depressive symptoms, particularly in the face of events like divorce/separation and work problems [5, 6]. All of these explanations are fairly crude, and there is usually no attempt to examine what might sit behind them. Further exploration is required to determine whether there are particular factors related to masculinity that may lead to suicidal thinking and influence resultant choices and behaviours, contributing to the gender imbalance.
Masculinity is not a homogenous, universal construct; rather there are multiple masculinities. These vary across and within time and place. However, it is possible to identify certain characteristics that might be ascribed to a view of masculinity that is arguably still dominant, at least in many Western societies [7]. Such characteristics include stoicism, invulnerability, strength, independence, ability to provide for a family, drive, a “go-getter” attitude, and success in chosen endeavours. These characteristics can be positive and adaptive in many ways, but may also contribute to behaviours and cognitions that increase suicide risk [7]. For example, high levels of stoicism might be associated with a reluctance to seek help. This dominant masculinity is an important lens through which males make other decisions [8]. For example, studies in Australia—where the model of dominant masculinity embodies the above characteristics—have shown that men who conform to dominant masculine norms are more likely to engage in health risk behaviours and less likely to engage in health promotion behaviours [9]. Given this, it makes sense that dominant masculine norms could also influence the course of action males might take in a suicidal crisis.
Relatively few empirical studies have been conducted in this area, but those that have been done provide at least some indicative support for the above argument. Qualitative studies have suggested that threats to masculinity (e.g., loss of the role of breadwinner or household head) are associated with depression and suicidality [10, 11], and that males who experience suicidal thoughts often employ “typically masculine” strategies, like “toughing it out” [7, 12, 13], or using drugs and alcohol as a form of escape [7, 11]. Some quantitative studies have found positive associations between adherence to masculine norms and suicidal thoughts and behaviours in males from the general population [2, 14, 15] and from particular at-risk groups [16].
It should be noted here that some conflicting results have been found too. For example, one qualitative study involving focus groups and interviews with men who had experienced depression found that not all of them identified with dominant ideals of masculinity, and this influenced the strategies they employed to cope with their depression [13]. Similarly, one quantitative study found that low conformity to masculine norms was associated with suicides in a military population [17]. Overall, the question of how characteristics of dominant masculinity might increase, or protect against, suicidal thoughts and behaviours has been under-researched.
We had the opportunity to contribute further to knowledge about the relationship between endorsement of dominant masculine norms and suicidal thoughts because of our involvement in the largest all-male, nationwide cohort study to be conducted anywhere in the world—the Australian Longitudinal Study on Male Health, better known as Ten to Men. Using data from Ten to Men, we were able to explore whether particular elements of dominant masculinity heighten the risk of or are protective against suicidal thinking.
Method
Data source
We used data from the 13,884 18–55 year old men who participated in the baseline wave (Wave 1) of Ten to Men to investigate the relationship masculinity and suicidality. The procedures and materials used in Ten to Men have been described in detail elsewhere [18] and additional information can be found on the study’s website (http://www.tentomen.org.au/). A brief summary is provided here.
The Ten to Men cohort was recruited in 2013/14 using a stratified, multi-stage, cluster random sampling strategy in which the primary unit of sampling was the household. We approached all 104,884 households in 622 randomly selected statistical areas (SA1 s, which have boundaries defined by the Australian Bureau of Statistics and average populations of about 400 individuals). We were able to make contact with 81,400 (78%) of these households and 33,724 (32%) were identified as having at least one in-scope resident (a male aged between 10 and 55). We identified 45,510 in scope males in these households, and 15,988 (35%) of these returned useable data, providing representation from all Australian states and territories and from major cities and inner and outer regional areas. The response fraction for the restricted age range considered in the current paper (18–55 years) was 36%.
The males in the Ten to Men cohort provided information in five broad domains (physical health, mental health and wellbeing, health behaviours, social determinants of health, and health service utilisation and health knowledge). The cohort provided this information via self-complete questionnaires (except for its youngest members who did so via interview and parent-completed questionnaires).
It is important to reiterate here that the current analysis used data from Wave 1 of Ten to Men, and is, therefore, cross-sectional in nature. We have now completed data collection for Wave 2 and these data will be available for analysis in early 2017.
Primary outcome
Our primary outcome was a single item taken from the Patient Health Questionnaire (PHQ-9) [19] which asks “Over the past two weeks, how often have you been bothered by thoughts that you would be better off dead, or of hurting yourself in some way?” Like the other questions on the PHQ-9, this is scored 0 (“not at all”), 1 (“several days”), 2 (“more than half the days”) or 3 (“nearly every day”). We deemed those who scored 1 or more to be experiencing suicidal ideation.
Main predictor variables
Our main predictor variables were a set of factors identified as being characteristic of dominant masculinity. These were assessed by the Conformity to Masculine Norms Inventory (CMNI-22), which is an abbreviated version of the original 94-item CMNI that was designed to measure cognitive, behavioural and affective conformity to dominant masculine ideologies [20].
The CMNI-22 asks respondents to think about their own actions, feelings and beliefs and indicate how much they personally agree or disagree with each of 22 statements which are scored from 0 (“strongly disagree”) to 3 (“strongly agree”). Pairs of statements correspond to 11 factors: (1) work; (2) dominance; (3) risk-taking; (4) heterosexual presentation; (5) power over women; (6) emotional control; (7) Playboy; (8) violence; (9) pursuit of status; (10) winning; and (11) self-reliance. Examples of factors and items include:
-
Work
-
“My work is the most important part of my life” (Item 1)
-
“I don’t like giving all my attention to work” (Item 14, reverse scored)
-
-
Emotional control
-
“I like to talk about my feelings” (Item 6, reverse scored)
-
“I tend to share my feelings” (Item 10, reverse scored)
-
-
Violence
-
“I believe that violence is never justified” (Item 9, reverse scored)
-
“Sometimes violent action is necessary” (Item 13).
-
Each factor is scored from 0 (lowest conformity) to 6 (highest conformity), and a total score from 0 to 66 can also be calculated.
When the original 94-item instrument was developed it was shown to have good internal consistency, construct validity and discriminant validity [20]. The 22-item instrument, which uses the two highest loading items for each of the 11 factors on the parent instrument, demonstrates excellent concurrent validity, correlating well with the original instrument [21] and other recognised measures of masculinity like the Gender Role Conflict Scale, the Brannon Masculinity Scale and the Masculine Gender Role Stress Scale [22]. There are suggestions, however, that the factor scores are more meaningful than the total score [23]. Both the 94-item and the 22-item CMNI were positively regarded by the authors of a recent review of instruments designed to capture masculinity ideologies, who noted that it has been widely used [21].
Covariates
We also examined the influence of a number of socio-demographic and clinical covariates, largely selecting these on the basis that they have been shown in previous studies to be associated with suicidal ideation in males. These included age, marital status, region of residence, socioeconomic status, employment status, social support, stressful life events, alcohol use, depression, and general practitioner (GP) use. The way in which each of these was operationalised is described below.
Age was dichotomised (18–34; 35–55), as were marital status (married/de facto; never married/widowed/divorced/separated) and employment status (employed or not looking for work/unemployed). Socio-economic status was ascribed to participants on the basis of their area of residence, using quintiles from the Index of Relative Socioeconomic Disadvantage (IRSD) [24]. Region of residence was defined using the Remoteness Area classification of the Australian Statistical Geography Standard (ASGS) and included major cities, inner regional areas and outer regional areas [25].
Social support was assessed via the emotional/informational support sub-scale of the Medical Outcomes Survey Social Support Survey (MOS-SS) which yields a scaled score from 0 to 100, with higher scores indicating greater social support [26]. Exposure to specific stressful life events over the past 12 months was ascertained using a checklist of 24 events, largely based on a modified version of the Social Readjustment Scale [27] used in the Australian Longitudinal Study of Women’s Health [28]. For this study, we included only the six life events that we had found to be significantly associated with suicidality in a previous analysis of Ten to Men data [29], namely: serious personal injury, illness or surgery; break-up of a serious relationship/divorce/separation; serious conflict with a family member; difficulty finding a job; legal troubles or involvement in a court case; and major loss or damage to personal property. The stressful life events variable was dichotomised (any stressful life event/no stressful life events).
Alcohol use was measured by the Alcohol Use Disorders Identification Test (AUDIT) [30], which allowed us to classify participants’ alcohol use as harmful/hazardous or not. The self-reported presence or absence of depression was determined by a two questions that were part of a broader set on a range of disorders based on the Australian Health Survey [31] format and elicited “yes” or “no” responses. The first of these asked, “Has a doctor or other health professional ever told you that you had depression?” The second was worded, “Have you been treated for or had any symptoms of depression in the past 12 months?” We deemed those who answered “yes” to the latter question to have experienced depression in the past 12 months.
GP use was classified according to whether the participant indicated he had visited a GP in the past 12 months.
Analysis
We summarised variables descriptively using frequencies, percentages and means (and standard deviations). We then conducted univariate and multivariate logistic regression analyses to estimate the strength of association between the 11 masculinity factors and suicidal ideation, in each case controlling for the effects of the alternative masculinity factors and each of the other covariates and adopting p < 0.01 as our criterion for statistical significance. We reported the results of the regression analyses as unadjusted and adjusted odds ratios.
We also did a series of sensitivity analyses to see whether our findings held under a variety of circumstances. In some cases, these employed identical analytic approaches to the primary analyses, but used different combinations of variables. In other cases, they involved transforming the CMNI scores into dichotomous variables.
All data were analysed using Stata (Version 13.1) [32].
Results
Primary analyses
The 13,884 men who were the focus of our analysis had a mean age of 38.1 (SD 10.6). These men were varied in terms of where they lived, with 58.2% coming from metropolitan areas, 22.7% from inner regional areas and 19.1% from outer regional areas.Footnote 1 They were evenly split across advantaged and disadvantaged areas, with around 20% living in areas from each of the quintiles of relative disadvantage assessed by the IRSD. The majority (91.6%) were employed or not looking for work, and 66.9% were married or in a de facto relationship. On average, they had relatively high levels of social support, with a mean score on the emotional/informational support sub-scale of the MOS-SS of 70.8 (SD 25.3).
Two-fifths (41.1%) of the men in the study sample had experienced at least one of the identified stressful life events in the previous 12 months. Suicidal thinking, mental health problems and alcohol misuse were not uncommon among these men. Just under one tenth (9.5%) reported that they had been bothered by thoughts that they would be better off dead, or of hurting themselves in some way on several days or more of the previous two weeks. More than one tenth (12.8%) reported that they had been treated for or had symptoms of depression in the past 12 months and more than one-third (39.1%) met criteria for harmful/hazardous alcohol use.
Table 1 indicates how the men scored on the CMNI-22. As a group, their overall scores showed they were “average” in terms of conformity to masculine norms (mean 30.1; SD 4.7], in the sense that they scored close to the mid-point in terms of their total scores [33]. However, there was considerable across-factor variability in their scores. They showed below average conformity on some factors [e.g., Playboy (mean 1.6; SD 1.3)] but above average on others [e.g., Risk-taking (mean 3.5; SD 1.2)].
Table 2 shows the results of the logistic regression analysis. In the univariate analysis, the masculinity factors of playboy, pursuit of status and self-reliance conferred risk for suicidal thinking, and risk-taking and emotional control were protective against it. After controlling for each of the other factors on the CMNI-22 and for the other covariates, only one masculinity factor remained significant, namely self-reliance (AOR 1.34; 95% CI 1.26–1.48).
As anticipated, all of the covariates were statistically significant in the univariate analysis, and a number also were in the multivariate analysis. These were not being married or in a de facto relationship (AOR 1.41; 95% CI 1.20–1.66), experiencing a key life event in the previous 12 months (AOR 1.88; 95% CI 1.60–2.20), using alcohol at harmful/hazardous levels (AOR 1.41; 95% CI 1.22–1.63), and having experienced symptoms of depression in the previous 12 months (AOR 4.73; 95% CI 4.04–5.53). Residing in an area of the least socio-economic disadvantage was protective (AOR 0.73; 95% CI 0.57–0.94), as was having relatively high levels of social support (AOR 0.98; 95% CI 0.98–0.98).
Sensitivity analyses
We conducted various sensitivity analyses which are summarised here. We were concerned that that controlling for each of the other 10 masculinity factors when we examined a given factor on the CMNI might be refining out error variance, rather than (as intended) picking up a true signal of the unique effect of that factor. For this reason, our first sensitivity analysis only controlled for the socio-demographic and clinical covariates, and not the residual masculinity factors. This had no bearing on the findings; self-reliance remained the only masculinity factor that was associated with suicidal thinking (AOR 1.34; 95% CI 1.26–1.42).
We also felt that it was important to determine whether the total CMNI score was related to suicidal thinking, although this would have been unlikely given that only one of the factors stood out as being significant. In our second sensitivity analysis, we replaced the 11 individual factors with the total score and found that it was not significantly associated with suicidal thinking (AOR 1.02; 95% CI 1.00–1.03).
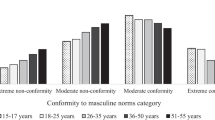
Finally, we dichotomised the CMNI factor scores to facilitate comparisons between the predictive strength of these and the covariates. We converted the raw factor scores into transformed scores (T-scores) using a mean of 50 and a standard deviation of 10, in line with a method outlined by the instrument’s developers [34]. We then treated T-scores above 50 as reflecting conformity or extreme conformity, and T-scores of 50 or below as reflecting non-conformity or extreme non-conformity. Using these dichotomised factor scores, self-reliance remained the only factor that was significantly associated with suicidal thinking (AOR 1.76; 95% CI 1.51–2.05). When we treated T-scores above 75 as reflecting extreme conformity, the same finding was true; self-reliance alone stood out (AOR 1.77; 95% CI 1.52–2.07).
Discussion
This study set out to explore whether conformity with particular elements of dominant masculinity increases (or decreases) the risk of suicidal thinking. We found that even after controlling for other predictors of suicidal thinking, one key masculine characteristic—self-reliance—stood out as a risk factor. This very specific finding extends the existing knowledge that is emerging from other studies of masculinity and suicidal thoughts and behaviours [2, 7, 10–17]. These other studies are relatively few in number, and have generally not “unpacked” the construct of dominant masculinity to consider the relevance of particular characteristics.
Self-reliance and suicidal thinking
Self-reliance is obviously a good quality in the right circumstances, but it is easy to see how it might confer risk for suicidality [35]. Men who are self-reliant may believe that they should be strong in the face of any adversity, consider that feeling down is a sign of weakness, and be unlikely to reach out to friends, family or professional sources for help. Indeed, the CMNI-22 assesses self-reliance in terms of behavioural and affective response to help-seeking: “I never ask for help” (Item 18) and “It bothers me when I have to ask for help” (Item 22). Help-seeking studies likewise approach self-reliance as a barrier to seeking help when experiencing mental health issues, including suicidality [36, 37], but have not explored the potential contribution of self-reliance as a masculine norm to the development of suicidal ideation.
It is possible to see how self-reliance may fit with current psychological theories of the suicidal process (i.e., how conformity to cultural or societal norms may influence cognitions and behaviours). For example, O’Connor’s Integrated Motivational-Volitional Model (IMV) suggests that the intention to engage in suicidal behaviour is underpinned by a feeling of entrapment, which in turn is triggered by feelings of defeat or humiliation [38]. It might be hypothesised that a man who is normally self-reliant might experience heightened levels of defeat or humiliation if his usual state is threatened in some way. In addition, his feelings of entrapment might be particularly severe if his usual modus operandi is to solve problems for himself, rather than to seek help from others. Similarly, Joiner’s Interpersonal Psychological Theory (IPT) suggests suicidal acts result from the confluence of a desire for death (caused by thwarted belongingness and perceived burdensomeness, and a lack of hope that these psychological states will improve) and the capability to act on this desire [39]. Self-reliance may influence either the psychological states (e.g., leading to an acute sense of burdensomeness in circumstances of perceived dependence) or the capability for suicide (being associated with a sense of invulnerability, which in turn may be related to a reduced fear of death).
Implications for suicide prevention
The identified association between self-reliance and suicidal thinking in men has implications for suicide prevention. In clinical settings, consideration might be given to ways of ensuring that services are geared towards and attractive to males who normally feel that they can do things for themselves. Interventions offered to males in these settings might include those that are accepted as standard practice in suicide prevention (e.g., psychotherapy and pharmacotherapy for depression), augmented by more tailored discussions about the impact of self-reliance on mental health and wellbeing. As others have noted, there is room for the development of male-specific therapies and services here [14].
At the other end of the suicide prevention spectrum, universal prevention activities that target males might also benefit from incorporating elements that actively address self-reliance. For example, a universal intervention like a suicide prevention media campaign that targeted males might be optimally effective if it explicitly addressed self-reliance, noting that although this can be adaptive it can act as a barrier to talking through problems and seeking help from informal and formal sources. Alternatively, a universal intervention like restricting access to means might want to focus on particular suicide methods that might symbolise masculine ways of “taking matters in hand”, like firearms or jumping from prominent heights.
More generally, as with other areas of suicide prevention, a societal approach is needed. If adherence to an element of dominant masculinity has negative consequences for men, then, as a society, we need to consider ways of ensuring that masculinity is more broadly defined and that men’s roles, relationships and possible identities are expanded.
Other factors associated with masculinity
It is worth commenting here about the other 10 factors measured by the CMNI which, in the multivariate analysis, did not appear to be associated with suicidal thinking. Lack of statistical support for the hypothesis that these other factors might be related to suicidal thinking should not be interpreted as refutation of that hypothesis. Suicidal thoughts and behaviours are underpinned by a complex array of factors, and it may be that other aspects of masculinity have an impact on suicidal thoughts via more mediated pathways. For example, high levels of emotional control may lead to fewer close relationships and social isolation, both of which may confer risk for suicidal thinking. Similarly, importance of work may lead to suicidal thinking in the context of job stressors or unemployment. More research in these areas—both quantitative and qualitative—is clearly warranted.
Study limitations
Our study relied on cross-sectional data so we cannot ascribe causality to the observed association between self-reliance and suicidality with any certainty. Having said this, we did use a proximal measure of suicidal thinking as our outcome measure (the PHQ-9 provides an indication of suicidal thinking over the past two weeks), whereas our primary predictor variable was more related to a more ingrained characteristic (the CMIN-22 asks about levels of agreement with particular statements without specifying a timeframe). We will be able to draw firmer conclusions when data are available from Wave 2 of Ten to Men (in early 2017) and we can conduct longitudinal analyses.
Other limitations include our reliance on self-report, and the fact that our sampling strategy meant that males in remote areas and/or who were not proficient in English were under-represented.
In addition, we used a single item from the PHQ9 depression screen to capture current suicidal ideation rather than a suicide specific assessment instrument, and the item combines “passive” suicidal ideation (thoughts of being better off dead) with “active” suicidal ideation (thoughts of hurting oneself). We believe this was defensible, however, because when this item has been used to screen for suicidal ideation it has shown good specificity and reasonable sensitivity when compared to a structured clinical interview [40].
Finally, we acknowledge that our outcome was suicidal thinking, whereas the excess male rate occurs for suicide. In the suicide prevention literature, suicidality is often thought of as developing along a continuum that begins with suicidal thoughts, continues through suicidal plans and suicide attempts that may increase in severity, and ends with suicide [41]. Of course, not all suicidal individuals travel in a linear fashion along this continuum, and it is overlaid with other constructs, such as degree of intent. There is a need for additional research to explore the relationship between masculinity and other points on the continuum, particularly suicide. Psychological autopsy studies could provide a vehicle for doing this.
Conclusions
These limitations aside, the study provides new insights that may assist in unravelling the vexing question of why males are more prone to suicide than females. It suggests that one particular element of dominant masculinity—being self-reliant—may place men at increased risk of suicidal thinking. This finding resonates with current theories of how suicidal thinking develops and leads to action. It also has implications for the full gamut of suicide prevention approaches that target males in clinical settings and in the general population, and for our broader society. Further work is needed, however, to confirm the direction of the relationship between self-reliance and suicidality, and to unpack the means through which self-reliance may exert an influence.
Change history
15 September 2017
In the original publication there was an error in the calculation of scores for a number of the CMNI subscales and consequently the overall scale score. Recalculating the scores did not alter the substantive finding, and largely resulted in only small adjustments to estimates. Tables 1 and 2 are revised to show the corrected values, and revisions to the text reflecting these changes are noted.
Notes
This breakdown reflects a deliberate oversampling of males in regional areas in Ten to Men.
References
World Health Organization (2014) preventing suicide: a global imperative. World Health Organization, Geneva
Houle J, Mishara B, Chagnon F (2008) An empirical test of a mediation model of the impact of the traditional male gender role on suicidal behavior in men. J Affect Disord 107:37–43
Moller-Leimkuehler A (2002) Barriers to help-seeking by men: a review of sociocultural and clinical literature with particular reference to depression. J Affect Disord 71:1–9
Hawton K (1998) Why has suicide increased in young males? Crisis 19:119–124
Kendler K, Thornton L, Prescott C (2001) Gender differences in the rates of exposure to stressful life events and sensitivity to their depressogenic effects. Am J Psychiatry 158(4):587–593
Tomova L, von Dawans B, Heinrichs M, Silani G, Lamm C (2014) Is stress affecting our ability to tune into others? Evidence for gender differences in the effects of stress on self-other distinction. Psychoneuroendocrinology 43:95–104
Cleary A (2012) Suicidal action, emotional expression, and the performance of masculinities. Soc Sci Med 74:498–505
Griffith D (2015) “I am a man”: manhood, minority men’s health and health equity. Ethn Dis 25(3):287–293
Mahalik J, Walker G, Levi-Minzi M (2007) Masculinity and health behaviors in Australian men. Psychol Men Masculin 8(4):240–249
Niehaus I (2012) Gendered endings: narratives of male and female suicides in the South African Lowveld. Cult Med Psychiatry 36:327–347
Oliffe J, Ogrodniczuk J, Bottorff J, Johnson J, Hoyak K (2012) “You feel like you can’t live anymore”: suicide from the perspectives of Canadian men who experience depression. Soc Sci Med 74:506–514
Alston M (2012) Rural male suicide in Australia. Soc Sci Med 74:515–522
Fogarty A, Proudfoot J, Whittle E, Player M, Christensen H, Hadzi-Pavlovic D, Wilhelm K (2015) Men’s use of positive strategies for preventing and managing depression: a qualitative investigation. J Affect Disord 188:179–187
Coleman D (2015) Traditional masculinity as a risk factor for suicidal ideation: cross-sectional and prospective evidence from a study of young adults. Arch Suicide Res 19(3):366–384
Granato S, Smith P, Selwyn C (2015) Acquired capability and masculine gender norm adherence: potential pathways to higher rates of male suicide. Psychol Men Masculin 16(3):246–253
Easton S, Renner L, O’Leary P (2013) Suicide attempts among men with histories of child sexual abuse: examining abuse severity, mental health, and masculine norms. Child Abuse Negl 37:380–387
Mansdotter A, Lundin A, Falkstedt D, Hemmingsson T (2009) The association between masculinity rank and mortality patterns: a prospective study based on the Swedish 1969 conscript cohort. J Epidemiol Community Health 63:408–413
Pirkis J, Currier D, Carlin J, Degenhardt L, Dharmage S, Giles-Corti B, Gordon I, Gurrin L, Hocking J, Kavanagh A, Keogh L, Koelmeyer R, LaMontagne A, Patton G, Sanci L, Spittal M, Schlichthorst M, Studdert D, Williams J, English D (2016) Cohort profile: Ten to Men (The Australian Longitudinal Study on Male Health). Int J Epidemiol. doi:10.1093/ije/dyw055
Kroenke K, Spitzer RL, Williams JBW (2001) The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 16:606–613
Mahalik J, Locke B, Ludlow L, Diemer M, Scott R, Gottfried M, Freitas G (2003) Development of the conformity to masculine norms inventory. Psychol Men Masculin 4(1):3–25
Thompson E, Bennett K (2015) Measurement of masculinity ideologies: a (critical) review. Psychol Men Masculin 16(2):115–133
Iwamoto D, Gordon D, Oliveros A, Perez-Cabello A, Brabham T, Lanza S, Dyson W (2012) The role of masculine norms and informal support on mental health in incarcerated men. Psychol Men Masculin 13(3):283–293
Owen J (2010) Assessing the factor structures of the 55- and 22-item versions of the Conformity to Masculine Norms Inventory. Am J Men’s Health 5:118–128
Australian Bureau of Statistics (2013) Census of population and housing: socio-economic indexes for areas (SEIFA), Australia, 2011 (Cat. No. 2033.0.55.001). Australian Bureau of Statistics, Canberra
Australian Bureau of Statistics (2011) Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure. Australian Bureau of Statistics, Canberra
Tarlov A, Ware J, Greenfield S, Nelson E, Perrin E, Zubkoff M (1989) The medical outcomes study: an application of methods for monitoring the results of Medical Care. J Am Med Assoc 262:925–930
Holmes T, Rahe R (1967) The social readjustment rating scale. J Psychosom Res 11(2):213–218
Pachana N, Brilleman S, Dobson A (2011) Reporting of life events over time: methodological issues in a longitudinal sample of women. Psychol Assess 23(1):277–281
Currier D, Spittal MJ, Patton G, Pirkis J (2016) Life stress and thoughts of death: the relationship between life events and suicidal ideation in Australian men—cross-sectional analysis of Ten to Men baseline data. BMC Public Health 16(Suppl 3):1031. doi:10.1186/s12889-016-3702-9
Babor T, Higgins-Biddle J, Saunders J, Monteiro M (2001) The alcohol use disorders identification test: guidelines for use in primary care, 2nd edn. World Health Organization, Geneva
Australian Bureau of Statistics (2015) The Australian Health Survey. Australian Bureau of Statistics. http://www.abs.gov.au/australianhealthsurvey. Accessed 18 Aug 2015
StataCorp (2013) Stata: Release 13.1. StataCorp LP, College Station TX
Last J (2001) A dictionary of epidemiology. Oxford University Press, Oxford
Mahalik J, Talmadge W, Locke B, Scott R (2005) Using the conformity to masculine norms inventory to work with men in a clinical setting. J Clin Psychol 61(6):661–674
Labouliere C, Kleinman M, Gould M (2015) When self-reliance is not safe: associations between reduced help-seeking and subsequent mental health symptoms in suicidal adolescents. Int J Environ Res Public Health 12:3741–3755
Hom MA, Stanley IH, Joiner TE Jr (2015) Evaluating factors and interventions that influence help-seeking and mental health service utilization among suicidal individuals: a review of the literature. Clin Psychol Rev 40:28–39. doi:10.1016/j.cpr.2015.05.006
Gulliver A, Griffiths KM, Christensen H (2010) Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry 10:113. doi:10.1186/1471-244X-10-113
O’Connor R (2011) The integrated motivational-volitional model of suicidal behaviour. Crisis 32:295–298
Van Orden K, Witte T, Curkrowicz K, Braithwaite S, Selby E, Joiner T (2010) The interpersonal theory of suicide. Psychol Rev 117:575–600
Uebelacker LA, German NM, Gaudiano BA, Miller IW (2011) Patient health questionnaire depression scale as a suicide screening instrument in depressed primary care patients: a cross-sectional study Prim Care Companion CNS Disord. 13(1). doi:10.4088/PCC.10m01027
Sveticic J, De Leo D (2012) The hypothesis of a continuum in suicidality: a discussion on its validity and practical implications. Mental Illness 4(2):e15
Acknowledgements
The research on which this paper is based was conducted as part of the Australian Longitudinal Study on Male Health (Ten to Men). We are grateful to the Australian Government Department of Health for funding and to the boys and men who provided the survey data. Ten to Men is managed by the University of Melbourne. Ten to Men data are the intellectual property of the Commonwealth.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical standards
Ten to Men was approved by the University of Melbourne Human Research Ethics Committee and, therefore, been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants gave written informed consent.
Conflict of interest
All authors report no conflict of interest.
Additional information
An erratum to this article is available at https://doi.org/10.1007/s00127-017-1443-4.
Rights and permissions
About this article

Cite this article
Pirkis, J., Spittal, M.J., Keogh, L. et al. Masculinity and suicidal thinking. Soc Psychiatry Psychiatr Epidemiol 52, 319–327 (2017). https://doi.org/10.1007/s00127-016-1324-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-016-1324-2