
Abstract
Purpose
The aim of this study was to investigate whether socio-demographic variables and physical disability (e.g. sensory impairment and mobility problems) were associated with self-reported stigma in people with intellectual disabilities (ID), and to examine whether age, sex and ethnicity modified the relationship between severity of intellectual disability and self-reported stigma.
Methods
229 participants with mild or moderate intellectual disabilities were recruited from 12 centres/sites in England from community intellectual disability services, day centres, supported housing schemes, voluntary organisations and invitation letters. Information on physical disability and socio-demographic variables were obtained using a structured data collection form. Self-reported stigma was measured using a validated questionnaire.
Results
Age was associated with self-reported stigma, with older adults reporting more stigmatising experiences. Participants with moderate intellectual disabilities were more likely to report being treated differently such as being made fun of and being treated like children. Physical disability such as sensory, mobility and speech problems were not associated with self-reported stigma. Gender modified the relationship between severity of ID and self-reported stigma as participants who were male and had moderate ID were more likely to report stigma compared to females with moderate ID. Categorical age also modified the relationship between severity of ID and self-reported stigma as older participants who had moderate ID were more likely to report stigma compared to younger people with moderate ID.
Conclusions
Older adults and those with moderate ID are potentially at higher risk of being targets of public stigma or are more likely to report stigma. Interventions to help individuals cope with stigma could be targeted to this group.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Intellectual disabilities (ID) is defined by the World Health Organisation [1] as “a condition of arrested or incomplete development of the mind, characterised by impairment of skills and overall intelligence in areas such as cognition, language, motor and social abilities, arising in the developmental period”. People with ID are consistently identified as one of the least acceptable groups in society [2, 3] and are often the target of disability related hate crime [4]. People with ID frequently report experiences of bullying [5] and of being rejected and treated negatively [6].
Public stigma can be conceptualised as a process by which certain groups, such as those with mental illness or ID, are marginalised and devalued by society because their values, characteristics or practices differ from the dominant cultural group. The social cognitive model of stigma involves cognitive, behavioural and emotional aspects presenting as stereotypes, prejudice and discrimination towards the marginalised group [7, 8]. Discrimination may take several forms. It may lead to withholding of help, avoidance, coercive treatment, and segregation. People from stigmatised groups, such as those with mental illness, frequently encounter discrimination that restricts opportunities in a number of domains including housing, education, employment, benefits, relationships with family and friends, and dating and marriage prospects [9–11]. Employment rates are low amongst people with ID and when paid work is available, it is usually in the form of sheltered workshops [12]. A key barrier to community-based employment is the belief that people with intellectual disabilities are “unemployable” [13].
Self-stigma, also known as internalised stigma occurs when individuals direct the stigmatised attitudes towards themselves [8, 14–16]. Self-stigma, like public stigma, comprises of stereotypes, prejudice and discrimination. Stereotypes such as “I am a weak person” are endorsed by the individual and lead to self-prejudice in the form of negative emotional responses, such as low self-esteem or self-worth. Self-prejudice can then lead to self-discrimination through behavioural responses such as not seeking employment opportunities or avoiding social relationships. The concept of self-stigma is poorly described amongst people with ID. In this paper we use the term self-reported stigma to describe experiences of being treated negatively and emotional reactions to discrimination as reported by people with ID. There are currently no instruments available that measure self or internalised stigma in people with ID.
Awareness of the stigma associated with ID
A number of studies have demonstrated that people with ID have varying awareness of the stigma attached to ID, which may be linked to factors such as limited cognitive development, over-protection from significant others and denial [17]. There is some evidence that people with ID are aware of their stigmatised status and endorse negative stereotypes such as believing that they cannot not engage in certain activities or have the same opportunities as those who did not have ID [18, 19], and awareness of the stigma attached to day services or long stay hospitals [19, 20].
Awareness of stigma is influenced by whether individuals with ID acknowledge and accept their ID. Cunningham and Glenn interviewed people with Down Syndrome and found that only half of the participants were aware that they had Down Syndrome and only a quarter were aware of the stigma associated with the condition [21]. Some individuals with ID may reject the label of ID entirely or may accept the label but may not be aware of the negative stereotypes that are attached to it or endorse these stereotypes [20]. These individuals may compare themselves favourably [22] with people who do not have ID and may have similar aspirations in life [23]. However, despite the low awareness of the stigma, studies have shown that people with ID are able to describe experiences of being treated differently and negatively [20, 23]. Therefore, individuals may experience stigma at an emotional level through their social interactions with others.
Socio-demographic factors associated with self-stigma
In people with mental illness (without ID), self-stigma has not been found to be consistently associated with demographic factors such as age, sex, ethnicity, marital status, employment and income [24]. However, in one meta-analysis, two thirds of the studies found that higher levels of self-stigma were associated with younger age and a third found that it was associated with older age [24]. In people living with HIV, lower income and lower age are associated with self-stigma [25].
Few studies have found an association between reports of stigma and socio-demographic variables in people with ID, most likely because of the small sample sizes of previous studies, which often included 50 participants or less [6]. However, in one study of 191 participants with mild and moderate ID in Cape Town, South Africa, self-reported stigma was associated with age [26]. Younger participants were more likely to describe stigmatising treatment than older individuals with ID. Other studies of people with ID found no relationship between stigma and age [23, 27, 28]. Previous studies of people with ID have not found a relationship between sex and self-reported stigma [23, 26–30] or between IQ or severity of ID and self-reported stigma [23, 26–28].
Only one study has explored the relationship between ethnicity and self-reported stigma in people with ID. In the South African study [26] there was a trend between ethnicity (Caucasian, Black African and Mixed ethnicity) and self-reported stigma, with the Black African group reporting more stigmatising experiences, but this difference was not statistically significant. However, severity of ID modified the relationship between ethnicity and self-reported stigma, with Black African participants with mild ID reporting higher levels of self-reported stigma compared to Black African participants with moderate ID. This study also found a trend towards participants with lower socio-economic status reporting higher levels of stigma. The study also found that there was a trend towards self-reported stigma being associated with “additional disability” (sensory, speech or mobility problems, unusual appearance or physical illness, e.g. epilepsy).
Psycho-social factors associated with self-stigma
In people with mental illness, higher levels of self-stigma is consistently associated with hopelessness, poorer self-esteem, reduced quality of life, lower empowerment and mastery, lower self-efficacy and lower social support [24]. In people living with HIV, self-stigma has been found to be associated with lower social support [25].
In people with ID, studies have demonstrated a consistent association between higher levels of reported stigma and lower self-esteem and more negative social comparisons with others [27, 28]. Higher levels of stigma have also been found to be associated with lower aspirations about the future [28, 30] and lower job satisfaction [30].
We have recently published a study investigating the relationship between self-reported stigma and a number of health outcomes in people 229 participants with mild and moderate ID from 12 sites/centres in England [31]. In this paper, we use the data obtained in the above study [31] to examine the association between self-reported stigma and socio-demographic variables and physical disability in people with ID. We define physical disability broadly to include any characteristics that are potentially stigmatising. This includes characteristics that are apparent to others such as the presence of genetic disorders speech, sensory and mobility problems, and characteristics that are less apparent to others such as the presence of epilepsy or general health problems.
Previous studies examining the relationship between stigma and socio-demographic variables have had methodological limitations such as small sample sizes [23, 27–30], lack of generalisability of findings due to unrepresentative samples and the use of a measure of stigma with poor reliability [6].
Aims and objectives of the study
-
1.
To examine the association between self-reported stigma and the following variables: severity of ID (mild or moderate ID), age, sex, ethnicity, degree of urban development, type of accommodation, employment status, social network, presence of mobility problems, sensory problems, speech abnormalities, genetic disorders, epilepsy, any physical health problem and any regular medication.
-
2.
To investigate whether age, sex and ethnicity modified the relationship between severity of ID (mild or moderate ID) and self-reported stigma.
Method
Ethical approval
Ethical approval was obtained from the West London Research Ethics committee (3) in November 2011 and Research and Development approval was obtained at all the participating sites. The study was conducted between February 2011 and February 2013.
Recruitment
The study was conducted at 12 centres/sites in England, including six boroughs/sites in London (Camden, Islington, Newham, Tower Hamlets, Bromley/Greenwich and Waltham Forest), and the sites outside of London were Kent, Surrey, Sussex, Somerset, Nottinghamshire and Lincolnshire. These sites represented diverse areas in terms of ethnicity, and also included rural, semi-rural and urban areas.
Participants were recruited from community intellectual disability services, day centres, social clubs, supported accommodation and voluntary organisations that work with people with ID through invitation letters and via health and social care professionals who knew the individual well.
Inclusion and exclusion criteria
Participants were aged 18 or over and had ID based on administrative classification, (e.g., were eligible to receive specialist intellectual disability services). Further information about the criteria that was used to determine the presence and degree of intellectual disability (mild and moderate) is described in Ali et al. [31].
Participants with a current diagnosis of mental illness were excluded because of the potential difficulty that participants could have in differentiating whether experiences of discrimination were due to intellectual disabilities or mental illness. We included participants who were able to provide consent to take part in the study. In order to facilitate this process, information was provided in an easy read (accessible) format that included text in simplified language and large font, accompanied by pictures and symbols. Individuals with poor verbal or comprehension skills, and individuals unable to speak English, were excluded from the study.
Measures
Self-reported stigma
Self-reported stigma was measured using a questionnaire that was previously developed by the researchers [32]. This self report instrument contains ten items with two subscales. The “perceived discrimination” subscale contains items that describe discrimination and negative treatment by others such as “people talk down to me”, “people on the street make fun of me” and “people treat me like a child”. The “reaction to discrimination” subscale describes emotional reactions to discrimination such as “the way people talk to me makes me angry” and “I worry about the way people act towards me”. The questionnaire does not require participants to report experiences over a particular time scale. Instead, participants are asked to report how they feel they are generally treated by others. The Items are rated “yes” (scored 1) and “no” (scored 0) and each item is accompanied by a photograph as a visual aid to help the individual understand the items. The total score ranges from 0 to 10, with higher scores indicating higher levels of self reported stigma. In this study, the internal consistency of the scale was alpha 0.87 for the full scale (perceived discrimination subscale: alpha 0.82; reaction to discrimination: alpha 0.74).
A structured data collection form was used to collect demographic information and information on physical disability. This was interviewer administered and included information on age, sex, ethnicity, marital status, attendance at a mainstream school or special school), accommodation status, employment status, number of friends, and degree of urban development. Information on physical disability included genetic disorders, sensory problems, mobility problems, presence of speech difficulties, epilepsy, general health problems and whether the participants were taking any regular medication. Data on level of ID were based on information obtained from referrers and clinical records and not on formal IQ testing.
Administration of questionnaires
The questionnaires were administered face to face, either at the participant’s home or another suitable setting (e.g., day centre). Participants were supported to complete the questionnaires, such as reading the question out aloud, paraphrasing questions to improve understanding and explaining the response format. Participants received a £20 gift voucher as an acknowledgement for their time and effort.
Sample size calculation
A minimum sample size of 171 was calculated, based on a regression analysis with a moderate effect size (f 2 0.15) and 15 predictors at 90 % power and 5 % significance level.
Analysis of data
Descriptive analysis
The data were analysed using SPSS (version 17). Some of the variables were reduced to smaller categories or dichotomised to aid analysis and interpretation of the data. Data for the whole sample were analysed descriptively. The mean, standard deviation and range of scores on the stigma questionnaire were obtained. The proportion of people responding to each item on the stigma questionnaire was analysed using Chi Square tests to identify whether the responses differed according to gender, age group, level of ID and ethnicity.
Regression analysis
Linear regression was used initially to examine whether any of the socio-demographic or clinical variables were associated with self-reported stigma. Following this, multivariate regression analysis was carried out using a random effects model to adjust for clustering by centre. There was no evidence of clustering by centre, and therefore normal regression analysis was performed. The total score on the stigma questionnaire was entered as the dependent variable in the random effects regression model. Potential confounders (age, gender, level of ID and ethnicity), and all the variables that were related to self-reported stigma in the linear regression analysis with p values of 0.2 or below, were then simultaneously added to the model. The variables that had p values equal to or less than 0.05 were identified as being independently associated with self-reported stigma.
Investigating effect modification
Interaction effects were investigated to identify whether age, sex and ethnicity modified the relationship between severity of ID and self-reported stigma. Interaction effects were analysed using the unadjusted model (stigma, severity of ID and interaction variable) and adjusted regression model (stigma, interaction variables and potential confounders).
Results
Recruitment
A total of 234 participants consented to take part in the study. Three participants were later withdrawn as they did not strictly meet the eligibility criteria (had a current diagnosis of mental illness for which they were receiving treatment), and two were excluded from the analysis as they did not complete the stigma questionnaire, leaving a total of 229 participants.
Characteristics of the participants
-
1.
Socio-demographic characteristics
Almost three quarters of the sample had a mild ID (72.7 %), 52.4 % were males, 82 % were from White ethnic backgrounds, and the mean age of the sample was 40.9 years (SD 11.4; range 19–73). The majority of the participants were single (62.9 %), only 2.2 % were in full time employment but 31.9 % were in part time paid employment (either in competitive or sheltered employment). The majority of the participants were living with their family or in supported accommodation (82 %).
-
2.
Physical disability
Thirty two percent pf the sample had a sensory problem; 32.8 % had speech abnormalities, 10.5 % had mobility problems, 64.6 % had at least one health problem, which included 17.0 % with epilepsy and 8.7 % had a genetic disorder or a syndrome, including Down Syndrome (5.2 %).
Exploring the socio-demographic variables associated with stigma
-
1.
Distribution of self reported stigma scores
The median score was 4.0 and the mean score was 4.2 (SD 3.3) in the whole sample.
-
2.
Responses to individual items on the stigma questionnaire according to socio-demographic factors
Item 9 (I keep away from other people because they are not nice to me) and item 1 (people talk down to me) received the most “yes” responses (58.5 and 48.5 % of the sample). Item 6 (people laugh at me because of the way I talk) and item 5 (People treat me like a child) received the fewest “yes” responses (31.9 and 32.3 %, respectively).
When the responses from participants with mild ID were compared to those with moderate ID (Table 1), a significantly higher proportion of people with moderate ID rated “yes” to four items compared to those with mild ID (item 2: people on the street make fun of me, p = 0.02; item 4: people laugh at me because of the way I look, p = 0.001; item 5: people treat me like a child, p = 0.05 and item 6: people laugh at me because of the way I talk, p = 0.02).
Table 1 Comparison of responses to individual items on the stigma questionnaire given by people with mild and moderate intellectual disability When the responses from males and females were examined, a significantly higher proportion of females rated “yes” to item 10. When the responses were compared across different age groups (Table 2), increasing age group was associated with a higher proportion of “yes” responses to all the items (p < 0.01 for almost all of these items) except for item 5 (people treat me like a child). Participants from White and non white backgrounds gave similar responses, apart from item 8 (people make me feel embarrassed) where a higher proportion of “yes” responses was given by those from a White background (Chi Square 4.21; p = 0.04).
Table 2 Responses given by different age groups to individual items on the stigma questionnaire -
3.
Regression analysis
The variables that had a strong association with self-reported stigma were older age (regression coefficient 0.06; p = 0.001); having a health problem (regression coefficient 1.38; p = 0.001) and sensory problems (regression coefficient 1.25; p = 0.01). There was a moderate association between self-reported stigma and not being in paid employment (regression coefficient −1.02; p = 0.02) and taking medication (regression coefficient 0.81; p = 0.05). There was a borderline association between self-reported stigma living in an urban area (regression coefficient 1.91; p = 0.08). Table 3 shows the results of the multivariate analysis of the variables that are independently associated with self reported stigma in the regression analysis. The only variable that was found to be strongly associated with self reported stigma, after adjustment of other variables, was age (older age associated with higher levels of stigma; p = 0.01). There was a weak association with having a physical health problem (p = 0.07) and being married or in a relationship (p = 0.08).
Table 3 The variables that are independently associated with self-reported stigma in the regression analysis The independent predictors of the two stigma subscales were analysed. Having a moderate ID (regression coefficient 0.60, p = 0.05) and older age (regression coefficient 0.02, p = 0.01) were associated with higher scores on the perceived discrimination subscale. Older age was the only variable associated with the reaction to discrimination subscale (p = 0.05).
-
4.
Self-reported stigma and moderating factors
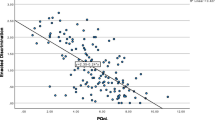
Ethnicity did not modify the relationship between self-reported stigma and severity of intellectual disabilities. However, gender and age were both effect modifiers (regression coefficient −1.83; p = 0.05 and regression coefficient 0.09; p = 0.04, respectively). Males with moderate ID reported higher levels of stigma compared to males with mild ID, and females with mild ID reported higher levels of stigma compared to females with moderate ID. This relationship is shown graphically in Fig. 1. Older people with moderate ID reported higher levels of stigma than younger people with moderate ID. This can be visualised graphically using categorical age (Fig. 2).
Fig. 1 
Interaction effects between gender and intellectual disability on self reported stigma. Males with moderate ID reported higher levels of stigma compared with males with mild ID; the reverse was seen in females
Fig. 2 
Interaction effects between categorical age and intellectual disability on self reported stigma. Older participants with moderate ID reported more stigma compared to younger males with moderate ID. The effect of age in those with mild ID was similar for all age categories


Discussion
Summary of the results
In this cross-sectional study of 229 participants with mild and moderate ID from 12 centres in England, we found that self-reported stigma was associated with older age. Participants with moderate ID were more likely to report experiences of being mocked or treated differently (e.g. being laughed at and made fun of, or being treated like children). In addition, there was a trend towards higher levels of self-reported stigma in participants who were married or in a relationship, and those who had health problems.
Results in the context of other studies
The association between self-reported stigma with age could be explained by cumulative adverse life events, including greater exposure to potentially stigmatising treatment increasing with age. This is reflected in the data, where older people (particularly the 60–80 age group) reported more stigmatising treatment. There may also be a period effect resulting from older participants having lived through a more stigmatising era. Deinstitutionalisation and government policies promoting the integration of people with intellectual disabilities in the community, and the promotion of equality and independence, are relatively recent changes. Participants from the older age group are more likely to have lived in institutionalised settings in the past, or may be currently living in residential settings, where certain types of stigmatising treatment are more common. In addition, they may be subject to additional age related discrimination.
Previous published studies of people with ID have not found a relationship between stigma and age [23, 27, 28]. However, Ali et al. [26] found that self-reported stigma was associated with age in participants from South Africa. However, in this study, stigma was associated with younger age. One meta-analysis of studies of people with mental illness (without ID) also found that both older and younger age was associated with self-stigma [24].
There was a trend towards physical health problems being related to self-reported stigma. This may be because some types of physical health problems are also stigmatising. In the South African study mentioned above [26], there was a trend towards stigma being associated with “obvious additional disability”, which included physical illness as well as other potentially stigmatising features such as sensory problems, mobility problems and where the individual looked “noticeably different to other people”. The combination of stigma due to ID and stigma due to physical health problems may result in “double stigma”. Individuals with both mental illness and physical illness report higher levels of stigma compared to individuals with only mental illness [33]. Double discrimination has been described in other groups with two or more stigmatising attributes such as those from ethnic minority groups who also have ID, or mental illness [34] or who are gay [35]; or individuals suffering from a serious mental illness and obesity [36] or substance abusers who also have HIV [37].
It is not clear why there was a trend towards an association of self-reported stigma with marital status. This appears counter-intuitive as one would expect that being married or in a relationship would be a “normalising” experience that would reduce the experience of self reported stigma. One possible explanation is that being married increases awareness of social limitations due to the pressure of having to fulfil certain roles and expectations, such as looking after children or working, and individuals may receive more critical comments from their partners. In many cultures around the world, disabled men and women are expected to marry and have children. The findings in relation to stigma and marital status may partly explain the results of a large cross sectional study, which found that wellbeing in women with intellectual disabilities was associated with being single [38]. In addition, studies of people with mental illness have found that one of the most common sources of discrimination is from family and close friends [39]. Alternatively, the relationship between self-reported stigma and marital status may be a spurious finding.
Although level of ID was not an independent predictor of self-reported stigma, those with moderate ID were more likely to report certain types of stigmatising treatment, particularly those involving discriminatory treatment by the public. People with moderate ID often have more noticeable or visible distinguishing features that may alert members of the community or neighbourhood that they are “different”, making them the target of abuse or harassment. Participants with intellectual disabilities are often treated unfairly when accessing the community and using public transport [40].
Participants with moderate ID did not report more negative reactions to discrimination such as getting angry or avoiding others. One explanation for this is that people with intellectual disabilities may not internalise their intellectual disability [20, 21, 41], thus, although they may be able to describe experiences of negative treatment, they may not relate these experiences to having the label of intellectual disabilities. This may occur because of insufficient cognitive development [21], which is required to enable individuals to compare themselves to others, and to understand the actions of others. Previous studies did not find a relationship between severity of ID, as measured by IQ, and stigma [23, 26–28], possibly because these studies had a small sample size, and they did not distinguish between different dimensions of stigma (e.g., discrimination or emotional reactions).
Our study found no differences between males and females in the levels of self-reported stigma, which is consistent with previous studies [23, 26–30]. However, males with moderate ID and females with mild ID were more likely to report stigma, which suggests that these individuals may be more susceptible to self reported stigma due to gender expectations. McDonald et al. [42] found that having an ID had differential effects in males and females. In males, it diminished the positive effects of their masculinity (e.g. males regarded as less competitive), and in females it accentuated the negative effects of their femininity (e.g. females regarded as being more dependent, less competent).
The finding that older individuals with moderate ID reported more stigma compared to younger individuals with moderate ID is perhaps understandable given that age is an independent predictor of stigma, and having moderate ID is associated with being treated differently.
Strengths and limitations
The sample size was relatively large compared to previous studies on self-reported stigma. Participants were also recruited from different settings and geographical sites (including rural and urban areas), using different methods and are therefore more representative of people with ID living in the community, compared to previous studies.
One of the main limitations of the study is the use of a ten-item instrument to measure self-reported stigma. The instrument does not capture all the different types of discriminatory and stigmatising treatment that individuals with ID may experience, which may vary between different age groups, gender and ethnicity.
Participants with mental illness were excluded from the sample. The point prevalence of mental health problems in people with ID varies between 16 and 41 % depending on the diagnostic criteria that is used [43]. Therefore a relatively large proportion of people were excluded from the study, which could potentially affect the generalisability of the results as experiences of stigmatising treatment may differ in those with mental health problems.
Another limitation was that IQ was not formally measured and information about the degree of ID was obtained from referrers and clinic notes. Most of the data obtained about socio-demographic variables were based on self-report, but where possible, information was corroborated with carers. However, this was not always possible, and may have affected the accuracy of the data.
Implications
Older adults and those with moderate ID may be at higher risk of being targets of discrimination and stigma directed by members of the public or those close to them. Services that support people with ID, such as community intellectual disability teams, could provide targeted support to older adults with ID and those with moderate ID, such as counselling to help individuals develop effective coping strategies and resilience, and practical support to report abuse and crimes to the police. It is also essential that the police, who have been criticised for not regarding people with ID as credible witnesses [44], deal with reported crimes in a serious and sensitive manner.
It is important to tackle negative stereotypes such as people with ID being regarded as incapable of working or living independently. Interventions that tackle public stigma (e.g. targeting specific groups such as school children or police officers and that involve direct or indirect contact with people with ID (particularly older individuals with moderate ID) could help to improve awareness and attitudes towards people with ID. For example, Film clips of people with ID, based on “protest” that highlights the immoral justice of stigma, have been found to be effective in changing attitudes [45].
References
World Health Organisation (1992) The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. World Health Organization, Geneva
Gordon PA, Feldman D, Tantillo JC, Perrone K (2004) Attitudes regarding interpersonal relationships with persons with mental illness and mental retardation. J Rehabil 70:50–56
Nagata KK (2007) The measurement of the Hong Kong-based ‘baseline survey of students’ attitudes toward people with disability’: cross cultural validation in Lebonon. Int J Rehabil Res 30:239–241
Sheik S, Pralat R, Reed C, Sin CH (2010) Don’t stand by. Hate Crime Research Report, Mencap. http://www.mencap.org.uk
Emerson E (2010) Self reported exposure to disablism is associated with poor self reported health and wellbeing among adults with intellectual disabilities in England: a cross sectional survey. Public Health 124:682–689
Ali A, Hassiots A, Strydom A, King M (2012) Self stigma in people with intellectual disabilities and courtesy stigma in family carers: a systematic review. Res Dev Disabil 33:2122–2140
Corrigan PW (2000) Mental health stigma as social attribution: implications for research methods and attitude change. Clinical Psychol Sci Pract 7:48–67
Corrigan P, Watson A (2002) Understanding the impact of stigma on people with mental illness. World Psychiatry 1:16–20
Time to Change (2008) Stigma shout: service user and carer experiences of stigma and discrimination. Time to Change, London
Social Exclusion Unit (2004) Mental health and social exclusion. ODPM, London
Time to Change (2009) Stigma of mental health makes finding work in recession more difficult. YouGov poll. London: Time to Change. http://www.time-to-change.org.uk/news/stigma-mental-health-makes-findingwork-recession-more-difficult-research-finds
Braddock D, Hemp R, Rizzolo M C, Coulter D, Haffer L, Thompson M (2005) The state of the states in developmental disabilities: 2005. Boulder and Washington, DC: University of Colorado, Department of Psychiatry and Coleman Institute for Cognitive Disabilities and American Association on Intellectual and Developmental Disabilities
Shaw L, MacKinnon J, McWilliam C, Sumsion T (2004) Consumerparticipation in the employment rehabilitation process: contextual factors and implications for practice. Work J Prevent Assess Rehabil 23:181–192
Corrigan P, Watson A, Barr L (2006) The self stigma of mental illness. Clin Psychol Sci Pract 9(35):53
Corrigan P, Kerr A, Knudsen L (2005) The stigma of mental illness: explanatory models and methods for change. Appl Prevent Psychol 11:179–190
Ritsher JB, Phelan JC (2004) Internalized stigma predicts erosion of morale among psychiatric outpatients. Psychiatry Res 129:257–265
Beart S, Hardy G, Buchan L (2005) How people with intellectual disabilities view their social identity: a review of the literature. J Appl Res Intellect Disabil 18:47–56
Chen C-H, Shu B-C (2012) The process of perceiving stigmatisation: perspectives from Taiwanese young people with intellectual disability. J Appl Res Intellect Disabil 25:240–251
Jahoda A, Markova I, Cattermole M (1988) Stigma and the self concept of people with mild mental handicap. J Ment Defic Res 32:103–115
Jahoda A, Markova I (2004) Coping with social stigma: people with intellectual disabilities moving from institutions and family home. J Intellect Disabil Res 48:719–729
Cunningham C, Glenn S (2004) Self awareness in young adult with Down Syndrome: 1. Awareness of Down Syndrome and disability. Intl J Disabil Dev Educ 51:335–361
Finlay WM, Lyons E (2000) Social categorizations, social comparisons and stigma: presentations of self in people with learning difficulties. Br J Soc Psychol 39:129–146
Cooney G, Jahoda A, Gumley A, Knott F (2006) Young people with intellectual disabilities attending mainstream and segregated schooling: perceived stigma, social comparison and future aspirations. J Intellect Disabil Res 50:432–444
Livingston JD, Boyd JE (2010) Correlates and consequences of internalized stigma for people living with mental illness: a systematic review and meta-analysis. Soc Sci Med 71:2150–2161
Logie C, Gadalla TM (2009) Meta-analysis of health and demographic correlates of stigma towards people living with HIV. AIDS Care 21:742–753
Ali A, Kock E, Molteno C, Mfiki N, King M, Strydom A (2015) Ethnicity and self-reported experiences of stigma in adults with Intellectual Disability in Cape Town, South Africa. J Intellect Disabil Res 59:530–540
Paterson L, McKenzie K, Lindsay B (2012) Stigma, social comparisons and self esteem in adults with an intellectual disability. J Appl Res Intellect Disabil 25:166–176
Szivos-Bach SE (1993) Social comparisons, stigma and mainstreaming: the self esteem.of young adults with a mild mental handicap. Ment Handicap Res 6:217–236
Dagnan D, Waring M (2004) Linking stigma to psychological distress: testing a social-cognitive model of the experience of people with intellectual disabilities. Clin Psychol Psychother 11:247–254
Petrovski P, Gleeson G (1997) The relationship between job satisfaction and psychological health in people with an intellectual disability in competitive employment. J Intellect Dev Disabil 22:199–211
Ali A, King M, Strydom S, Hassiotis A (2015) Self-reported stigma and symptoms of anxiety and depression in people with intellectual disabilities: findings from a cross sectional study in England. J Affect Disord 187:224–231
Ali A, Strydom A, Hassiotis A, Williams R, King M (2008) A measure of perceived stigma in people with intellectual disability. B J Psychiatry 193:410–415
Bahm A, Forchuck C (2008) Interlocking oppressions: the effect of a comorbid physical disability on perceived stigma and discrimination among mental health consumers in Canada. Health Soc Care Commun 17:63–70
Gary FA (2005) Stigma: barrier to mental health care among ethnic minorities. Issues Ment Health Nurs 26:979–999
Zamboni BD, Crawford I (2007) Minority Stress and sexual problems among African–American gay and bi-sexual men. Arch Sex Behav 36:569–578
Mizcock L (2012) The double stigma of obesity and serious mental illnesses: promoting health and recovery. Psychiatr Rehabil J 35:466–469
Samilov D (2004) Double discrimination: drug users living with HIV/AIDS. HIV AIDS Policy Law Rev 9:83–85
Emerson E, Hatton C (2008) Self reported wellbeing of women and men with intellectual disabilities in England. Am J Ment Retard 113:143–155
Corker E, Hamilton S, Henderson C, Weeks C, Pinfold V, Rose D, Williams P, Flach C, Gill V, Lewis-Holmes E, Thornicroft G (2013) Experiences of discrimination among people using mental health services in England 2008–2011. Br J Psychiatry Suppl 202(S55):s58–s63
McEvoy SC, Keenan E (2014) Attitudes towards people with disabilities—what do people with intellectual disabilities have to say? Br J Learn Disabil 42:221–227
Finlay M, Lyons E (1998) Social identity and people with learning difficulties: implications for self-advocacy groups. Disabil Soc 13:37–51
McDonald KE, Keys CB, Balcazar FE (2007) Disability, race/ethnicity and gender: themes of cultural oppression, acts of individual resistance. Am J Commun Psychol 39(145–6):1
Cooper-SA Smiley E, Morrison J, Williamson A, Allan L (2007) Mental ill-health in adults with intellectual disabilities: prevalence and associated factors. Br J Psychiatry 190:27–35
Mencap (2010). Don’t stand by. Hate crime research report. www.opm.co.uk/wp-content/uploads/2014/02/Stand-by-me-research-report.pdf. Accessed Sept 2015
Walker J, Scior K (2013) Tacking stigma associated with intellectual disability among the general public: a study of two indirect contact interventions. Res Dev Disabil 34:2200–2210
Acknowledgments
This study was funded by the Medical Research Council (MRC) in the UK as part of a 3 year Clinical Training Fellowship award to Afia Ali. Award reference: G0901946 (ID no: 93676). We would like to acknowledge the support and contribution of the following people: Karen Dodd, Nikkita Osiadacz, Mark Hayward, Sally Skipper, Deborah Hussey, Claudia Watson, Mark Bradley, Hannah Kelly, Susan King, David Trevor, Rachael Mendy, Hannah Antoniades, Katie Finning, Andy Inett, Amy Hammond, Ian Hall, Emmanuel Akuffo, Deirdre O’Brady.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Rights and permissions
About this article

Cite this article
Ali, A., King, M., Strydom, A. et al. Self-reported stigma and its association with socio-demographic factors and physical disability in people with intellectual disabilities: results from a cross-sectional study in England. Soc Psychiatry Psychiatr Epidemiol 51, 465–474 (2016). https://doi.org/10.1007/s00127-015-1133-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-015-1133-z