
Abstract
Purpose
Network medicine considers networks among genes, diseases, and individuals. Networks of mental disorders remain poorly understood, despite their high comorbidity. In this study, a network of mental disorders in Korea was constructed to offer a complementary approach to treatment.
Methods
Data on the prevalence and morbidity of mental disorders were obtained from the 2006 and 2011 Korean Epidemiologic Catchment Area Study, including 22 psychiatric disorders. Nodes in the network were disease phenotypes identified by Diagnostic and Statistical Manual of Mental Disorders-IV, and the links connected phenotypes showing significant comorbidity. Odds ratios were used to quantify the distance between disease pairs. Network centrality was analyzed with and without weighting of the links between disorders. Degree centrality was correlated with suicidal behaviors and use of mental health services.
Results
In 2011 and 2006, degree centrality was highest for major depressive disorder, followed by nicotine dependence and generalized anxiety disorder (2011) or alcohol dependence (2006). Weighted degree centrality was highest in conversion disorder in both years.
Conclusions
Therefore, major depressive disorder and nicotine dependence are highly connected to other mental disorders in Korea, indicating their comorbidity and possibility of shared biological mechanisms. The use of networks could enhance the understanding of mental disorders to provide effective mental health services.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Various biological levels such as cells, organs, individuals, and environments are involved in the onset of disease. Since interactions occur both within and between these levels, network theory has become increasingly important to understand these complex interactions for medicine [1, 2]. In network medicine, a node, the basic unit of a network, may represent a biological factor (e.g., a gene, chromosome, metabolite, RNA, or specific disease/phenotype), and the interaction between two nodes is defined as a link [3]. Through this simplification process, networks provide new perspectives on the etiology, treatment, and classification of diseases [4].
In molecular network studies, networks are composed of a small number of highly connected nodes (hubs) and many poorly connected nodes (non-hubs). This kind of structure is observed in several types of complex networks, including World Wide Web links, biological networks, and social networks, and is referred to as a scale-free network [5–7]. Hubs play important roles in determining the network structure. For example, hub proteins are more likely to be an essential or lethal protein [8, 9]. In addition, Goh et al. [10] constructed a human disease network of Mendelian gene associations composed of disease nodes whose links represent shared genes. Their human disease network was naturally clustered according to primary disorder classes, and essential genes, that are indispensable to support cellular life, were more likely to encode hub proteins.
Hidalgo et al. [11] built a phenotypic disease network (PDN), in which diseases were linked to each other on the basis of comorbidity, using phenotypic data from clinical records. They showed that disease-related mortality is correlated with the number of connections. Phenotype mapping also may be used to predict candidate genes that play an important role in the onset of diseases. Van Driel et al. [12] showed that disease phenotypic similarity is positively correlated with biological signatures of the two linked diseases based on relatedness at the level of the protein sequence, protein motifs, and direct protein–protein interactions.
Social network analysis has also been used to understand disease spread. For example, Christakis and Fowler [13] showed that obesity has spread through social networks, in which individuals in the same social network are more likely to be obese. In addition, sexually transmitted diseases were shown to spread through a social network, where the distribution of numbers of sexual partners appeared to be a scale-free parameter [14]. This means that people who have multiple sex partners (hubs) play an important role in spreading the sexually transmitted disease; therefore, preferentially managing disease in these “hub” individuals is a more efficient means of preventing its spread.
In psychiatry, mental disorders are known to have high rates of comorbidity. Among patients who are diagnosed with a mental disorder, approximately 45 % receive another diagnosis [15]. Because of these phenotypic relationships, a network-based approach in understanding mental disorders will be helpful in several ways. First, patients with co-occurring mental disorders are in greater need of professional help and also have a poorer prognosis, result in greater psychosocial impairment, and are associated with higher suicidal rates [16–18]. In Korea, the suicide rate has increased to 31.2 per 100,000 individuals, making it one of the highest suicide levels in the world, and is one of the country’s most serious and urgent public issues [19]. However, according to the Korean Epidemiologic Catchment Area Study 2011 (KECA-2011), only 15.3 % of people with mental disorder receive treatment in Korea, which is substantially lower than rates in other countries, including 39.2 % in the USA, 34.9 % in Australia, and 38.9 % in New Zealand [20]. Hence, identifying hub disorders that should be of priority for development of a mental health policy is a potentially valuable method to increase efficient utilization of health services. Second, many disorders share common symptoms; thus, in routine clinical settings, unstructured interviews may lead to missing comorbidity [21]. Through the visualization of a network of mental disorders, such relationships can be easily recognized, which should be helpful in clinical diagnosis. Third, a better understanding of network-based knowledge may lead to the identification of pathophysiology shared by these disorders [1]. As an example of using network approach to psychopathology of comorbidity, Denny borsboom et al. showed that half of the symptoms in DSM-IV are connected, the connections of these symptoms exhibit a small world, where each symptom can be reached from almost all by a small number of steps, and distance between mental disorders are correlated with empirical comorbidity rates [22]. In addition, network model of comorbidity could be useful to understand the causal interplay between symptoms (e.g., sleep deprivation → fatigue → concentration problems) [23].
Therefore, we aimed to construct a Korean network of mental disorders, investigate the network’s characteristics, and analyze the correlation between the network’s characteristics and suicidal behaviors as well as the use of mental health services.
Methods
Source data and study population
To investigate the relationships among mental disorders, we used two large national studies of Korean adults, the KECA-R [24] and the KECA-2011 [20]. The KECA-R was conducted from July 2006 to April 2007. The KECA-2011 was conducted from July to October 2011. Both surveys were carried out with the same basic principles of survey design.
In KECA-R and KECA-2011, Subjects were selected using a multistage cluster sampling method based on data from the community registry office of the population census [25, 26]. Subjects were recruited across 12 catchment areas, which consisted of three metropolitan districts, five districts of mid-sized cities, and four rural counties. One individual per selected household was randomly chosen, and face-to-face interviews were conducted using the Korean version of the Composite International Diagnostic Interview (K-CIDI) [27] at the house of the respondent. A total of 160 interviewers who were familiar with psychiatric epidemiologic surveys, were recruited from each catchment area, including psychiatric nurses, social workers, and medical students. All of interviewers participated in a 5-day training that included didactic sessions covering general interviewing skills and the instrument content, followed by mock interviews and role-playing exercises [28, 29].
Each study protocol was approved by the institutional review board of the Seoul National University College of Medicine. Each subject was fully informed of the study objectives and methods before the interview. Informed consent was obtained prior to participation.
In the KECA-R, from the initially selected 7968 individuals aged 18–64 years, a total of 6510 participants completed the interview (response rate 81.7 %). In the KECA-2011, from the initially selected 7655 individuals aged 18–74 years, a total of 6027 participants completed the interview (response rate 78.6 %). Thus, the present study included a total of 12,532 individuals from both surveys.
Assessment of lifetime diagnostic and statistical manual of mental disorders (DSM)-IV disorders
The K-CIDI was administered to make a psychiatric diagnosis based on DSM-IV criteria [30], and has been validated by Cho et al. [27], according to the World Health Organization guidelines [28]. Weighted prevalences were calculated for the respondents and used to adjust the data to approximate the national age and sex distributions according to the 2005 census [25] and the 2010 census [26].
Assessment of lifetime suicidal behaviors and the use of mental health services
The KECA-R and KECA-2011 surveys included questions related to suicidal behaviors (suicidal ideation, plans, and attempts). However, because we were only able to access the suicidal behavior data for KECA-2011, only KECA-2011 data were used for the analysis conducted to investigate the relationship among the network model, suicidal behaviors, and the use of mental health services.
Quantifying the strength of comorbidity relationships
Comorbidity is defined as the co-occurrence of one or more disorders [31]. To quantify the strength of comorbidity in the network, we used the zero-order odds ratio (OR). The OR represents the increased chance that someone with a mental disorder will have another mental disorder. A statistically significant OR represents a risk associated with a particular factor. In the KECA-R and KECA-2011, ORs and 95 % confidence intervals were calculated from multiple logistic regression models.
Network generation
In this study, the nodes are disorder phenotypes identified based on DSM-IV, and links connect phenotypes that showed comorbidity according to statistically significant ORs. Node size is proportional to prevalence, and link thickness is proportional to the OR, reflecting the strength of the link. A connection between nodes can be either one-way (directed) or two-way (undirected). Unlike the relative risk, the OR is always the same for both disorders in a link. Thus, the direction of the connection is not reflected in this study. Based on DSM-IV, the 22 mental disorders were classified into 6 categories, which are identified by distinct colors in the network: substance-related disorders, schizophrenia and other psychotic disorders, mood disorders, anxiety disorders, eating disorders, and somatoform disorders.
We used NetMiner V.4 software [32] for exploratory analysis and visualization of the network data. We graphed the network with the use of the stress majorization method [33] to reduce the overlap between nodes and links, thus achieving more interpretable images. To identify hubs in the network, we calculated the degree centrality, which is simply defined as the number of links. In order to reflect link strength (OR), degree centrality was adjusted by the α parameter, as proposed by Opsahl et al. [34]. When α = 0, the degree centrality does not reflect the link strength. As α increases, the link strength, or weight, becomes a more significant factor for determining degree centrality than the degree itself (i.e., the number of links). When α = 0.5, link strength begins to be reflected in degree centrality. When α = 1, degree centrality is equal to the sum of the link strengths of a node. When α = 1.5, link strength is reflected more than degree in determining degree centrality. Pearson correlation coefficients were also used to evaluate the relationship among degree centrality, suicidal behaviors, and the use of mental health services.
Results
A total of 22 mental disorders were included in this study. Table 1 shows the prevalence of each disorder and the prevalence of suicidal behaviors and the use of mental health services for the included disorders. For the 12,532 subjects, the mean age was 44.4 years, and ages ranged from 18 to 79 years. 61.0 % were female, 38.6 % of the sample had been in full-time education for more than 13 years, 67.3 % were married.
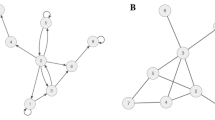
The set of all comorbidity associations between mental disorders was summarized by constructing a PDN from the KECA-R and KECA-2011 data (Figs. 1, 2). In both the KECA-R- and KECA-2011-based networks, eating disorders were isolated from the network because of their low prevalence and lack of statistically significant ORs. The other disorders were all closely connected. In the KECA-R network, bipolar disorders and somatization disorder were more isolated than in the KECA-2011 network.

Mental disorder network from the KECA-R survey data. Nodes are mental disorders. Links are correlations. The node color indicates the six main DSM-IV categories. Node size is proportional to disorder prevalence. Line thickness indicates correlation strength. This network was constructed using only links with statistically significant odds ratios

Mental disorder network from the KECA-2011 survey data. Nodes are mental disorders. Links are correlations. The node color indicates the six main DSM-IV categories. Node size is proportional to disorder prevalence. Line thickness indicates correlation strength. This network was constructed using only links with statistically significant odds ratios
Degree centrality values (α = 0, 0.5, 1, 1.5) of the 22 disorders were used to evaluate the relationship between disorders (Table 2). In the KECA-R network, the degree centrality (α = 0), reflecting only the degree and not the weight, was highest in major depressive disorder, followed by nicotine dependence, alcohol dependence, alcohol abuse, and dysthymic disorder. The weighted degree centrality at α = 0.5 was highest in posttraumatic stress disorder, followed by major depressive disorder, social phobia, obsessive–compulsive disorder, and dysthymic disorder. The weighted degree centrality at α = 1 was highest in conversion disorder, followed by social phobia, posttraumatic stress disorder, obsessive–compulsive disorder, and pain disorder. Likewise, the weighted degree centrality at α = 1.5 was highest in conversion disorder, followed by pain disorder, social phobia, obsessive–compulsive disorder, and posttraumatic stress disorder. In the KECA-2011 network, the unweighted degree centrality (α = 0) was highest in major depressive disorder, followed by nicotine dependence, generalized anxiety disorder, posttraumatic stress disorder, and obsessive–compulsive disorder. The weighted degree centrality at α = 0.5 was highest in conversion disorder, followed by social phobia, generalized anxiety disorder, posttraumatic stress disorder, and major depressive disorder. The weighted degree centrality at α = 1 was highest in conversion disorder, followed by panic disorder, social phobia, pain disorder, and posttraumatic stress disorder. The weighted degree centrality at α = 1.5 was highest in conversion disorder, followed by panic disorder, pain disorder, social phobia, and somatization. In both surveys, there was a relatively high degree of centrality in mood disorders and substance-related disorders. As the α increases, weight plays as a more significant role for degree centrality than the degree. Thus, somatoform disorders and anxiety disorders with relatively high ORs ranked higher as the α increased.
The correlations among degree centrality, suicidal behaviors (ideation, plans, attempts), and the use of mental health services were analyzed by Pearson’s correlation coefficient to investigate the clinical significance of degree centrality (Table 3). When α = 0, the degree centrality showed a significant correlation with both suicidal behaviors and the use of mental health services (p < 0.001); no significant correlation was found for weighted measures of degree centrality. Suicidal behaviors and the use of mental health services were also significantly correlated (p < 0.001).
Discussion
The aim of this study was to build a network model representing the relationships between mental disorders in Korea. Through network analysis, the KECA-R and KECA-2011 data can be illustrated in an intuitive way by allowing visualization of the relationships between mental disorders. In this study, all psychiatric disorders included, except for eating disorders, were closely connected, similar to the results of Goh et al. [10], where each disease was naturally clustered according to primary disorder class such as cardiovascular, respiratory, psychiatric, etc. Although eating disorders do show high comorbidity [35], they were likely excluded from the network because of their relatively low prevalence in the populations considered. Through the network graph, we can infer that most psychiatric disorders have high connectivity and are likely to share a common pathophysiology. Furthermore, in practice, the network map can be useful to easily recognize the possibility of comorbidities in a patient.
Determining the centrality of nodes is a basic method in network analysis, enabling identification of the most central, important, or prominent nodes (hubs) in the network. Among several possible measures of centrality, degree centrality shows good potential as an accurate indicator to predict the association between genes and diseases [36]. Thus, we used degree centrality as the main indicator to analyze the network. However, it was recently argued that calculations of degree centrality should include measurements of link strength as well as the degree, defined as the number of nodes to which a node is connected [34]. Hence, in this study, we used degree centrality reflecting link strength (OR) as well as the degree (number of links) to find the hub disorder. During this process, we adjusted degree centrality with the α parameter. In this study, when α = 0, there was a relatively high degree centrality in mood disorders and substance-related disorders. Somatoform disorders and anxiety disorders with relatively high ORs ranked highest as the α parameter increased.
Korea is well known to have a high rate of suicide [19], and, in most cases, individuals that committed suicide suffered from a mental disorder [37]. Taking these facts into account, preventative intervention is needed for individuals with a mental disorder. Nevertheless, in reality, there are limitations related to time and costs, making individual-based approaches for each mental disorder difficult. Our network model shows that mental disorders are highly connected, indicating that analysis of network characteristics would be useful to recognize the mental disorders most deserving of primary intervention in order to determine the best use of limited resources. Thus, we analyzed the correlation among degree centrality, suicidal behaviors, and the use of mental health services for establishing a cost-effective mental health policy. In this study, degree centrality, only when α = 0, showed a significant correlation with suicidal behaviors and the use of mental health services. Suicidal behaviors and the use of mental health services were more correlated to the number of comorbidities than to the sum of the strength (OR) of comorbidities. In terms of service use, these results are similar to those of a previous study indicating that the higher the comorbidity, the more likely an individual is to seek treatment [38]. This is likely due to the fact that people with comorbidities have more severe symptoms.
The relationship between suicidal behaviors and degree centrality (α = 0) indicates that there are two main ways to establish an effective health policy for suicide prevention. Focusing a policy primarily on a disorder with high degree centrality would likely lead to the decrease of suicidal behaviors and help to increase the number of patients seeking treatment. For example, when a patient with major depressive disorder (with high degree centrality) receives treatment, the many disorders connected can also benefit from the treatment. On the other hand, in the case of a disorder with low degree centrality such as somatization disorder, schizophrenia and other psychotic disorders, and pain disorder, the approach above may not be helpful due to the low connectivity. In order for patients with these less-connected disorders to participate in treatment, an individual approach is needed according to each disorder. Thus, an alternative policy focusing on clinical characteristics of disease presentation itself may be necessary. Furthermore, suicide has been used as an indicator of disorder severity [15]. Based on the correlation between suicidal behaviors and degree centrality, degree centrality shows potential as a useful indicator for predicting suicide risk and severity.
Suicidal behaviors and the use of mental health services also showed a positive correlation in Pearson’s correlation analysis. The same result was reported in a previous study, where individuals with high suicidal-risk behaviors were found to be more likely to participate in the use mental health services [39]. However, service use of considering the fact that low service use contributes to the high suicide rate in Korea, high suicide-risk groups should be identified and preferentially be provided with more treatment. In Korea, many people are reluctant to receive psychiatric treatment, because there is still a cultural stigma related to having a mental disorder, and individuals are afraid of potential disadvantages associated with a diagnosis, such as an increased likelihood of being rejected from private health insurance due to their medical record and psychiatric disorders [40].
Weighted degree centralities reflecting the strength of the links did not show a correlation with suicidal behaviors or the use of mental health services. In other words, OR is not an appropriate weight parameter to indicate suicidal behaviors or the use of mental health services. However, this does not mean that degree centrality values reflecting ORs are not clinically useful, and it is necessary to analyze the clinical relevance of other factors in this respect. In addition, relative risk or other adjustment variables can be used as an alternative to OR for a weighted analysis of degree centrality, as described by Hidalgo et al. [11].
In this study, we were not able to classify mental disorders into subgroups based on the link connectivity. This is because the mental disorders were closely linked with each other regardless of the major classes of the DSM-IV. DSM-IV is based on a categorical approach, which can be used more effectively when there is a clear and definite boundary between disorders [41]. In our study, each disorder overlapped with respect to current diagnostic classification; therefore, another diagnostic approach is needed.
The use of a network-based approach is also helpful to establish disease classification. Current disease classification has focused on a reductionist approach and has therefore neglected the interconnected nature of many diseases [1]. To overcome these limitations, the use of a systems-based network has been proposed. In psychiatry, most disorders are classified on the basis of their clinical syndromes, rather than on the knowledge of disease etiology or pathophysiology [42]. Recently, the fifth edition of the DSM [43] was published, which has been criticized for the fact that classification still focuses on clinical observations such as symptoms and signs, and does not adequately reflect advances in neurobiological, genetic, cognitive, and behavioral knowledge [44, 45]. The National Institute of Mental Health proposed the use of Research Domain Criteria (RDoC) as a new way of classifying psychopathology, which are based on dimensions of observable behaviors and neurobiological measures [46]. RDoC consist of five domains: negative valence domain, positive valence systems, cognitive systems, systems for social processes, and arousal/modulatory systems. Independent variables, including genes, molecules, cells, neural circuits, physiology, behaviors, and self-reports, are then used to analyze these five domains. This system is founded on the perspective that complex system interactions cause disease. However, RDoC do not cover clinical phenotype or define how to integrate and apply the studies in practice. One potentially helpful integration approach could be based on the method used by Goh et al. [10] to investigate the interaction between genes and diseases.
There are a few limitations of the study worth mentioning. First, it was difficult to identify comorbidity of disorders with low prevalence, because the KECA-R and KECA-2011 data are based on community surveys. For example, no significant comorbidity was found with respect to eating disorders. In addition, overall, disorders with low prevalence (e.g., conversion disorder, pain disorder) showed relatively high ORs. Conversely, disorders with high prevalence (e.g., substance-related disorders) showed relatively low ORs. For these results, degree centrality reflecting the OR is assumed not to show a correlation with suicidal behaviors and the use of mental health services. To overcome this limitation, network analysis for patients in particular will be needed, rather than for the general population. Furthermore, use of the method of Hidalgo et al. [11], in which results are weighted according to the prevalence of disorders, may be helpful in this respect. Second, in this study, no other centrality measure (e.g., closeness, betweeness, and Eigen-vector centrality) was evaluated. Hence, the clinical relevance of the network should be further explored through the calculation of other centrality measures. Third, this network study included only 22 among the many disorders in DSM-IV, indicating that further network analysis should be conducted including more disorders. Moreover, adolescents were not included in the KECA-R and KECA-2011 surveys, but are expected to be included in KECA-2015 [20]. These data may be helpful to better understand the mental disorder network by including disorders that are often diagnosed during adolescence. Fourth, because OR was used as the measure of linkage, direction could not be evaluated. Therefore, the use of a link parameter that incorporates directionality would be useful to better identify the causal relationships between disorders. Finally, the relationships among symptoms shared by multiple mental disorders were not evaluated in the present study. Because mental disorders often share a number of symptoms, Cramer et al. [47] propose an integrative method to visualize comorbidity as a symptom network, and show this approach can be helpful to evaluate causal relations between symptoms. But also, we have to consider another possibility that comorbidity is an artifact of the diagnostic system, such as DSM or ICD, because diagnostic criterion overlaps. Therefore, further studies to integrate networks between clinical phenotype and other independent variables are needed.
Our results demonstrate that degree centrality can be used as a valuable indicator to determine clinical access and for developing new mental health policies. Further network-based studies integrating the factors mentioned above can provide a new perspective for understanding the pathophysiology of mental disorders and establishing more appropriate diagnostic classification systems.
Abbreviations
- PDN:
-
Phenotypic disease network
- KECA:
-
The Korean Epidemiologic Catchment Area Study
References
Barabási AL, Gulbahce N, Loscalzo J (2011) Network medicine: a network-based approach to human disease. Nat Rev Genet 12:56–68. doi:10.1038/nrg2918
Barabási AL (2007) Network medicine–from obesity to the diseasome. N Engl J Med 357:404–407. doi:10.1056/NEJMe078114
Chan SY, Loscalzo J (2012) The emerging paradigm of network medicine in the study of human disease. Circ Res 111:359–374. doi:10.1161/CIRCRESAHA.111.258541
Vidal M, Cusick ME, Barabási AL (2011) Interactome networks and human disease. Cell 144:986–998. doi:10.1016/j.cell.2011.02.016
Barabási AL, Albert R (1999) Emergence of scaling in random networks. Science 286:509–512
Newman ME (2003) The structure and function of complex networks. SIAM Rev 45:167–256. doi:10.1137/S003614450342480
Clauset A, Shalizi CR, Newman ME (2009) Power-law distributions in empirical data. SIAM Rev 51:661–703. doi:10.1137/070710111
Jeong H, Mason SP, Barabási AL, Oltvai ZN (2001) Lethality and centrality in protein networks. Nature 411:41–42
Yu H, Greenbaum D, Xin LuH, Zhu X, Gerstein M (2004) Genomic analysis of essentiality within protein networks. Trends Genet 20:227–231. doi:10.1016/j.tig.2004.04.008
Goh KI, Cusick ME, Valle D, Childs B, Vidal M, Barabási AL (2007) The human disease network. Proc Natl Acad Sci 104:8685–8690. doi:10.1073/pnas.0701361104
Hidalgo CA, Blumm N, Barabási AL, Christakis NA (2009) A dynamic network approach for the study of human phenotypes. PLoS Comput Biol 5:e1000353. doi:10.1371/journal.pcbi.1000353
van Driel MA, Bruggeman J, Vriend G, Brunner HG, Leunissen JA (2006) A text-mining analysis of the human phenome. Eur J Hum Genet 14:535–542
Christakis NA, Fowler JH (2007) The spread of obesity in a large social network over 32 years. N Engl J Med 357:370–379. doi:10.1056/NEJMsa066082
Schneeberger A, Mercer CH, Gregson SA, Ferguson NM, Nyamukapa CA, Anderson RM, Johnson AM, Garnett GP (2004) Scale-free networks and sexually transmitted diseases: a description of observed patterns of sexual contacts in Britain and Zimbabwe. Sex Transm Dis 31:380–387. doi:10.1097/00007435-200406000-00012
Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE (2005) Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 62:617–627. doi:10.1001/archpsyc.62.6.617
Albert U, Rosso G, Maina G, Bogetto F (2008) Impact of anxiety disorder comorbidity on quality of life in euthymic bipolar disorder patients: differences between bipolar I and II subtypes. J Affect Disord 105:297–303. doi:10.1016/j.jad.2007.05.020
Brown TA, Antony MM, Barlow DH (1995) Diagnostic comorbidity in panic disorder: effect on treatment outcome and course of comorbid diagnoses following treatment. J Consult Clin Psychol 63(3):408
Schoevers RA, Deeg D, Van Tilburg W, Beekman A (2005) Depression and generalized anxiety disorder: co-occurrence and longitudinal patterns in elderly patients. Am J Geriatr Psychiatry 13:31–39. doi:10.1176/appi.ajgp.13.1.31
Kim SW, Yoon JS (2013) Suicide, an urgent health issue in Korea. J Korean Med Sci 28:345–347. doi:10.3346/jkms.2013.28.3.345
Cho MJ, Seoul National University of Medicine Korean Ministry of Health and Welfare (2011) The Epidemiological Survey of Mental Disorders in Korea. Seoul National University of Medicine, Seoul
Zimmerman M, Mattia JI (1999) Psychiatric diagnosis in clinical practice: is comorbidity being missed? Compr Psychiatry 40:182–191. doi:10.1016/S0010-440X(99)90001-9
Borsboom D, Cramer AO, Schmittmann VD, Epskamp S, Waldorp LJ (2011) The small world of psychopathology. PLoS One 6(11):e27407
Borsboom D, Cramer AO (2013) Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol 9:91–121
Cho MJ, Chang SM, Lee YM, Bae A, Ahn JH, Son J, Hong JP, Bae JN, Lee DW, Cho SJ, Park JI, Lee JY, Kim JY, Jeon HJ, Sohn JH, Kim BS (2010) Prevalence of DSM-IV major mental disorders among Korean adults: a 2006 National Epidemiologic Survey (KECA-R). Asian J Psychiatr 3:26–30. doi:10.1016/j.ajp.2010.01.009
Korea National Statistical Office (2006) The Report of Population and Housing Census 2005. Korea National Statistical Office, Daejeon
Korea National Statistical Office (2011) 2010 Population and Housing Census Report. Korea National Statistical Office, Daejeon
Cho MJ, Hahm BJ, Bae JN, Suh TW, Lee DW, Cho SJ, Kim JK (1999) Development of the Korean version of Composite International Diagnostic Interview. Annual Meeting of the Korean Neuropsychiatric Association Korean Neuropsychiatric Association. Korean Neuropsychiatric Association, Seoul, Korea
WHO (1997) Procedures for the development of new language versions of the WHO Composite International Diagnostic Interview (WHO-CIDI). World Health Organization, Geneva, Switzerland
WHO (1997) CIDI, Core Version 2.1 Trainer’s manual. World Health Organization, Geneva, Switzerland
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, 4th edn. American Psychiatric Association, Washington
Kessler RC (1995) The National Comorbidity Survey: preliminary results and future directions. Int J Methods Psychiatr Res 5:139–151
Cyram NI (2004) Cyram. Seoul
Gansner ER, Koren Y, North S (2005) Graph drawing by stress majorization. In: Pach J (ed) Graph drawing, Lecture notes in computer science, vol 3383. Springer, Berlin, Heidelberg, pp 239–250
Opsahl T, Agneessens F, Skvoretz J (2010) Node centrality in weighted networks: generalizing degree and shortest paths. Soc Networks 32:245–251. doi:10.1016/j.socnet.2010.03.006
Wonderlich SA, Mitchell JE (1997) Eating disorders and comorbidity: empirical, conceptual, and clinical implications. Psychopharmacol Bull 33:381–391
Özgür A, Vu T, Erkan G, Radev DR (2008) Identifying gene-disease associations using centrality on a literature mined gene-interaction network. Bioinformatics 24:i277–i285. doi:10.1093/bioinformatics/btn182
Jacobs D, Brewer M (2004) APA practice guideline provides recommendations for assessing and treating patients with suicidal behaviors. Psychiatric Annals 34:373–380. doi:10.3928/0048-5713-20040501-18
Andrews G, Henderson S, Hall W (2001) Prevalence, comorbidity, disability and service utilization. Overview of the Australian National Mental Health Survey. Br J Psychiatry 178:145–153. doi:10.1192/bjp.178.2.145
Pirkis JE, Burgess PM, Meadows GN, Dunt DR (2001) Suicidal ideation and suicide attempts as predictors of mental health service use. Med J Aust 175:542–545
Bahn GH, Kim JW, Cho AR, Park JK, Kim YJ, Park JH (2007) The status quo and problems of private health insurances for psychiatric illnesses in Korea. J Korean Neuropsychiatr Assoc 46:373–377
Helzer JE, Kraemer HC, Krueger RF (2006) The feasibility and need for dimensional psychiatric diagnoses. Psychol Med 36:1671–1680. doi:10.1017/S003329170600821X
Dalal PK, Sivakumar T (2009) Moving towards ICD-11 and DSM-V: concept and evolution of psychiatric classification. Indian J Psychiatry 51:310–319. doi:10.4103/0019-5545.58302
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Association, US
Carpenter WT (2013) RDoC and DSM-5: what’s the fuss? Schizophr Bull 39:945–946. doi:10.1093/schbul/sbt101
Hyman SE (2007) Can neuroscience be integrated into the DSM-V? Nat Rev Neurosci 8:725–732. doi:10.1038/nrn2218
Insel T, Cuthbert B, Garvey M, Heinssen R, Pine DS, Quinn K, Sanislow C, Wang P (2010) Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am J Psychiatry 167:748–751. doi:10.1176/appi.ajp.2010.09091379
Cramer AO, Waldorp LJ, van der Maas HL, Borsboom D (2010) Comorbidity: a network perspective. Behav Brain Sci 33(2–3):137–150
Acknowledgments
This work was supported by the 2011 Inje University research grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Rights and permissions
About this article

Cite this article
Choi, M., Lee, DW., Cho, M.J. et al. Disease network of mental disorders in Korea. Soc Psychiatry Psychiatr Epidemiol 50, 1905–1914 (2015). https://doi.org/10.1007/s00127-015-1106-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-015-1106-2