
Abstract
Objective
Our objective was to investigate change in prevalence rates for mental and substance abuse disorders between early adolescence and young adulthood in a cohort of indigenous adolescents who participated in an 8-year panel study.
Method
The data are from a lagged, sequential study of 671 indigenous adolescents (Wave 1) from a single culture in the Northern Midwest USA and Canada. At Wave 1 (mean age 11.3 years, Wave 4 (mean age 14.3 years), Wave 6 (mean age 16.2 years), and at Wave 8 (mean age 18.3 years) the tribally enrolled adolescents completed a computer-assisted personal interview that included DISC-R assessment for 11 diagnoses. Our yearly retention rates by diagnostic wave were: Wave 2, 94.7 %; Wave 4, 87.7 %; Wave 6, 88.0 %; Wave 8, 78.5 %.
Results
The findings show a dramatic increase in lifetime prevalence rates for substance use disorders. By young adulthood, over half had met criteria of substance abuse or dependence disorder. Also at young adulthood, 58.2 % had met lifetime criteria of a single substance use or mental disorder and 37.2 % for two or more substance use or mental disorders. The results are compared to other indigenous diagnostic studies and to the general population.
Conclusions
A mental health crisis exists within the indigenous populations that participated in this study. Innovations within current mental health service systems are needed to address the unmet demand of adolescents and families.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Although there have been recent large psychiatric epidemiological studies of American Indian (AI) adults [1], there have been just three published psychiatric diagnostic studies that included AI children and adolescents and some are now decades old. The best known is the Great Smoky Mountains Study (GSMS) which compared 323 Cherokee children aged 9, 11, and 13 years to 933 similarly aged European American children [2]. The AI children were slightly less likely than European American (EA) children to meet criteria for a psychiatric disorder; however, the AI children were significantly more likely to meet criteria for substance abuse disorder (SUD) (1.2 %) than their EA counterparts (0.1 %). The second study was of 109 Northern Plains AI adolescents aged 14–16 years (mean = 15.6 years) [3]. The Northern Plains adolescents were more likely than EA adolescents to meet 6-month criteria for attention deficit/hyperactivity disorder (ADHD), SUD, and conduct disorders (CD), but had similar or lower rates of major depressive episode (MDE) and anxiety disorders.
The third published study was our analyses of the first two diagnostic waves of the current longitudinal study of 746 Northern Midwest indigenous adolescents (i.e., AI and Canadian First Nations adolescents) [4]. We reported a dramatic increase in the prevalence of psychiatric disorders between early (mean age 11.1 years) and mid-adolescence (mean age 14.3 years). The increases were particularly pronounced for SUDs and disruptive behavior disorders. At mid-adolescence, the 12-month prevalence rates for SUDs were three times those reported in the National Survey of Drug Use and Health and rates for lifetime conduct disorder were more than twice those in the general population.
Such early onset of SUDs and psychiatric disorders is associated with emerging comorbidity during adolescence [5] and portend psychiatric and substance use problems that can reach into adulthood [6, 7]. The research reported here empirically addresses these trajectories into late adolescence (mean age 16.2 years) and early adulthood (mean age 18.3 years). It is the only longitudinal study of onset of psychiatric and substance use disorders among indigenous (American Indian and Canadian First Nations) youth from early adolescence through young adulthood.
Method
Procedures
Yearly interviews were conducted with an adolescent and at least one primary caretaker on four reservations in the Northern Midwest US and four Canadian First Nations reserves. There was a 1-year lag between study sites for data collection. Three Canadian reserves and one US reservation were added to the study 1 year after the first cohort was interviewed at three US reservations and one Canadian reserve. The interviews continued in a 1-year lagged sequence through the eight waves of data collection. After Wave 1, to reduce subject burden, the subsequent Waves 4, 6 and 8 were reserved for diagnostic interviews only. Therefore, we have diagnostic information for Wave 1 (mean age 11.1 years), Wave 4 (mean age 14.3 years), Wave 6 (mean age 16.2 years), and Wave 8 (mean age 18.3 years). We present the findings by diagnostic wave.
The research team was invited to work on these reservations/reserves by tribal councils and tribal resolutions were obtained from each reservation/reserve. As part of our agreement to work together, the researchers agreed that participating reservations/reserves would be kept confidential in published reports. These reservations/reserves did not have organized human subjects review boards, so the advisory boards appointed by the tribal councils performed this function. Once we had advisory board consensus across all of the reservations/reserves, the study procedures and questionnaires were submitted to the university institutional review board for clearance for ethically appropriate research with human subjects.
Participants
A population sample of 746 tribally enrolled adolescents aged 10–12 years (average age 11.3 years) and 971 of their parents/caretakers was recruited to participate in an eight-wave panel study conducted from 2002 to 2010 with diagnostic interviews at Waves 1, 4, 6, and 8. The overall initial response rate was 79.4 %. Yearly retention rates for the diagnostic waves were: Wave 4, 87.7 %; Wave 6, 88.0 %; and Wave 8, 78.5 %. Reservation/reserve advisory boards approved all manuscripts prior to submission for publication. The sample reported on here was reduced from that in previously published reports, in that one US reservation advisory board dissolved and therefore could not read and approve this paper. The loss of the approximately 70 cases from this reservation did not significantly change the results of these analyses. For this report, the diagnostic sample at Wave 1 consisted of 672 adolescents (334 males and 337 females).
Eligibility
Each reservation/reserve provided a list of families of tribally enrolled children aged 10–12 years. We attempted to contact all families with an enrolled child within the specified age range who lived on or proximate to (within 50 miles) the reservation or reserve. Children in foster care or staying with relatives other than their biological parents were not excluded from the study. Families were recruited through a personal visit by an indigenous interviewer at which time the project was explained to them. On the advice of elders on the advisory boards, the families were presented with a small traditional gift as a gesture of respect for giving their time when they were invited to participate. If they agreed to be interviewed, the study child and at least one caretaker each received $40 for their time when the interviews were completed.
Interviewer training
All of the interviewers on the reservations/reserves were approved by the advisory boards and were either tribal members or, in a very few cases (4 out of approximately 45 interviewers), non-members who were spouses of tribal members. The families were given the opportunity to decline particular interviewers if they were related to them or if they were otherwise uncomfortable with the interviewer. Each reservation/reserve had a local indigenous full-time interviewer supervisor who coordinated visits and provided quality control. To ensure quality of data collection, all the interviewers underwent special training for conducting computer-assisted personal interviewing (CAPI) for the diagnostic measures. The training took place on-site over a period of 3 days and included practice interviews and feedback sessions regarding interview quality. Prior to each wave of data collection, each interviewer submitted four practice diagnostic interviews for feedback. All of the interviewers completed annual required human subjects’ protection training. The training emphasized the importance of confidentiality and taught procedures to maintain the confidentiality of data.
Measures
Child diagnostic information was obtained for 11 diagnoses. The substance abuse disorders (alcohol abuse, alcohol dependence, marijuana abuse, marijuana dependence, nicotine dependence, other substance use/dependence), major depressive disorder, dysthymic disorder, generalized anxiety disorder, oppositional defiant disorder, conduct disorder, and attention deficit hyperactivity disorder modules were assessed using the Diagnostic Interview Schedule for Children-Revised (DISC-R). The diagnoses were based on algorithms for the Diagnostic and Statistical Manual-IV-TR [8]. Cultural sensitivity regarding any measures that would identify child maltreatment prohibited administering the posttraumatic stress disorder module.
The DISC-R is a highly regarded, structured interview intended for use with trained interviewers. The DISC-R has been used extensively for children aged 11 years and older [9, 10]. Test–retest reliability for self-reports of children under 11 years of age varies by diagnostic category, with younger children being particularly unreliable reporters of onset and duration of symptoms. Reliability research on various versions of the DISC indicate that parent reports are the most reliable and that combined parent–child reports are more reliable than child reports alone [11–13]. Jensen and colleagues [14] argue that although discrepant caretaker and child reports provide meaningful information in some cases (e.g., attention deficit hyperactivity disorder), child reports should be treated cautiously. We have reported combined caretaker and child reports elsewhere. [7, 15, 16] For ease of comparison of prevalence estimates across the four waves of date, we report only the adolescent reports for meeting diagnostic criteria. For this reason, the Wave 1 prevalence rates should be accorded proper caution. By Wave 4, the adolescents averaged 14.3 years, at Wave 6, 16.2 years, and at Wave 8, 18.3 years.
Impairment
For each disorder at Waves 6 and 8, adolescents were asked six questions to assess levels of impairment. Response categories for some of the impairment questions were “a lot of the time,” “some of the time,” and “hardly ever,” and for others, “very bad,” “bad,” and “not too bad.” As we did in our 2008 report [7], we calculated impairment ratings using the following criteria: (1) adolescents were given an intermediate impairment rating if they gave a response of “some of the time” or “bad” to at least one of the questions, and (2) adolescents were given a severe impairment rating if they gave a response of “a lot of the time” or “very bad” to at least one question. If an adolescent was both intermediately and severely impaired, he/she was classified as only severe to make the rating categories mutually exclusive for individual disorders.
Results
Sample characteristics
The mean per capita family income was $5,522. Approximately, 32.6 % of the adolescents resided with a single parent. Among parents/caretakers, 20.6 % had less than a high school education, 41.2 % had a high school diploma or GED, and 38.2 % had at least some college education.
Breakdown of diagnoses across the four diagnostic data points (Waves 1, 4, 6, and 8)
Table 1 presents diagnostic prevalence by study wave (confidence intervals for Waves 6 and 8 are presented in Appendix).
One or more psychiatric or substance use disorders
By Wave 8, over one-half (58.2 %) of the adolescents had met criteria for at least one psychiatric disorder and 28.1 % met criteria for a past-year disorder. More than one-third (37.2 %) met lifetime criteria for two or more disorders at Wave 8. The prevalence of two or more past-year disorders increased from Wave 1 (4.8 %) to Wave 4 (16.1 %) where they plateaued at Wave 6 (16.7 %) then declined at Wave 8 (11.8 %).
Alcohol/substance use disorders
At Wave 8, the most prevalent lifetime young adult diagnostic category was alcohol and substance use disorder (51.0 %). The most frequent lifetime substance use disorder was alcohol abuse (32.7 % at Wave 8) followed by marijuana dependence (23.7 %), nicotine dependence (19.3 %), and alcohol dependence (17.6 %). At Wave 8 there was very little lifetime abuse (1.2 %) or dependence (1.9 %) of other substances (i.e., substances other than alcohol, nicotine, or marijuana).
Past-year rates of substance abuse and dependence disorders increased between Waves 1 and 4, leveled off between Waves 4 and 6, and declined between Waves 6 and 8. There was a decline in past-year alcohol dependence (5.2 vs 4.2 %), nicotine dependence (7.9 vs 5.0 %), and marijuana dependence (10.0 vs 7.4 %) between Waves 6 and 8.
Internalizing disorders
We found very low rates of internalizing disorders. At Wave 8, only 1.5 % of the young people met past-year criteria for major depressive disorder (MDD), down from 4.6 % at Wave 6. Only 1.0 % of the adolescents were currently depressed (past month) at Wave 8 compared to 1.9 % at Wave 6. Less than 1 % met past-year criteria for generalized anxiety disorder (GAD) or dysthymic disorder (DD).
Attention deficit/hyperactivity disorder
The prevalence rates of past-year attention deficit/hyperactivity disorder (ADHD) were low across waves, ranging from 2.5 % at Wave 1 and declining to 1.4 % at Wave 6, and 1.0 % at Wave 8.
Disruptive behavior disorders
The number of adolescents meeting criteria for past-year oppositional defiant disorder (ODD) decreased between Wave 4 (4.4 %), Wave 6 (3.5 %), and Wave 8 (1.7 %). Adolescent-reported lifetime conduct disorder (CD) increased linearly across the diagnostic waves from 7.6 % at Wave 1 to 32.1 % at Wave 8. Although lifetime CD increased across time, current CD (past year) declined after peaking at 12.1 % at Wave 4 (average age 14.3 years). At Wave 6, 9.0 % of the adolescents met past-year criteria for CD; this further decreased to 1.3 % at Wave 8.
Past-year and lifetime comorbidity
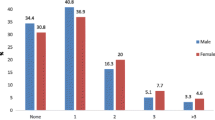
We assessed 12-month comorbidity at Wave 6 when 12-month prevalence was highest (Table 2). The adolescent males who met criteria for past-year SUD at Wave 6 were more likely also to meet criteria for CD (30.9 %) than were adolescent females (17.7 %). The SUD females, on the other hand, were more likely to also meet criteria for MDD (12.8 %) than males (6.2 %). The majority of adolescent males (75.8 %) and females (85.0 %) who met the criteria for past-year CD also met criteria for SUD. Very few adolescents met criteria for both CD and MDD, but young women with CD were more likely also to be depressed (6 females, 33.3 %) than the young men with CD (3 males, 9.1 %). Among the adolescents who met past-year criteria for MDD, 5 of the males (55.6 %) and 12 of the females (66.7 %) also met past-year criteria for SUD. Three males with MDD and six females with MDD also met past-year criteria for CD.
Tests for gender differences
We tested for gender differences among diagnostic groups of lifetime disorders: alcohol substance use disorders, disruptive behavior disorders, at least one disorder, and two or more disorders. The only statistically significant gender difference was at Wave 6 where the adolescent males were more likely to meet criteria for disruptive behavior disorders than adolescent females.
Impairment
Impairment ratings were calculated for only those adolescents who met past-year criteria for each disorder. Of the young people who met past-year criteria for alcohol dependence at Wave 8, 40.9 % indicated that they were severely impaired and 45.5 % indicated intermediate impairment (see Table 3). Almost one-half of those who met criteria for marijuana dependence at Wave 8 reported intermediate (23.1 %) or severe (23.1 %) impairment. Of the four adolescents who met criteria for GAD at Wave 8, one reported intermediate impairment and three severe impairment. At Wave 6, 27 of the adolescents who met criteria for MDD indicated impairment, 40.7 % reported intermediate and 48.1 % severe impairment. Two years later (Wave 8), five (62.5 %) of the eight young adults who met criteria for MDD reported severe impairment and the remaining three (37.5 %) reported intermediate impairment. At Wave 6, two (25 %) of the eight adolescents who met criteria for ADHD indicated that they were severely impaired by inattention and five (62.5 %) reported that they were severely impaired by hyperactivity. In addition, four (50 %) of the adolescents were intermediately impaired by inattention and one (12.5 %) by hyperactivity. Among those who met criteria for CD at Wave 6 (N = 53), 34.0 % indicated that they were severely impaired and 37.7 % were intermediately impaired.
At Wave 6, of those who met criteria for any single diagnosis, about two-thirds (62.9 %) were intermediately impaired and more than one-half (56.4 %) were severely impaired. The general trend was for decreasing impairment at young adulthood. At Wave 8, among those with caseness for any single diagnosis, 53.1 % were intermediately impaired and 38.1 % were severely impaired. Those with comorbid disorders reported high levels of impairment at both Waves 6 and 8. At Wave 6, among adolescents with two or more disorders, 77.8 % were intermediately impaired and 65.7 % were severely impaired. Among young adults (Wave 8) with comorbid disorders, 57.6 % were intermediately impaired and 59.3 % were severely impaired.
Placing the results in context
To place the results in the context of other epidemiological studies of indigenous people, we compared Wave 6 (mean age 16.2 years) and Wave 8 (mean age 18.3 years) young people and their adult parent/caregiver prevalence rates [17] to other studies of AI adolescents and adults (Table 4). There are no perfectly comparable studies matching diagnostic categories and age ranges; however, five published reports provide some perspective for our findings. (1) Beals and colleagues [3] used the Diagnostic Interview Schedule for Children, Version 2.1C, to assess 109 American Indian adolescents from a Northern Plains tribe. (2) The American Indian Service Utilization, Psychiatric Epidemiology, Risk and Protective Factors Project (AI-SUPERPFP) surveyed 15- to 54-year-old American Indians from two reservation populations [1]. This is a stratified random sample of tribally enrolled individuals from two Northern Plains tribes (n = 1,638) and one Southwest tribe (1,446). (3) The Great Smoky Mountains Study (GSMS) is a longitudinal, population-based study which included 1,420 participants who were interviewed multiple times between the ages of 9 and 21 years [2]. Our comparisons are for respondents interviewed at age 21 years. Although American Indians were oversampled in the GSMS, they were not reported separately. (4) Two reports from the National Comorbidity Survey Replication (NCS-R) provide comparisons to the general population (n = 9,282), because lifetime and 12-month prevalence were reported in separate publications [18, 19]. The comparisons are most applicable to our Wave 8 young adults. We included the Wave 6 adolescents to make the point that psychiatric diagnoses appeared to have peaked early among our study participants. We included the few diagnoses we had for the study parent/caretakers to provide intergenerational comparisons between the adolescent and parent generation.
Substance use disorders
At Wave 8, the Northern Midwest (NMW) adolescents had higher lifetime prevalence rates of SUD (51.0 %) than participants in the AI-SUPERPFP Northern Plains sample (37.0 %), even though the age range for AI-SUPERPFP was much wider (15–54 years).Prevalence of lifetime SUD among the NMW adolescents also was higher than the rates from the National Comorbidity-Replication (NCS-R) (14.6 %). Current SUD (12-months for NMW, 6 months for Beals et al.) was higher among the NMW adolescents (29.9 %) than for Beals and colleagues’ sample of Northern Plains adolescents (18.3 %) and AI-SUPERPFP (17.5 %, Northern Plains; 10.5 % Southwest). The Wave 8 adolescents’ lifetime SUD (51.0 %) was already approaching that of their parent generation (69.4 %).
At Wave 8 with an average age of about 18 years, the prevalence of lifetime alcohol dependence (17.6 %) was similar to lifetime rates of their parents/caretakers (19.6 %) and to AI-SUPERPFP Northern Plains people aged 15 years and older (16.6 %). At Wave 6, prevalence rates for combined marijuana dependence plus abuse were about twice those of the Beals and colleagues’ Northern Great Plains sample (16.2 vs 8.6 %). However, the NMW adolescents reported less abuse or dependence of substances other than alcohol or marijuana at Wave 8 (1.3 %) than those in the Beals and colleagues sample (3.9 %).
Internalizing disorders
The NMW adolescents had very low rates of past-year generalized anxiety disorder (GAD) (0.3 %, Wave 6) compared to their parents/caretakers (3.2 %), Northern Plains (1.0 %) and Southwest (1.8 %) AI people. In fact, all of the indigenous samples had lower GAD rates than those reported in the general population (5.7 %).
Twelve-month major depressive disorder (MDD) among the NMW adolescents at Wave 6 (4.6 %) was similar to the past-month MDD reported by Beals et al. (4.7 %) and to past-year prevalence among Northern Plains (4.3 %) and Southwest AI adults (6.5 %). Prevalence for MDD dropped dramatically among the NMW adolescents in Wave 8 (1.5 %). Past-year MDD among the NMW parent generation (8.1 %) was much higher than their Wave 6 or Wave 8 offspring, perhaps indicating adult onset.
Attention deficit/hyperactivity disorder
Past-year ADHD among the NMW adolescents (1.4 %) was much lower than that reported by Beals et al. (10.6 %), but very similar to that reported by Costello and colleagues [2] in the Great Smokey Mountain Study (Wave 1; 1.2 %, not shown).
Disruptive behavior disorders
Rates of past-year CD were 7.8 % for the Wave 6 NMW adolescents compared to 3.8 % in the Beals et al., Northern Great Plains; and Costello et al., GSMS, 6.5 % (not shown). The prevalence of past-year NMW CD dropped dramatically between Waves 6 and 8.
Prevalence rates across diagnoses
At Wave 6, approximately one-half (51.4 %) of the adolescents met criteria for at least one disorder. This had increased to 58.2 % by Wave 8, approaching the lifetime rates of their parents/caretakers (71.8 %) and slightly exceeding the rates for a single psychiatric disorder in general population studies (46.4 %). This is congruent with other research that indicates the adolescent onset of most psychiatric disorders [18]. Approximately, one-third of the NMW young adults (37.2 %) and their parents/caretakers (37.0 %) met criteria for two or more lifetime disorders. Again, the prevalence rate for comorbid disorders is higher than comorbidity rates found in the general population (27.7 %).
Discussion
We see a pattern of early-onset behavioral disorders (primarily conduct disorder) that emerge prior to SUDs until mid-adolescence, at which point new cases of SUD accelerate and behavioral disorders essentially plateau. Disruptive behavior disorders and SUDs account for much of the early psychopathology as opposed to internalizing disorders, such as generalized anxiety disorders and mood disorders. Moreover, disruptive behavior disorders are highly comorbid with SUDs, perhaps a consequence of emerging earlier. Our findings are congruent with years of earlier work showing early onset of substance abuse among indigenous adolescents [20–22], but they extend these findings to the diagnostic level for early onset of SUDs. Kessler [18] has pointed out that SUDs are often the last diagnoses to emerge, usually in the early twenties. For these adolescents, SUDs emerge much earlier. Our results also refine previous findings by demonstrating the interrelationship of early behavioral disorders and SUDs.
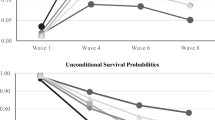
There were few new diagnoses after an average age of about 16 years. Lifetime prevalence rates peaked at an average age of 16.2 years (Wave 6) and leveled off at an average age of 18.3 years (Wave 8). This is particularly apparent with regard to past-year prevalence rates. In nearly all of the diagnostic categories there was a decline in past-year prevalence between Waves 6 and 8. This was most evident for disruptive behaviors (e.g., CD, ODD) and to a lesser extent the SUDs. Meeting criteria for any past-year disorder declined from 34.1 % at Wave 6 to 28.1 % at Wave 8, and for two or more past-year disorders from 16.7 to 11.3 %.
The patterns of impairment suggest that the diagnoses seriously affect the life of the adolescents. This is particularly true for alcohol dependence where at Wave 8, 40.9 % reported severe impairment and 45.5 % intermediate impairment. Although there were few cases of generalized anxiety disorder and major depressive disorder in the later waves of the study, the adolescents who met criteria for these diagnoses tended to rate their symptoms as severe. In general, those meeting criteria for a single disorder in Wave 8 were more likely to rate their symptoms as intermediate (53.1 %) than severe (38.1 %). Those with two or more disorders were more likely to report severe symptoms (59.3 %).
Like most studies that focus on indigenous children and adolescents, this research was limited to a single culture. The results may not be generalizable to other indigenous cultures and perhaps not even to urban indigenous people in this same culture. Diagnostic measurement is also a concern [23]. It is possible that behavioral measures such as those for SUD and disruptive behaviors are more valid in this culture than measures pertaining to feelings and emotional states. This may account for our low rates of mood and anxiety disorders. This is a non-trivial concern that suggests cross-cultural differences in internalization disorders may be affected by culturally insensitive or inappropriate measures, an area that that we believe needs increased scrutiny [24]. Regardless of whether we are underestimating internalizing disorders, the prevalence and early onset of externalizing disorders and SUDs have important policy and prevention implications.
Also, this is a community-based participatory research. Almost all of the interviewers were conducted by enrolled tribal members from the participating communities. Although the families were given the opportunity to decline particular interviewers if they were related to them or if they were otherwise uncomfortable with the interviewer, local interviewers may have resulted in underreporting and may have introduced a conservative bias.
There is the additional concern that at Wave 8 we continued to use the diagnostic criteria for CD for adolescents who had become older than 18 years. This calls into question the age appropriateness of the CD diagnoses. Only seven (7.3 %) of the Wave 8 young people met past-year criteria for CD. Six of the seven were aged 17 or 18 years; only one was aged 19 and this individual had met criteria for past-year CD in previous waves. For lifetime CD, all of the young people over the age of 18 years who met lifetime criteria had met criteria in previous waves. No new cases of CD emerged after 18 years.
A final concern is the small decrease in prevalence rates for some diagnoses between Wave 6 and 8 (Table 1). The decreases across age cohorts (Table 1) are the result of the timing of the interviews. Diagnostic interviews were not conducted at every wave of data collection, but rather at Waves 1, 4, 6, and 8. At Wave 1 the adolescents were between the ages of 10 and 13 years. Because of the timing of subsequent interviews across a changing age range of the adolescents, we do not have estimates of mental and substance use disorders at every age for each adolescent.
Conclusions
The strong linkages between disruptive behavior disorders and SUDs suggest that indexed behavioral interventions should begin in early childhood when they are first identified. Based on our results, we would argue for two levels of interventions. First, we recommend very early and ongoing indexed interventions directed at early childhood behavioral problems. Second, because early use is the strongest predictor of meeting criteria for alcohol dependence during adolescence [18], we recommend universal prevention programs beginning at pre-adolescence and repeated throughout early adolescence with the goal of delaying early experimentation and transition to regular use.
We should note that the findings reflect evidence of adolescent resilience and some cause for optimism. Although we have lingering concerns about measurement of internalizing disorders among indigenous people, the rates of internalizing disorders are very low. Also, the low rates of substance abuse other than nicotine, alcohol, and marijuana indicate adolescents have not progressed to harder drug use. Finally, the decrease in past-year diagnoses in Wave 8 may reflect emergence of healthier young adults after a period of mid-adolescent problems.
In summary, we found a peak in behavioral disorders in mid-adolescence and escalating SUDs into young adulthood. Of primary concern is that these adolescents are beginning to use substances early and their use is to such a degree that they are meeting diagnostic criteria. This is a serious public health issue that portends long-term consequences. The problem has been documented now at multiple levels [20–22]. There remains an urgent need for research that addresses the specific mechanisms at work that account for the early-onset SUDs and disruptive behavior disorders among indigenous adolescents. Finally, our findings regarding the late adolescent–early adulthood leveling off of new diagnoses needs replicating, to be certain this finding was not a design or measurement artifact.
References
Beals J, Manson SM, Whitesell NR, Spicer P, Novins DK, Mitchell CM (2005) Prevalence of DSM-IV disorders and attendant help-seeking in 2 American Indian reservation populations. Arch Gen Psychiatry 62(1):99–108
Costello EJ, Angold A, Burns BJ et al (1996) The Great Smoky Mountains study of youth: goals, design, methods, and the prevalence of DSM-III-R disorders. Arch Gen Psychiatry 53(12):1129–1136
Beals J, Piasecki J, Nelson S et al (1997) Psychiatric disorder among American Indian adolescents: prevalence in Northern Plains youth. J Am Acad Child Psychiatry 36(9):1252–1259
Whitbeck LB, Yu M, Johnson KD, Hoyt DR, Walls ML (2008) Diagnostic prevalence rates from early to mid-adolescence among indigenous adolescents: first results from a longitudinal study. J Am Acad Child Psychiatry 47(8):890–900
Angold A, Costello E (2001) The epidemiology of depression in children and adolescents. In: Goodyer I (ed) The depressed child and adolescent, 2nd edn. Cambridge University Press, New York, pp 143–178
Harrington R, Fudge H, Rutter M, Pickles A, Hill J (1990) Adult outcomes of childhood and adolescent depression: I. Psychiatric status. Arch Gen Psychiatry 47(5):465–473
Lewinsohn P, Rohde P, Klein D, Seeley J (1999) Natural course of adolescent major depressive disorder: I. Continuity into young adulthood. J Am Acad Child Adolesc Psychiatry 38(1):56–63
American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders, fourth edition, text revision. American Psychiatric Association, Washington
Shaffer D, Schwab-Stone M, Fisher P et al (1993) The diagnostic interview schedule for children—revised version (DSC-R): I preparation, field testing, interrater reliability, and acceptability. J Am Acad Child Psychiatry 32(3):643–650
Shaffer D, Schwab-Stone M, Fisher P et al (1988) A revised version of the diagnostic interview schedule for children DISC-R): results of a field trial and proposals for a new instrument (DISC-2). Epidemiology and Psychopathology Research Branch, Division of Clinical Research, National Institute on Mental Health, Rockville
Schwab-Stone ME, Schwab D, Dulcan MK et al (1996) Criterion validity of the NIMH diagnostic interview schedule for children version 2.3 (DIS-2.3). J Am Acad Child Psychiatry 35(7):878–888
Shaffer D, Fisher P, Dulcan MK et al (1996) The NIMH diagnostic interview schedule for children version 2.3 (DISC-2.3): description, acceptability, prevalence rates, and performance in the MECA study. Methods for the epidemiology of child and adolescent mental disorders study. J Am Acad Child Psychiatry 35(7):865–877
Jensen P, Roper M, Fisher P et al (1995) Test–retest reliability of the diagnostic interview schedule for children (DISC 2.1) parent, child, and combined algorithms. Arch Gen Psychiatry 52(1):61–71
Jensen PS, Rubio-Stipec M, Canino G et al (1999) Parent and child contributions to diagnosis of mental disorder: are both informants always necessary? J Am Acad Child Psychiatry 38(12):1569–1579
Whitbeck LB, Hoyt D, Johnson K, Chen X (2006) Mental disorders among parents/caretakers of American Indian early adolescents in the northern midwest. Social Psychiatry Psychiatr Epidemiol 41(8):632–640
Whitbeck L, Yu M, Johnson K, Hoyt D, Walls M (2008) Diagnostic prevalence rates from early to mid-adolescence among indigenous adolescents: first results from a longitudinal study. J Am Acad Child Adolesc Psychiatry 47(8):890–900
Bird HR, Gould MS, Staghezza B (1992) Aggregating data from multiple informants in child psychiatry epidemiological research. J Am Acad Child Psychiatry 31(1):78–85
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 62(6):593–602
Kessler RC, Chiu WT, Demler O, Walters EE (2005) Prevalence, severity and comorbidity of twelve-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 62(6):612–627
Bachman JG, Wallace JM, O’Malley PO et al (1991) Racial/ethnic differences in smoking, drinking, and illicit drug use among American high school seniors, 1967–1989. Am J Pub Health 81(3):372–377
Blum RW, Harmon B, Harris L et al (1992) American Indian–Alaska native youth health. JAMA 267(12):1637–1644
Cheadle JE, Whitbeck LB (2011) Alcohol use trajectories and problem drinking over the course of adolescence: a study of North American indigenous youth and their caretakers. J Health Soc Behav 52(2):228–245
Dingwall KM, Cairney S (2010) Psychological and cognitive assessment of indigenous Australians. Aust N Z J Psychiatry 44(1):20–30
Armenta BE, Sittner Hartshorn KJ, Whitbeck LB, Crawford DM, Hoyt DR. A longitudinal examination of the measurement properties and predictive utility of the center for epidemiologic studies depression scale among North American indigenous adolescents. Psychol Assess (in press)
Acknowledgments
This research was funded by the National Institute on Drug Abuse (DA13580) and the National Institute of Mental Health (MH67281).
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
See Appendix Table 5.
Rights and permissions
About this article
Cite this article
Whitbeck, L.B., Sittner Hartshorn, K.J., Crawford, D.M. et al. Mental and substance use disorders from early adolescence to young adulthood among indigenous young people: final diagnostic results from an 8-year panel study. Soc Psychiatry Psychiatr Epidemiol 49, 961–973 (2014). https://doi.org/10.1007/s00127-014-0825-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-014-0825-0