
Abstract
Background
Evidence indicates that an adverse psychosocial work environment contributes to the explanation of depressive symptoms. Research was mainly informed by two theoretical models, the demand-control and the effort-reward imbalance model. Yet, a comparative analysis of the two models, using original scales, has not yet been conducted in an unselected working population.
Methods
A total of 1,811 working men and women from the baseline screening of an epidemiological cohort study were interviewed (job stress, depressive symptoms [CES-D], health behaviours, medical history, socio-demographic characteristics). Logistic regression models were calculated to estimate associations between depressive symptoms, the two job stress models and relevant covariates.
Results
Analyses showed significantly increased multivariate odds ratio (OR) of job strain and effort-reward imbalance. When the two models were mutually adjusted control [OR, 95%CI = 1.9, 1.3–2.7], effort-reward imbalance [OR, 95%CI = 3.4, 2.1–5.1] and overcommitment OR, 95%CI = 3.9, 2.7–5.8] were independently associated with depressive symptoms Additional tests of interaction between the models revealed relatively highest level of depressive symptoms in employees who simultaneously reported low control and high overcommitment.
Conclusions
Components of an adverse psychosocial work environment are associated with depressive symptoms in an unselected working population. Policy implications of accumulated evidence on this relation should be addressed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Evidence indicates that an adverse psychosocial work environment contributes to the explanation of depressive symptoms including major depressive episodes in initially healthy populations. This has been demonstrated for two models that specify an adverse psychosocial work environment in stress-theoretical terms, the demand-control model [13] and the effort-reward imbalance model [26]. The focus of the former model is on a specific combination of job task characteristics, i.e. high quantitative psychological demands and a low degree of control over one’s tasks, a combination that prevents the experience of autonomy of the working person. The latter model is concerned with the reciprocity of a contractual exchange at work where efforts are compensated by adequate rewards in terms of money, career opportunities including job security and esteem. Lack of reciprocity (high effort and low reward) is relatively frequent in modern economy and may elicit strong stress reactions due to the fact that a basic principle of social exchange is violated.
Several cross-sectional and prospective investigations found partial or full support by analysing the components of the demand-control [8, 14, 18–20, 29, 32–34] or the effort-reward imbalance model [7, 15, 16, 18, 21, 29, 30] respectively. However, few studies so far examined the two models simultaneously with regard to depression although this approach is important at least for two reasons. First, the models identify complementary aspects of a stressful work environment and, thus, offer the opportunity to evaluate the relative strength of each association with the outcome under study. Secondly, if either model is associated with depression, a more comprehensive set of worksite intervention measures needs to be developed for preventive reasons, in particular for people whose work environment is characterised by features of the demand-control and the effort-reward imbalance model.
To our knowledge, four studies explored the association of the two models with depression so far, but each one has limitations. One study used proxy measures of the job stress models [29], a second study was restricted to a relatively small sample of 190 working men of a car producing company in Japan [30] and a third investigation analysed these associations in a sample of some 1,168 middle-aged working men and women from central and eastern Europe [21], but included partial measures of the two models only (no measures of ‘demands’ and of ‘overcommitment’). Finally, a most recent investigation was restricted to employees working in a specific company that was subjected to a major organisational change [18].
Therefore, this study sets out to analyse the association between either job stress model and depressive symptoms (1) by using the original scales measuring the models, (2) by testing the hypothesis in an unselected population drawn from a random sample on the basis of urban citizen registries (thus representing a variety of occupations), and (3) by adjusting for important confounders including the effect of a possible reporting bias. Furthermore, (4) interaction between components of the two work stress models are analysed with respect to risk of depressive symptoms.
Methods
Sample
Data were collected during the baseline examination of the Heinz Nixdorf Recall (HNR) Study, an ongoing prospective population-based cohort study in Germany (for rationale and design see Schmermund et al. [25]). The study base was the general German population aged 45–74 years, living in three cities in an industrialized urban region (Ruhr Area). Participants were recruited out of a random sample derived from mandatory citizen registries. A total of 4,814 men and women agreed to participate, which corresponds to a response proportion of 55.8%. Details about the sample, the recruitment method, non-responder characteristics and possible sources of bias are presented elsewhere [28].
For this investigation, we restricted the sample to working individuals with a regular working time of at least 15 h a week and an age below the official retirement age of 66 years. A total of 1,811 persons met these criteria (37.6% of total), 1,070 men and 741 women.
Data collection
Although the main focus of the HNR Study is to clarify the value of subclinical coronary calcification as a predictor of cardiac events during follow-up, a variety of biomedical, behavioural, psychosocial and socio-economic risk factors were assessed as well. For the analyses presented in this article we used information from computer-assisted-personal interviews, paper and pencil questionnaires which were accomplished during the baseline screening, taking place from December 2000 to August 2003 in a study site at the University Clinic in Essen. To guarantee a high quality of data, a far-reaching quality assurance strategy had been applied. The interviewer staffs of students, nurses and medical doctors were intensively trained. Furthermore, the study design was reviewed by an international panel of experts and, in addition to continued external monitoring, an official certification was achieved (DIN EN ISO 9001:2000).
Depressive symptoms
Participants filled in the Center for Epidemiological Study-Depression Survey (CES-D) questionnaire in a 15 item version [9, 22]. This frequently applied screening instrument contains questions about the 7-day incidence of different types of depressive symptoms (sample questions: “during the past week I felt sad” or “during the past week I felt fearful”). Answers are given on a 4-point Likert-scale ranging from “less than one day” (0) to “5–7 days” (3). We calculated a sum score of all items with a range of 0–45, with higher values indicating higher symptom load. The internal consistency of the questionnaire was appropriate (Cronbach’s alpha for the whole sample = 0.86; men = 0.83; women = 0.88). However, as the score was not normally distributed we calculated logistic instead of linear regression models. For this purpose the score was dichotomised. Using gender specific cutpoints, participants with values in the upper quartile of the distribution in our sample were defined as exposed, i.e. as suffering from depressive symptoms. This distribution-based cut-off point was chosen because the distribution of the CES-D scores in this sample of working men and women differed from the reference population for the instrument (where a cut-off point of 17 was proposed) [9].
Job stress models
Both job stress models were measured by validated questionnaires. The demand-control model was operationalised by 16 items from the job content questionnaire [12, 13], where the dimensions of control and demand were assessed by 8 items respectively. Scales were constructed by summing up the answers for each dimension. A job strain variable was constructed by dichotomising the two scales (median) and combining them into one variable with the categories ‘no strain (low demands and high control)’, ‘active job (high demands and high control)’, ‘passive job (low demands and low control)’ and ‘job strain (high demands and low control)’. As in previous studies [15, 18, 21, 29, 30], the two scales were also analysed separately. Continuous scores of each scale were transformed into four exposure levels by using gender-specific quartiles as cut-off points. These categorical variables entered multivariate logistic regression, with the lowest exposure level (low demands/high control) as reference category.
The effort-reward imbalance model distinguishes between two main sources of stressful experience at work, an extrinsic component defined by perceived efforts and experienced or anticipated rewards; and an intrinsic component which identifies a motivational pattern of work-related overcommitment [26, 27]. The first component is measured by 17 items (scale effort: 6 items; scale reward: 11 items). To mirror the core theoretical notion of nonreciprocal exchange at work, a ratio of these two scales was constructed according to established recommendations [27]. Overcommitment was measured by a unidimensional scale of 6 items. Again, exposure levels of the two scores were defined by quartiles.
Covariates
We added a set of covariates to the multivariate regression models. Gender and age were introduced because they are standard risk factors of depression. Furthermore, education and occupational status were added as indicators of socio-economic position. Education was classified according to the International Standard Classification of Education [31] as total years of formal education, combing school, and vocational training. A crude measure of occupational status describes whether participants are blue-collar workers, white-collar workers or self-employed. Additionally, average working hours per week were introduced as a covariate to adjust for exposure duration of work-related stress. Concerning nonworking life, an important factor related to mental health was included, social integration. The social integration index [1] is a composite measure of social activities and integration into family and community life. It includes different types of social contacts (partnership, family members, friends and participation in voluntary organisations). As chronic disease may affect mood and, thus, produce a response bias, a score of five highly prevalent chronic disease conditions was constructed (history of coronary heart disease or stroke, diabetes, hypertension, hypercholesterolaemia) and included into multivariate analysis. Finally, cigarette smoking (“former—current—never smoker”) and physical inactivity (less than once a week regular sports) were selected as relevant behavioural covariates.
Data analyses
As mentioned, we calculated multivariate logistic regression models with the dichotomised CES-D score as a dependent variable to examine statistical relationships between job stress and depressive symptoms. Covariates were added to the models consecutively, starting with gender and age and ending with a fully adjusted model. In the first step, the two models were analysed separately. Thereafter, both models were simultaneously included to estimate their independent effects.
Interaction was tested using the method described by Rothmann [23]. A combined exposure variable was computed by combining the high exposure categories of two variables, e.g. the control scale and the effort-reward-ratio. A synergy index was calculated to test if the combined exposure significantly exceeds the additive effect of the two single exposures [4]. An index >1 indicates a synergistic interaction. All calculations were done with the SPSS statistical package 12.0.1.
Results
The distribution of the dependent and independent variables is given in Tables 1 and 2. We should add that 26.3% (N = 468) of the participants had depression scores in the upper quartile.
Table 3 shows the associations between the five indicators of job stress and depressive symptoms: a higher exposure to job stress is associated with a higher symptom load. The relative differences are mostly similar in both sexes, therefore the following results refer to the whole sample. Bivariate findings are further proved using multivariate regression. In Table 4 estimations of the strength of association of either job stress model with depressive symptoms are given.
Odds ratios in the first and the second column are derived from separate regression analyses for each job stress component. Job strain and its components of low control and high demand are significantly related to depressive symptoms where the probability of exhibiting high depressive symptom load increases with a decreasing control score and an increasing demand score. Estimators are only slightly affected by additional adjustment for covariates. Results of the complementary job stress model are comparable. The higher the imbalance between effort and reward, and the higher the degree of overcommitment, the higher the odds ratios of reporting a high number of depressive symptoms. Again, adjustment for covariates does not reduce these strong effects.
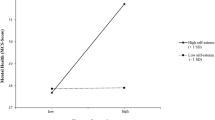
The third column shows the results of a regression model in which all components are entered simultaneously. An exception is job strain which is not additionally adjusted for its sub-components. It is obvious that all odds ratios are reduced in this analysis. Job strain and the demand scale were no longer associated with depressive symptoms. Low control, effort-reward-imbalance, and overcommitment remained significantly related to symptoms, indicating that they have independent relationships to the outcome measure. For the three remaining variables, we conducted further analyses to test possible interaction effects on depressive symptoms. Two models were analysed, first a combination of low control and the effort-reward-ratio, second, a combination of low control and overcommitment. Results are shown in Table 5. Employees who were exposed to low control and effort-reward imbalance had a higher odds ratio of depressive symptoms compared to those who reported only a single or no exposure, but this combination did not exceed the additive effect of either condition. In contrast, a synergistic interaction of low control and high overcommitment was observed.
Discussion
This study documented strong associations of the extrinsic and intrinsic component of the effort-reward-imbalance model with depressive symptoms in a sample of an unselected working population. In addition, low control, but not high demand and job strain at work was associated with depressive symptoms as well when both models were analysed simultaneously. Furthermore, a synergistic interaction between overcommitment and low control was found when a combined exposure to both components was studied. Results were largely comparable for men and women when gender specific analyses were additionally performed (results not shown). Extensive adjustment did not alter the findings. For all job stress components with significant effects, a stepwise increase in odds ratios from lower to higher quartiles was observed. The same holds true for analyses based on the cut point for clinical depression although confidence intervals were large due to a small number of cases [10].
Our finding of an association of effort-reward imbalance with depression is in accordance with the results of previous reports, three prospective [7, 15, 29] and four cross-sectional studies [16, 18, 21, 30]. Although three of these investigations used proxy or incomplete measures, this convergence of results adds to the robustness of the observed relationship.
As mentioned in the Introduction, four studies tested the effort-reward-imbalance and demand-control models simultaneously. Findings of our investigation are in line with those reported by Niedhammer et al. [18] and Tsutsumi et al. [30]. They both observed an effect of low control, but not of high demand at work with depression after adjusting for the alternative model. In a third study, the effect of low control disappeared after adjusting for socio-economic factors, whereas the effect of effort-reward imbalance remained significant [21]. Unfortunately, the only report documenting independent effects of high demand, low control (decision authority), and effort-reward imbalance is based on proxy measures and cannot be compared in a strict sense [29]. Yet, it should be mentioned that several investigations found significant relations of both components, demand and control, with depression without including the complementary effort-reward imbalance model [8, 14, 19, 20, 32–34]. Moreover, we may have underestimated the contribution of this model to some extent as we did not include a third dimension, social support at work, that is sometimes considered an additional model component [12].
The fact that the present study is the first to test the two models with original scales in an unselected population covering a wide range of different occupations adds to the validity of previous findings which were restricted to specific occupational groups [18, 29, 30]. Given the independent and combined effects of components of the two models, we recommend using both measures of psychosocial stress at work in future studies.
Despite this degree of concordance, this study suffers from several limitations. First, due to its cross-sectional design an inference concerning a causal direction of the association is problematic. We cannot exclude reverse causation where respondents with depressive symptoms perceive their psychosocial work environment as particularly stressful. At best, we can conclude that results concur with those obtained from prospective observational studies [7, 15, 19, 29].
Furthermore, we were not able to adequately control for bias due to common method variance [11] as no alternative measure of health was available. To approximate the possible bias, we included a measure of negative affectivity [2] in the regression analysis to explore the effect of a response style that may underlie the observed association (results not shown). This additional adjustment reduced the odds ratios for the main job stress measures, but they remained significantly elevated. This result indicates that common method variance does not fully explain the relationship between job stress and depressive symptoms in our study. On the other hand, given a high correlation of negative affectivity with depression, we may run the risk of overadjustment.
Another possible source of bias is a selection bias due to nonresponse of eligible subjects. We conducted a number of nonresponse analyses published in a former article [28] which showed that the sample has a good external validity. Nonetheless, possible bias could not be ruled out and should be acknowledged when interpreting the results.
A further limitation is the lack of a more comprehensive analysis that includes interactions between work and family life [33], an issue of future exploration. Finally, it would have been interesting to include biological markers of risk for depression, such as polymorphism of the 5-HT gene, in order to test gene-environment interaction in relation with depression [3].
These limitations are balanced by several strengths. First, we applied validated scales to measure independent and dependent variables and we performed state of the art analyses with careful adjustments including a range of important confounders. Second, our findings are based on an unselected sample of middle-aged to early-old age working men and women from a variety of occupations. Therefore it is unlikely that the observed odds ratios are due to a specific occupational or socio-economic subgroup within this sample. Third, particular emphasis was put on high quality performance in gathering the data. We used computer-assisted personal interview to assess the two job stress models, and interviewer underwent an extensive training to avoid known sources of systematic bias.
Conclusion
In conclusion, this investigation provides additional evidence of a strong association of components of an adverse psychosocial work environment with depressive symptoms. An imbalance between high efforts spent and low rewards received at work, a pattern of overcommited work-related motivation, and a low degree of task control were repeatedly found to increase the risk of depressive symptoms.
In view of the significant impact of reduced mental health on work performance [6, 17] and health costs [5] and in view of a relevant comorbidity of depression with several highly prevalent cardiovascular and metabolic health risks [24] preventive efforts are justified. These efforts concern an increased awareness of physicians in assessing psychosocial risks of depressive symptoms and in counselling and supporting their patients. Even more important, measures of worksite health promotion instructed by available scientific evidence, should be intensified.
References
Berkman LF, Melchior M, Chastang JF, Niedhammer I, Leclerc A, Goldberg M (2004) Social integration and mortality: a prospective study of French employees of Electricity of France-Gas of France: the GAZEL Cohort. Am J Epidemiol 159:167–174
Bradburn NM (1969) The structure of well-being. Chicago
Caspi A, Sugden K, Moffitt TE, Taylor A, Craig IW, Harrington H, McClay J, Mill J, Martin J, Braithmaite A, Poulton R (2003) Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 301:386–389
Dragano N, Verde PE, Siegrist J (2005) Organisational downsizing and work stress: testing synergistic health effects in employed men and women. J Epidemiol Commun Health 59:694–699
Eurostat (2004) Work and health in the EU. A statistical portrait. Office for official publications of the European Communities, Luxembourg
Faragher EB, Cass M, Cooper CL (2005) The relationship between job satisfaction and health: a meta-analysis. Occup Environ Med 62:105–112
Godin I, Kittel F, Coppieter Y, Siegrist J (2005) A prospective study of cumulative job stress in relation to mental health. BMC Public Health 15:67
Griffin JM, Fuhrer R, Stansfeld SA, Marmot M (2002) The importance of low control at work and home on depression and anxiety: do these effects vary by gender and social class? Soc Sci Med 54:783–798
Hautzinger M, Bailer M (1993) A global depression scale (German). Beltz Test GmbH, Weinheim
He Y (2005) Prevalence of depressive disorders in a working population and associations with work stress [German]. Unpublished dissertation, Medical Faculty University Duesseldorf, Duesseldorf
Judge TA, Erez A, Thoresen CJ (2000) Why negative affectivity (and self-deception) should be included in job stress research: bathing the baby with the bath water. J Organiz Behav 21:101–111
Karasek RA, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B (1998) The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol 3:355
Karasek RA, Theorell T (1990) Healthy work. Stress, productivity and the reconstruction of working life. Basic Books, New York
Kawakami N, Haratani T, Araki S (1992) Effects of perceived job stress on depressive symptoms in blue-collar workers of an electrical factory in Japan. Scand J Work Environ Health 18:195–200
Kivimaki M, Vahtera J, Elovainio M, Virtanen M, Siegrist J (2007) Effort-reward imbalance, procedural injustice and relational injustice as psychosocial predictors of health: complementary or redundant models? Occup Environ Med, Epub ahead of print, January 25:doi: 10.1136/oem.2006.031310
Larisch M, Joksimovic L, von dem Knesebeck O, Starke D, Siegrist J (2003) Effort-reward imbalance at work and depressive symptoms-a cross-sectional investigation of middle-aged employees. [German]. Psychother Psychosom Med Psychol 53:223–228
Meerding WJ, IJzelenberg W, Koopmanschap MA, Severens JL, Burdorf A (2005) Health problems lead to considerable productivity loss at work among workers with high physical load jobs. J Clin Epidemiol 58:517–523
Niedhammer I, Chastang JF, David S, Barouhiel L, Barrandon G (2006) Psychosocial work environment and mental health: job-strain and effort-reward imbalance models in a context of major organizational changes. Int J Occup Environ Health 12:111–119
Niedhammer I, Goldberg M, Leclerc A, Bugel I, David S (1998) Psychosocial factors at work and subsequent depressive symptoms in the Gazel cohort. Scand J Work Environ Health 24:197–205
Paterniti S, Niedhammer I, Lang T, Consoli SM (2002) Psychosocial factors at work, personality traits and depressive symptoms. Longitudinal results from the GAZEL Study. Br J Psychiatry 181:111–117
Pikhart H, Bobak M, Pajak A, Malyutina S, Kubinova R, Topor R, Sebakova H, Nikitin Y, Marmot M (2004) Psychosocial factors at work and depression in three countries of Central and Eastern Europe. Soc Sci Med 58:1475–1482
Radloff LS (1977) The CES-D Scale: a self-report depression scale for research in the general population. Appl Psychol Measure 1:385–401
Rothman KJ (1986) Modern epidemiology. Little, Brown, Boston
Rudisch B, Nemeroff CB (2003) Epidemiology of comorbid coronary artery disease and depression. Biol Psychiatry 54:227–240
Schmermund A, Möhlenkamp S, Stang A, Grönemeyer D, Seibel R, Hirche H, Mann K, Siffert W, Lauterbach K, Siegrist J, Jöckel KH, Erbel R (2002) Assessment of clinically silent atherosclerotic disease and established and novel risk factors for predicting myocardial infarctin and cardiac death in healthy middle-aged subjects: rationale and design of the Heinz Nixdorf Recall Study. Am Heart J 144:212–218
Siegrist J (1996) Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol 1:27–41
Siegrist J, Starke D, Chandola T, Godin I, Marmot M, Niedhammer I, Peter R (2004) The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med 58:1483–1499
Stang A, Moebus S, Dragano N, Beck E, Möhlenkamp S, Schmermund A, Siegrist J, Erbel R, Jöckel K (2006) Baseline recruitment and analyses of nonresponse of the Heinz Nixdorf Recall Study: identifiability of phone numbers as the major determinant of response. Eur J Epidemiol 20:489–496
Stansfeld SA, Fuhrer R, Shipley MJ, Marmot MG (1999) Work characteristics predict psychiatric disorder: prospective results from the Whitehall II Study. Occup Environ Med 56:302–307
Tsutsumi A, Kayaba K, Theorell T, Siegrist J (2001) Association between job stress and depression among Japanese employees threatened by job loss in a comparison between two complementary job-stress models. Scand J Work, Environ Health 27:146–153
UNESCO (1997) International Standard Classification of Education. ISCED 1997. UNESCO, Paris
Wang J (2004) Perceived work stress and major depressive episodes in a population of employed Canadians over 18 years old. J Nerv Ment Dis 192:160–163
Wang J (2006) Perceived work stress, imbalance between work and family/personal lives, and mental disorders. Soc Psychiatry Psychiatr Epidemiol 41:541–548
Wang J, Patten SB (2001) Perceived work stress and major depression in the Canadian employed population, 20–49 years old. J Occup Health Psychol 6:283–289
Acknowledgements
We thank the Heinz Nixdorf Foundation (Chairman: Dr. jur. G. Schmidt, Essen, Germany) for the sponsoring of this study. This study is also supported by the German Ministry of Education and Science. We are indebted to the investigative group and the study personnel of the Heinz Nixdorf Recall Study, in particular EM Beck, IMIBE, Dr. GF Matysik, and Dr. M Bröcker from the Dept. of Clinical Chemistry and Laboratory Medicine. Finally we thank the German Research Council (DFG; Project SI 236/8-1) for sponsoring additional assessment of psychosocial factors.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Dragano, N., He, Y., Moebus, S. et al. Two models of job stress and depressive symptoms. Soc Psychiat Epidemiol 43, 72–78 (2008). https://doi.org/10.1007/s00127-007-0267-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-007-0267-z