
Abstract
Objectives
There are currently around 120 million rural–urban migrants in China. Elsewhere migration has been associated with increased vulnerability to mental health problems. This study was conducted to explore the mental health status and help seeking behaviours of migrant workers in Hangzhou city, Zhejiang Province, and to compare them with permanent urban and rural dwellers.
Methods
A self-completion questionnaire including items relating to sociodemographics, health and lifestyles and mental health, was completed by 4453 migrant workers and 1957 urban workers in Hangzhou city, and by 1909 rural residents in Western Zhejiang Province.
Results
The mean age of the migrants was 27 years, (male 29 years, female 25 years). They worked long hours (28% >12 h per day, 81% 6 or 7 days per week) and their living conditions were very basic. On the SF-36 mental health scale migrants had lower scores (52.4) than rural residents (60.4, P < 0.0001) but scored higher than urban residents (47.2, P = 0.003). The difference between urbanites and migrants disappeared after adjustment for confounders (P = 0.06). Independent predictors of better mental health status among migrants were being unmarried, migrating with a partner, higher salary, good self-reported health and good relationships with co-workers. There were small significant differences in suicide ideation and attempts between the three groups with suicide ideation commonest in migrants and suicide attempts most common in the rural population. Fewer than 1% across all three groups had received any professional help for depression or anxiety.
Conclusion
Rural–urban migrant workers in this part of China are not especially vulnerable to poor mental health. This may result from a sense of well being associated with upward economic mobility and improved opportunities, and the relatively high social capital in migrant communities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Rural-to-urban migration takes place in China on a massive scale. Numbers have increased from 50 million in 1990 to 120 million in 2000 and by 2010 there are expected to be around 160 million [18], accounting for around 25% of the working population of the whole country. Migrants provide an important mechanism to cope with fluctuating labour demand in urban sectors and with surplus rural labour. They make a major contribution to China’s industrial development, inflow of foreign investment and economic growth. Their remittances support the rural economy, accounting for over 5% of the GDP of some poor provinces [21]. Because of the Chinese system of household registration or hukou, rural–urban migrants are classified as temporary residents in cities, irrespective of their length of stay. By law all individuals must have household registration or hukou, which ensures certain rights (such as free education and access to social welfare) in the place where the registration is held. With very few exceptions migrants keep their rural hukou. This means, not only that they are denied some citizens’ rights at their urban destination, but also that they have a lower status than their urban counterparts [3]. They are frequently marginalised in urban communities and are targets of discrimination [2, 22].
The relationship between migration and mental health has been studied in a number of populations [1]. The overwhelming majority of studies are concerned with permanent inter-country migration [8, 20]. Many of these studies have concluded that migration and the related experiences of insecurity and loss of accustomed social networks are a major risk factor for psychological ill health [9, 19]. But other studies suggest that since migrants typically leave their homes to improve their economic status and increase their life opportunities, this may lead to improved psychological health [5, 14].
The literature about health consequences of migration in China has mainly focused on physical health status and in particular reproductive health [27–31, 33]. There is little focusing on the mental health consequences of migration. The present study aimed to explore the mental health status and help-seeking behaviours of rural-to-urban migrant workers in Hangzhou city, China, and to compare them with permanent urban and rural dwellers. It was part of a larger study, which investigated a range of health outcomes related to rural–urban migration.
Methods
This cross-sectional study was carried-out from June to December 2004 in Hangzhou, the provincial capital, and two rural townships in Zhejiang Province. Hangzhou has a population of 6.2 million with a migrant population of around 1.2 million, and is one of the boom cities of the East [32]. The study aimed to compare three population groups, rural-to-urban migrant workers, permanent urban residents, and permanent rural dwellers. Migrant workers were defined as individuals who hold a rural hukou, that is, with registered permanent residence in a rural area, and who have been living at the urban destination for at least 3 months. Permanent urban residents were those who possess an urban hukou and live and work in their permanently registered urban areas. In order to make these groups more comparable we limited the urban counterparts to those who were working in the same work units as migrant workers rather than sampling from the general population. Permanent rural residents were those holding a rural hukou and who live and work in their permanently registered villages.
The urban component of the study was carried-out in two of the eight districts of the city, randomly selected to represent suburban (Xiaoshan) and inner-city (Xihu). In each district a list of work units employing at least 30 workers and providing unskilled employment for both migrants and local people was drawn-up, giving 31 in Xiaoshan and 42 in Xihu. A sample of 50% of these workunits was selected to be representative of the major occupations of migrant workers in the formal sector in Hangzhou: construction companies, factories, restaurants, shops and hotels. For example, in Xihu 16 of 28 work units were involved in manufacturing, so the first eight factories on the list drawn-up were approached. In total 16 work units in Xiaoshan and 21 in Xihu were asked to participate and none refused. In each work unit all workers (migrant and urban) present on the day were invited to participate in the study.
Rural sampling took place after the migrant data were obtained, since the aim was to include areas from which a large number of the migrants originated. Migrants originated from 27 of the 33 Chinese provinces By far the largest single group (21%) were from Western Zhejiang, so this area was selected to provide the rural sample. Two of the 12 counties in Western Zhejiang were randomly selected and three villages in each of the counties were in turn randomly selected. Households were then randomly sampled from lists held by village authorities to achieve a sample size of approximately 300 respondents per village or a total of 1800. Working adults aged 15–54 (to match the age range in the migrant and urban samples) resident in the selected households on the day of the survey were included.
The questionnaire was developed specifically for this study. It included basic sociodemographic information and questions about living and working conditions and self-reported general health. The mental health component was divided into three parts:
-
(1)
Mental health status, measured by the 5-item Mental Health Scale from the Chinese SF-36 Health Survey which has been validated in Chinese populations [16, 17]. The five questions ask about mental well being in the last month on a 6-point Likert scale ranging from never to all the time. The SF-36 Mental Health Scale is recognised as a useful tool for monitoring population mental health, estimating burden of disease, monitoring outcomes in clinical practice and evaluating treatment effects [26].
-
(2)
Two questions about suicide ideation and suicide attempts: “Have you ever felt so low that you have thought of taking your own life?” and “Have you ever attempted to take your own life?” These questions were included because of the particular concerns about the high prevalence and distinctive socio-demographic characteristics of suicide in China [13].
-
(3)
Help-seeking behaviours for mental health problems: “At times when you have felt low, depressed or anxious have you felt you needed help from someone?” and for those who said they needed help “Who did you get help from” as an open question.
The questionnaire was piloted among a sample of 50 respondents and was modified and finalised according to the feedback. Prior to the study posters were used in all work units and in villages to publicise the project. Verbal consent was obtained from each respondent. The right to refuse participation was guaranteed. Anonymity and confidentiality were assured. Questionnaires were completed in the respective workunits in Hangzhou and in respondents’ homes in the villages. In both settings questionnaires were completed in the same way, self-administered without conferring with colleagues or family members. But research assistants were on-hand to help with any queries. All respondents were given the phone number of a professional counselor (placed at the end of the questionnaire) and they were advised that they could discuss any issues arising from the questionnaire in confidence with the counselor if they wished. In fact no-one took-up this offer.
Approvals for the study were obtained from the Ethics Committee of the Institute of Child Health, University College London and Zhejiang Bureau of Public Health.
Analysis
Data analysis was performed using SPSS for Windows Version 13.0. The SF-36 Mental Health scale scores were calculated according to the established scoring algorithms with higher scores indicating better health status. Sociodemographic variables were dichotomized for analysis purposes as shown in the tables. Pearson’s χ2 was used to evaluate the association between median SF-36 scores, suicide ideation, suicide attempts and help-seeking and key sociodemographic variables. Multivariate analysis was then used to compare these parameters between the migrants, urban and rural residents, while controlling for potential confounders. We further explored potential determinants of low mental health status in migrant workers because they were the main focus of interest. We divided the migrants into quartiles by their mental health scores on the SF-36 and compared top and bottom quartiles using initial Pearson χ2 tests followed by logistic regression to control for gender and age.
Results
Socio-demographic characteristics (Table 1)
A total of 4466 migrant workers, 2081 urban residents, and 1915 rural dwellers participated in the study, of which 4453 (99.7%), 1957 (94.0%), and 1909 (99.6%) in each group respectively were eligible for analysis. Migrant workers were the youngest of the three groups with rural workers the oldest (P < 0.0001). As expected urban workers had the highest levels of education, migrants second, with rural residents the least well educated (P < 0.0001). Half of the migrants (50%) worked in the manufacturing sector with 29% in the service sector (shops, hotels and restaurants) and 27% of the men in construction. The major incentive for migration was financial (81%), but 19% also cited acquiring new skills and 8% the attraction of an urban lifestyle. The median length of time since first migration was 2.7 years (range 3 months–10 years) and the median number of migrant labour jobs done was three with a range of 1–15. Fifty-one percent had migrated with a partner.
Working/living conditions (Table 1)
Migrants worked long hours, 28% over 12 h per day, and 81% 6 or 7 days per week, compared with 9.3% and 52% for urban workers respectively. The income of migrant workers was over twice that of rural workers, but less than urban workers. Sixty-three percent of the migrants said they were satisfied or very satisfied with their salary and 75% said they were able to save money. Only 19% of the migrants had any kind of health insurance compared with 68% of the urban workers and 9% of the rural residents, though levels of re-imbursement of medical expenditure varied widely from just 10% to 90%. Twenty-six percent of migrants, compared with 66% of urban workers, were entitled to sickpay, though in most cases (85%) this was not full salary equivalent. Delays and apparently arbitrary reductions in salary payments were described by 61% of migrants, but by only 23% of urban workers. Most (74%) of the migrants said they had excellent or very good relationships with their workmates with only 3% saying relationships were poor. Living conditions of migrants were very basic for the majority, most (64%) living in dormitory-style accommodation, provided by the work unit, sharing with several other workers and with outside amenities (tap water and toilets). However, nearly three-quarters (72%) of those living in this type of accommodation were satisfied or very satisfied with these conditions. The self-reported general health status of migrants was better than their urban and rural controls: 30% of migrant workers reported their health to be excellent or very good, in comparison with 13% of urban residents and 21% of rural residents, respectively (P < 0.001).
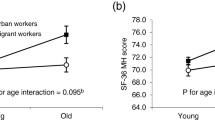
Mental health
On the SF-36 mental health scale migrants scored higher (mentally more healthy) than their urban counterparts, median 52.4 vs. 47.2 (P = 0.003), but lower than their rural counterparts, 52.4 vs. 60.4 (P < 0.0001). (Table 2) Male gender, older age (over 30), being married and higher income were all independently associated with better mental health status. After adjustment for age, gender, marital status and income, differences between migrants and urban workers for median MH SF-36 scales ceased to be significant (P = 0.08) while the comparison with rural workers remained significant P = 0.0005. There were small but significant differences in levels of suicide ideation and suicide attempts between the three groups with contemplation of suicide commonest in migrants and actual suicide attempts most common in the rural population (Table 3). However, the differences ceased to be significant after controlling for gender, age and marital status.
Migrants were most likely to say they needed help when anxious or depressed, but differences between the groups disappeared after controlling for gender, age and marital status (Table 3). However, migrants were least likely to have actually sought help when they needed it, 39% compared with 67% of urbanites and 86% of rural residents, with highly significant differences persisting after adjustment. In all three groups family and friends were the predominant help providers (Table 4). Rural dwellers mostly turned to family members, while migrants, far from family support, were more inclined to turn to friends. In <1% of cases professional help had been sought.
Separate analysis for migrants showed that being married, having migrated with a partner, a higher salary, good self-reported health and good living conditions were all associated with a higher mental health score on the SF-36 after adjustment for age and gender. (Table 5) The strongest associations were with good self-reported health (OR 3.1 95% CI 2.4–3.8), migration with a partner (OR 2.15, 95% CI 1.85–2.46) and higher salary (OR 1.75 95% CI 1.64–1.86).
Discussion
This study has a number of limitations. First, the study sampled work units in the formal sector and did not include the self-employed, such as hawkers and street-traders, who may have poorer mental health status. But it is estimated that these account for less than 3% of the total migrant population of Hangzhou, [32] so our sample is representative of the overwhelming majority. Second, the validity of self-report may be questionable, especially when exploring sensitive issues. There may be a tendency to answer questions more according to social norms than actual situations, a phenomenon known as social desirability [24]. There may also be a simple reluctance to admit to psychological difficulties even in an anonymous confidential questionnaire. However, the SF-36 has been validated for this population [17], and at the very least there is no reason to assume that any of the three population groups would be more likely than any other to misreport, so the comparisons are probably valid. In addition, in this study respondents were encouraged to use the don’t know option if they were not sure of their feelings, in an attempt to reduce this bias. It is also possible that the different situations in which the questionnaires were completed, work units in the urban area and home in the rural area, could present a source of bias, though in both situations privacy and anonymity were ensured, and research assistants were on hand to deal with any issues which arose. Finally, the study was carried-out in low income working individuals in a rich eastern coastal province. While some inferences can be drawn from this sample to individuals of similar socioeconomic status in other coastal provinces, our sample does not try to be representative of other parts of China, especially the poor inland and Western provinces.
Despite these limitations the study does contribute to our understanding of the mental health status of Chinese rural–urban migrant workers.
First, migrants did not have the worst mental health, as had been expected. After adjusting for confounders, they had slightly better mental health than urbanites but still had worse mental health than rural dwellers. There are a number of possible explanations for these observations. Although migrants have moved away from accustomed social networks, and experience long working hours, insecure employment and overcrowded, insalubrious living conditions (making them more vulnerable to mental ill-health than permanent rural dwellers), they have also taken the step to improve their economic situation with potential enhancement of psychological well-being [23]. Krahl et al. [14] in Malaysia and Coutinho et al. [5] in Brazil concluded that migration to a new environment with better economic opportunities impacts positively on psychological well being. In contrast, low paid urban dwellers may feel a grievance about their low income compared with other urban dwellers; with urban consumerism having risen dramatically over the past two decades alongside a huge increase in available consumer goods for those who can afford them, this has resulted in frustrated aspirations and envy for many of those who cannot [23]. In 2004 the average urban monthly income in Hangzhou was 1350 RMB [32], so the mean income in our urban sample was well below the average wage, perhaps contributing to a low sense of mental well-being compared with rural dwellers. The stress of contemporary urban life in China was highlighted by a survey among 3760 permanent urban dwellers from four cities (Hangzhou, Guangzhou, Chongqing and Taiyuan). This showed that 64% of respondents felt what was described as “middle level” stress, and 22% suffered from “frank” mental disorders, defined as meeting diagnostic criteria for a range of types of mental illness [29]. Rural dwellers on the other hand are surrounded by similar low income individuals and have less access to consumer goods. It has been suggested that rural poverty, because it is less inequitable, therefore impacts less on their psychological well being [23].
Second, this population of migrants has moved within a country and a culture, and because of the system of hukou, they are not classed as permanent residents. Many will eventually return to their rural area of origin. Much of the research focusing on the psychological vulnerability of migrants relates to migrants crossing borders and migrating on a permanent basis [1, 20]. Moving to a different country with unfamiliar culture and language, has been shown to lead to anxiety, depression and stress, and in extreme cases, physical illness and suicide among migrants [11, 25]. This is clearly a very different situation to that experienced by these Chinese internal migrants and this is reflected in their relatively good mental health status.
The third possible reason for the good mental health status of the migrants in our study relates to social capital. Social capital has a structural component and a cognitive component. The structural aspect of social capital (connectedness, membership of organisations, or in the Chinese context work units), may reduce the negative impacts of a life event such as migration, by providing additional support. The cognitive aspects of social capital, such as trust, sense of belonging, and shared values, may increase feelings of security and self-esteem and consequently improve mental health [7]. That a lack of social capital could lead to mental health problems has been supported by much evidence [6, 10]. The importance of social capital to mental well being is well shown in our study. Migrating with a partner and having very good relations with colleagues were strong predictors of higher mental health scores. It is also well known in China that migrants frequently migrate in groups from the same rural area to a single work unit, leading to increased camaraderie and mutual support [10].
Previous work has shown an association between migration and suicide [15, 25]. It is therefore of note that we found only small differences between suicidal thoughts and suicide attempts in the three groups, supporting the view that these migrants are not more vulnerable to these extremes than rural or urban counterparts. The higher level of suicide attempts in rural areas is in line with previous findings of high attempted suicide and particularly completed suicide in rural China [4].
Help-seeking behaviour showed interesting patterns. Migrants felt they needed help when they were depressed or anxious more than either urban or rural counterparts. However, they were least likely to actually take action to get help. This maybe because they are separated from their accustomed support network which, in rural China consists largely of family. But across all three groups family and friends were by far the major sources of support with only a tiny minority having resorted to professionals. This is perhaps not a surprising finding given that professional counseling and psychological support services remain very limited even in urban China [28] and what is available is costly, and certainly beyond the reach of the populations in this study. It also remains traditional, even in urban China, to seek help from informal sources, even in extreme situations [12]. It is noteworthy that no-one took-up the offer of free counseling following the completion of the questionnaire. This could be partly because the respondents are unaccustomed to such a free offer (and maybe suspicious of it) or it may relate to the considerable stigma, which is still attached to help seeking for mental health disorders. Given the number of individuals across all three groups who had contemplated and actually tried to commit suicide, this is a serious concern. There is clear unmet need here and professional help should be more readily accessible and affordable to migrants, urban dwellers and rural dwellers alike.
References
Bhugra D (2004) Migration and mental health. Acta Psychiatr Scand 109:243–258
Cai F, Wang D (2003) Migration as marketisation: what can we learn from China’s 2000 census data? The China Rev 3(2):73–93
Chan KW, Zhang L (1998) The hukou system and rural-urban migration in China: processes and changes. Centre for Studies in Demography and Ecology Working Paper, University of Washington
Conner KR, Phillips MR, Meldrum SC (2007) Predictors of low-intent and high-intent suicide attempts in rural China. Am J Public Health 97(5):1–5
Coutinho Eda S, de Almeida Filho N, Mari J, et al. (1996) Minor psychiatric morbidity and internal migration in Brazil. Soc Psychiatry Psychiatr Epidemiol 31:173–179
De Silva MJ, Huttly S, Harpham T, Kenward MG (2007) Social capital and mental health: a comparative analysis of four low income countries. Soc Sci Med 64:5–20
De Silva MJ, McKenzie K, Harpham T, Huttly S (2005) Social capital and mental illness: a systematic review. J Epidemiol Community Health 59:619–627
Escobar JL, Hoyos Nervi C, Gara MA (2000) Immigration and mental health: Mexican Americans in the United States. Harv Rev Psychiatry 8(2):64–72
Fox PG, Burns KR, Popovich JM, et al. (2001) Depression among immigrant Mexican women and Southeast Asian refugee women in the U.S. Int J Psychiatr Nurs Res 7:778–792
Guan XP, Jiang MY (2002) Basic life and health services for migrants in cities. In Peilin L (ed) Peasant workers: economic and social analysis of peasant workers in the city. Social Sciences Documentation Publishing House, Beijing
Hovey JD, Magana CG (2002) Exploring the mental health of Mexican migrant farm workers in the Midwest: psychosocial predictors of psychological distress and suggestions for prevention and treatment. J Psychol 136:493–513
Hu JN, Higgins J, Higgins LT (2006) Development and limits to development of mental health services in China. Crim Behav Mental Health 16(2):69–76
Ji J, Kleinmann A, Becker AE (2001) Suicide in contemporary China: a review of China’s distinctive suicide demographics in their sociocultural context. Harv Rev Psychiatry 9(1):1–12
Krahl W, Hashim A (1998) Psychiatric disorders in ASEAN-migrants in Malaysia-a university hospital experience. Med J Malaysia 53:232–238; 31. Kwan
Kwan YK, Ip WC (2007) Suicidality and migration among adolescents in Hong Kong. Death Stud 31(1):45–66
Lam C, Tse E, Gandek B, Fong D (2005) The SF-36 summary scales were valid, reliable and equivalent in a Chinese population. J Clin Epidemiol 58:815–822; 21
Li L, Wang HM, Shen Y (2003) Chinese SF-36 health survey: translation, cultural adaptation, validation, and normalization. J Epidemiol Community Health 57:259–263
National Bureau of Statistics of China (NBSC) (2002) Statistics of the Fifth National Census in 2000. Available at http://www.china.org.cn Accessed September 1, 2006
Noh S, Avison WR (1992) Assessing psychopathology in Korean immigrants: some preliminary results on the SCL-90. Can J Psychiatry 37:640–645
Pumariega AJ, Rothe E, Pumariega JB (2005) Mental health of immigrants and refugees. Community Ment Health J 41(5):581–597
Saywell T (2000) Hit the high road. Far East Econ Rev May, 35–39
Seeborg MC, Jin Z, Zhu Y (2000) The new rural-to-urban mobility in China: causes and implications. J Socio Econ 29:39–46
Shen YC (1996) Mental health challenges in China in the twenty-first century. Chinese J Psychiatry 29:5–6
Sjostrom O, Holst D (2002) Validity of a questionnaire survey: response patterns in different subgroups and the effect of social desirability. Acta Odontol Scand 60:136–140
Stack S (1980) The effects of interstate migration on suicide. Int J Soc Psychiatry 26:17–26
Ware JE, Snow KK, Kosinski M (1993) SF-36 health survey: manual and interpretation guide. The Health Institute, New England Medical Centre, Boston Massachusetts
Wu JL, Bao YQ (1999) Beijing migrants reproductive health. Chinese MCH J 14(4):234–236
Yan HQ (1998) New challenges of psychiatry: the development of mental health service in Shanghai. Psychiatry Clin Neurosci 52:S357–S358
Yang TZ, Liu XL (2003) Public health issues on psychological stress and preventive countermeasures. Chinese J Prev Med 37:207–209
Ye XJ, She WX, Li L (2004) Health status of migrant workers in cities and policy suggestions. Chin J Hosp Admin 20:562–566
Ye LM, Wang JJ, Mei LY (2004) Health maintenance and countermeasures for rural migrant workers. J Pub Health Prev Med 15:75–76
Zhejiang Provincial Statistics Bureau (2005) Zhejiang statistical year book 2004. Zhejiang People’s Publisher, Hangzhou
Zheng Z, Zhou Y, Zheng L, Yang Y, Zhao D, Lou C, Zhao S (2001) Sexual behaviour and contraceptive use among unmarried young women migrant workers in five cities in China. Reprod Health Matters 9(17):118–127
Acknowledgements
The study was funded through a Wellcome Trust project grant No 069355
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Li, L., Wang, Hm., Ye, Xj. et al. The mental health status of Chinese rural–urban migrant workers. Soc Psychiat Epidemiol 42, 716–722 (2007). https://doi.org/10.1007/s00127-007-0221-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-007-0221-0