
Abstract
Background
Illness perception, a measure of illness representations developed from physical medicine, has recently been applied to psychosis. We investigated how illness perceptions relate to affect and expressed emotion (EE) in carer-patient dyads, particularly if their perceptions differed.
Method
We interviewed 82 carer-patient dyads, after a relapse of psychosis. Carers were assessed for illness perceptions, distress, self-esteem and EE; patients for illness perceptions, depression, anxiety and self-esteem, in a cross sectional study.
Results
Carers were more pessimistic than patients about illness persistence and consequences, and carers with low mood were particularly pessimistic about persistence and controllability. Discrepant views about illness consequences were related to greater anxiety, depression, and lower self-esteem in patients, while discrepant views on controllability were associated with greater distress, depression, and lower self-esteem in carers. Illness perceptions did not relate directly to EE.
Conclusions
In this sample, meta-cognitive carer representations of illness in psychosis are related to negative affective reactions in carers, but not to EE. Resolving discrepant illness perceptions between carers and patients might provide a way of improving family reactions to the health threat of psychosis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Caring for people with psychosis has been associated with subjective burden and loss, depression, distress, reduced quality of life, lower social support and stigma [20, 34, 36, 41, 42]. One way of understanding this impact of care has been through carers’ appraisals of the difficulties, as it has been shown that their reactions to their role can be as important as the problems they encounter [2, 17, 40].
There have been various approaches to this. One method involves rating comments, or expressed emotion (EE), during an interview, using prosodic variables such as tone and pitch as well as content. EE has been found to be a robust predictor of poor outcome in both schizophrenia and other physical and mental health conditions [9, 16, 46]. Another approach is the study of carer attributions, which also relate to EE [7, 14]. For instance, highly critical relatives are particularly likely to attribute to patients more control over their symptoms and problems, and to hold them responsible for their difficulties [7].
In health psychology, one conception of illness appraisal has been based on the self-regulatory model of Leventhal and colleagues [29]. These authors have proposed that when individuals are faced with a health threat, they formulate a cognitive representation of their illness in terms of five core constructs. These comprise identity (the symptoms and name of the illness), cause (the aetiology), cure/control (the extent to which the illness is modifiable or curable), consequences (the personal, social and financial effects of the illness) and timeline (the perceived length of time the illness will continue). These are held to predict both practical and emotional responses to a health threat, such as the amount of distress, or whether a person will seek or accept treatment. These illness perceptions have been investigated in physical health conditions, where they do indeed predict a range of outcomes including well-being [23].
In health psychology, there has also been interest in discrepancies in illness perceptions between patients and their carers. Heijmans et al. [24], in an elegant study, found that carers of those with Addison’s disease (AD) tended to have more concerns than patients (maximizers), whereas carers of those with Chronic Fatigue Syndrome (CFS) tended to minimise concerns. Thompson et al. [43], found that if carers were overprotective with stroke patients, the patients became more dependent. Weinman et al. [48], found that carer minimisation of difficulties predicted poor patient outcomes, and suggested that in psychiatric illness this might indicate that problems were not being taken seriously. For people with psoriasis, Richards et al. [38] found that dissimilar beliefs about illness consequences related to worry in carers.
The self-regulatory model and the measurement of illness perceptions have recently been extended to those with psychosis and their carers [22, 30, 31]. Barrowclough et al. [5] showed that more critical relatives perceived themselves to have less control over the illness, thought it would last longer, and perceived a greater number of symptoms. Lobban et al. [32] found that where participant-relative dyads diverged in their illness perceptions, the carers were more likely to be high EE and to maximise negative outcomes compared to patients.
Given this background and the paucity of studies in psychosis so far, we aimed to investigate the relationships in carer–patient dyads between illness perceptions, affect and carer EE, following a recent relapse of psychosis. We also wished to look at the effects of discrepant illness perceptions on both carer and patient affect.
We tested the following hypotheses:
-
High EE in carers (criticism and over-involvement) would be related to pessimistic illness perceptions of psychosis, specifically perceptions of the consequences, how long it would last (timeline) and whether anything could be done to improve things (cure/control), for both patients and carers.
-
Negative illness perceptions would be related to disturbed affect in carers (distress, depression and low self-esteem)
-
In order to replicate Lobban et al. [32] we predicted that discrepant illness perceptions between carers and participants would relate to high EE ratings. Further we predicted that such discrepancies would also relate to disturbed affect (stress/anxiety, depression and low self-esteem) in both carers and patients.
-
Finally, we hypothesised that carers and patients would have discrepant illness perceptions (carers would be maximisers) in high EE dyads and concordant illness perceptions in low EE dyads.
Method
Participants
The study sample consisted of patients recruited for the Psychological Prevention of Relapse in Psychosis (PRP) Trial (ISRCTN83557988) and their immediate carers. PRP is a UK multi-centre randomised controlled trial of cognitive behaviour therapy and family intervention for psychosis, designed to test hypotheses both about outcome and about the psychological processes associated with psychosis for carers and patients.
The trial was located in four NHS Trusts in London and East Anglia, in the UK. Within each of these Trusts, recruitment was from specified inpatient and outpatient teams that agreed that all patients meeting the eligibility criteria would be asked to participate in the trial. These services were canvassed at least fortnightly for patients with psychosis who were relapsing. Patients meeting the inclusion criteria for the study, (see below), were asked to provide informed consent. If they had carers, they were included if they were the carer in most contact with the patient (i.e., for at least 10 h a week, including telephone calls), had been in a caring role with the patient for at least the previous 3 m, and had a command of the English language sufficient for interview and potential participation in psychological therapies. Consent was then sought from the patient for their carers to enter the trial. Carers were not approached unless this consent had been obtained. Only the primary carer was sought for each patient, and if consent was refused, no other carer from that family was approached.
Patients were recruited at the time of a re-emergence of positive symptoms, either from a previously recovered state or from a state of persisting symptoms. For people with persistent symptoms, a significant exacerbation in positive symptoms was required, typically leading to hospital admission. Patient inclusion criteria were: current clinical diagnosis of non-affective psychosis (schizophrenia, schizo-affective psychosis, delusional disorder; ICD-10, F20); age 18–65 years; a second or subsequent episode starting not more than three months before patients consented to enter the trial; and a rating of least four (moderate severity) on at least one positive psychotic symptom of the Positive and Negative Syndrome Scale (PANSS; Kay et al. [26]) at the first time of meeting.
Eighty-two patients and their carers who had consented to take part in the PRP trial and completed a majority of the assessments were included in this study.
The study design was cross-sectional. The data were all obtained by trained independent research assessors, who interviewed identified patients and then their carers, and administered questionnaires during the baseline phase of the randomised controlled trial and before allocation.
Carers were recruited consecutively. 208 patients who met criteria were in contact with carers but 114 refused access to them (54%). Our ethics committee required that carers did not have to give a reason for this refusal, information that is thus unavailable. This was about the same refusal rate for patient participation in PRP overall (55%). A further 11/94 carers themselves refused consent (12%). Again, no details were available for the group that refused consent. One further carer did not provide full data on the IPQ ratings.
The study had ethical approval; reference MREC 01/1/14.
Carer measures
Illness Perceptions Questionnaire (IPQ) [47]
The IPQ consists of items measuring 5 core illness constructs: identity, cause, consequences, cure/control, timeline. The IPQ is a reliable and valid measure of illness perceptions in psychosis [30]. We used a version of the original IPQ modified by Weinman and Garety for use in people with psychosis [25], with the words problem/illness used instead of just illness. The constructs used in this study were consequences, timeline and cure/control, comprising seven, three and six items respectively in accordance with Weinman’s [47] original IPQ. Items were measured on a scale of 1–5, ranging from strongly disagree to strongly agree. Carers were asked to rate how they thought the illness had affected the participant.
When carer and participant IPQ’s were compared directly, the items in each component were matched to ensure that we were looking at identical scales; for these comparisons, we used 6 items for consequences, five for cure/control and 2 timeline items. Internal reliability values for these identical modified scales were satisfactory, although those for consequences were lower (carer perception of patient consequences, Cronbach α = 0.55; patient perception of consequences α = 0.53; carer cure/control α = 0.77; patient cure/control α = 0.67; carer chronic timeline items α = 0.74; patient chronic timeline α = 0.92 [45]).
In order to assess discrepancies between patient and carer scores, we looked directly at the scores for each dyad, and subtracted patient from carer scores. This meant that positive scores indicated that carers were more pessimistic than patients (maximisers). Cure/control was reversed scored for consistency. In order to see if it was the size of the discrepancy rather than the direction that was indicative, we then modified the discrepancy score by removing the sign, to obtain a total discrepancy score.
Camberwell Family Interview (CFI) [44]
The CFI is a semi-structured interview during which carers are asked how they get on with the person who has had a recent episode of psychosis. It covers family relationships, arguments, time spent together, symptoms, and role functioning. With consent this interview was audiotaped, and subsequently rated for EE, by trained research assessors. Five scales are rated, critical comments (CC, frequency count), hostility (0, 1, 2 or 3), warmth (0–5), emotional over involvement (EOI) (0-5) and positive remarks (frequency count). More than 6 CCs, any hostility, or a rating of 3 or above on EOI categorise a carer as high EE. The interviews were taped recorded, and rated by assessors who had been trained by Dr Christine Vaughn After training, all assessors had obtained high correlations or phi coefficients on all EE scales: >0.76 for CC, hostility, EOI, warmth, positive remarks and overall EE category. In the current study we focussed on CC, EOI and overall EE.
Rosenberg Self-esteem scale [39]
This measure consists of 10 items, each measured on a four-point scale, from strongly agree to strongly disagree. After reverse scoring, the items were totalled and divided by 10 to produce an overall self-esteem score, where a high score represents low self-esteem.
The General Health Questionnaire (GHQ) [22]
The 28-item version was used, with scoring of 0,1,2,3... It has a total score and four subscales of somatic symptoms, stress, social functioning, and depression. In the current paper we focus on the stress and depression subscales.
Participant measures
Illness Perceptions Questionnaire [47] (see above).
Rosenberg Self-esteem scale (see above) [39].
Beck Depression Inventory-II (BDI-II) [11]
This established measure consists of 21 items, each measured on a scale of 0–3. The total BDI-II score thus ranges from 0 to 63, with a high score representing more symptoms. Depression is measured for the previous two weeks. Birchwood et al. [13], have reported a high correlation (r = 0.91) between the BDI and the interview based Calgary Depression Scale for Schizophrenia [1], confirming that the BDI can be used for assessing depression in psychosis.
Beck Anxiety Inventory [10]
This measure consists of 21 items, each measuring common anxiety symptoms. The total anxiety score ranges from 0 to 63, with a higher score representing greater anxiety. Anxiety is measured in relation to the previous week.
Statistical analysis
Analyses were conducted using SPSS for Windows (version 12.01). Using analysis of variance we initially looked at the relationships between high EE and carer and participant consequences, timeline and perceptions of cure/control. We repeated this for criticism and for EOI, the latter having been dichotomised: ≥3 indicated high EOI. We used Spearman’s correlations to test relationships between effects on carers using the stress (B) and depression (D) subscales of the GHQ and the Rosenberg self-esteem score (SE). Differences in patient and carer illness perceptions were investigated for their relationships with EE in cross tabulations, with post hoc tests of significance. Finally carer and patient affect were correlated with IPQ discrepancy ratings.
Results
The sample consisted of 82 carer/participant dyads. Analyses were done on those with a full data set for the specific comparisons (N = 66–82). Demographic details for patients and carers are given in Table 1. Patients were mainly male (72%), unemployed (79%), white (83%), and single (63%). They had a mean age of 36.2 years, and an average 11.2 years of illness before the most recent episode. Sixty nine percent had a diagnosis of schizophrenia and 13% a diagnosis of schizoaffective disorder. The mean total PANNS score for the patient group was 67.3 (SD = 14.4). On the BDI II the mean score for patients was 24.9 (SD = 13.2), and of 20.5 on the BAI (SD = 14.7). On the Rosenberg, patients had a mean score of 2.46 (SD = 0.65).
Carers had an average age of 52.4 years, and were mainly female (69%). Half were parents, and 40% were employed. Aspects of their contact time and ratings on EE are provided in Table 2. There was some expected overlap between high criticism and high EOI, in that 10 carers had both. Hostility coincided with criticism apart from one carer, and was not therefore considered separately in any of the following analyses. Carers were predominantly low EE (N = 53, 65%), and revealed relatively low levels of criticism (mean = 3.2). There was no relationship between EE and any demographic variable.
First, high and low EE dyads were examined in relation to the carer and patient-rated IPQ constructs of consequences, timeline and cure/control. All IPQ variables were rated in two ways, based respectively on the carers’ views and the patients’ views of the implications of the illness for the patient. Contrary to prediction, there were no significant relationships between EE and IPQ variables. When EOI was examined separately using analysis of variance, there was a single significant difference: patients in high EOI dyads rated the consequences of their illness less seriously (mean = 3.43, SD = 0.7) than those in low EOI dyads (mean = 3.84, SD = 0.57) (F = 6.14, P = 0.02). There were no significant relationships between criticism and any patient or carer IPQ variables.
Next we looked at whether carer IPQ variables were related to carer affect (Table 3). There were four significant correlations; carers who rated patients as having little cure or control had significantly greater stress (spearman’s rho = −0.25 P = 0.03), greater depression (rho = −0.26, P = 0.02) and poorer self-esteem (rho = −0.41, P = <0.001); carers who thought that the illness had a long timeline also had significantly higher stress (rho = 0.22, P = 0.05).
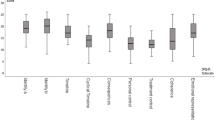
Discrepant scores on consequences and control were correlated (rho = 0.38, P < 0.001) as were consequences and timeline (rho = 0.43, P < 0.001). Carers emerged as significantly more pessimistic than patients about both consequences (carer mean = 4.02 (SD = 0.56), patient mean = 3.75 (SD = 0.62), paired t = 2.91, P < 0.005) and timeline (mean for carers = 3.86 (SD = 0.83), mean for patients = 3.47 (SD = 1.25), paired t = 2.86, P = 0.006), but not for cure/control (mean for carers = 3.56 (SD = 0.73), mean for patients = 3.43 (SD = 0.77), paired t = 1.15, ns). In other words carers generally tended to regard problems more seriously than patients.
We examined whether high EE dyads revealed more discrepant scores than low EE dyads, using analysis of variance. However no significant differences emerged. We then correlated IPQ differences with carer and patient affect. We found that when carers were more optimistic than patients about consequences, this seemed to relate to greater patient anxiety (rho = 0.35, P = 0.003), more depression (rho = 0.398, P < 0.001), and poorer self-esteem (rho = 0.38, P = 0.001). Carer optimism about illness persistence was also correlated with patient anxiety (rho = 0.26, P = 0.026). When carers were more pessimistic about future control of the illness, patients had relatively good self-esteem (rho = 0.29, P = 0.016), but carers experienced greater stress (rho = 0.39, P = 0.001) and depression (rho = 0.28, P = 0.019), and lower self-esteem (rho = 0.40, P = 0.001). Finally, irrespective of direction, the magnitude of divergent views between carers and patients about illness consequences related to carer emotional over-involvement, a component of EE (rho = 0.26, P = 0.022). This relationship remained significant (rho = 0.23, P = 0.045) when criticism was controlled for.
Discussion
We were not able to confirm previous findings [5, 32] that high EE related directly to negative illness perceptions in carers, nor that high EE dyads had more discrepant illness representations. This may have been because our EE ratings were lower than in other samples, so that we had a majority of carers in the low EE category. Our sample was thus unusual compared to previous literature. This may have been due to our low consent rates, as high EE dyads may have opted out of the study, but we were unable to check this. It may also have been the result of the rural residence of many of the participants. It was unlikely to have been due to errors in rating, as we used the Camberwell Family Interview, the ‘gold standard’ for measuring EE, and our EE ratings were trained to criteria. While the lower levels of criticism might have led to some lack of power, our high EE sample was still larger than those of previous studies in the area, but our results may not be generalisable.
What we did find was that negative carer illness representations were related to carer affect. Carer distress, depression, and low self-esteem was also associated with the thought there was little participants could do to control their symptoms. Moreover, carers who were more stressed were also more pessimistic about the persistence of illness. Barrowclough et al. [5] found relationships between carer depression, burden and negative consequences on the IPQ, but only high EE in carers was related to negative perceptions of cure control. Fortune et al. [21] found greater distress in carers who perceived negative illness consequences and felt strongly that patients could control their illness.
Lobban et al. [32] did not show relationships between overall EE and carer illness perceptions either, but did show that high EE carers (N = 14) were more likely to be maximisers of illness perceptions, compared to low EE carers (N = 35). We found that all carers tended to have more pessimistic illness perceptions than patients, and this was not related to EE. Instead we found that patients in high emotional over-involvement dyads (a component of high EE) rated illness consequences more optimistically. However, we do not know the direction of this relationship. Either patients in these dyads tended to minimise or perhaps deny any consequences for themselves, or patients who felt that there were fewer consequences had more over-involved carers.
We have previously shown that patients with high EE carers have significantly more anxiety and depression, but not more symptoms of psychosis [28]. Barrowclough et al. [6] demonstrated that critical evaluation by family members was associated with negative evaluation of self in patients. Lysaker et al. [33] recently found poor coping with stress in people with schizophrenia was related to their anxiety. Bentsen et al. [12] had previously shown that carer over-involvement related to greater patient anxiety and depression. In the current study we were able to show that disagreement about consequences and the amount of patient control in psychosis was associated with disturbed affect in patients as well as in carers, although the direction of causality is not clear. However, it is consistent with evidence from physical health that negative illness perceptions can relate to poor outcomes [23]. Divergent views, particularly minimisation, appear to be one response to serious ill health in carer-patient dyads [24]. We have shown that such disagreement can also be relevant to psychosis.
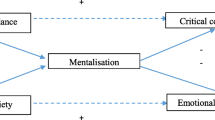
The results are of theoretical interest, in that they suggest that the meta-cognitive representation of illness has relevance for our understanding of psychosis in the same way that it has for other health conditions. Neither these representations nor discrepant views related directly to measures of EE as we had predicted. However, discrepant views did relate to negative affect in both patients and carers, and negative affect has been found to relate to EE in other studies. Discrepant illness representations may be a more direct way of understanding how patients and their families feel about, and try to cope with, the health threat posed by psychosis, and how they go on to make decisions about actions they will take as a result.
Limitations
This study has several limitations. First, it was a cross sectional study, and we were not able to infer causality or look at illness perceptions over time. Secondly, we did not compare participant IPQ ratings with symptoms. We have investigated this in another study [22], in which we found that, as we predicted, patients distressed about their symptoms had more negative illness perceptions but not more symptoms of psychosis. Thirdly, our sample of carers and participants had relatively low EE and generally did not come from inner city locations, and this may limit the generalisability of the results. Fourthly, unlike Figueras and Weinman [19], we did not use medians to establish discrepant IPQ ratings, but used a straightforward difference score. This may have weakened the power of some of our analyses. Fifthly, many of our correlations, although significant, were modest. Our results thus need to be replicated.
Clinical applications
Family interventions in psychosis [3, 4, 8, 18, 27] have a relatively well-established evidence base [15, 35, 37]. However, if illness perceptions in families relate to mood, this provides a theoretical basis for specific interventions for those living with psychosis. One therapeutic pathway is to facilitate communication and negotiated problem solving. Encouraging both participants and carers to be realistic and respectful of each other’s perceptions, neither overly pessimistic nor dismissive, and able to listen to a contrary view, is part of more productive and solution focussed change. This study suggests that we can use illness perceptions to understand that when carers and patients have different views about the health threat of psychosis, this can impact on mood. This awareness could help therapists to focus on ways of resolving such discrepancies, and improving negative mood, for both carers and patients.
References
Addington D, Addington J, Maticka-Tyndale E (1993) Assessing depression in schizophrenia: the Calgary Depression Scale. Br J Psych 163(s22):39–44
Addington J, McCleery A, Addington D (2005) Three-year outcome of family work in an early psychosis program. Schizophrenia Res 79:107–116
Addington J, Burnett P (2004) Working with families in the early stages of psychosis. In: Gleeson JFM, McGorry PD (eds) Psychological interventions for early psychosis. Wiley and Sons, Chichester
Anderson C, Reiss D, Hogarty GE (1986) Schizophrenia in the family: a practical guide. Guilford Press, New York
Barrowclough C, Lobban F, Hatton C, Quinn J (2001) Investigation of models of illness in carers of schizophrenic patients using the Illness Perception Questionnaire. Br J Clin Psychol 40:371–385
Barrowclough C, Tarrier N, Humphreys L, Ward J, Gregg L (2003) Self-esteem in schizophrenia: Relationships between self-evaluation, family attitudes, and symptomatology. J Abnorm Psychol 112/1:92–99
Barrowclough C, Hooley JM (2003) Attributions and expressed emotion: a review. Clin Psychol Rev 23(6):849–880
Barrowclough C, Tarrier N (1992) Families of schizophrenic patients: cognitive behavioural intervention. Chapman & Hall, London
Bebbington P, Kuipers L (1994) The predictive utility of EE in schizophrenia: an aggregate analysis. Psychol Med 24:707–718
Beck AT, Epstein N, Brown G, Steer R (1988) An inventory for measuring clinical anxiety: psychometric properties. J Consulting Clin Psychol 56:893–897
Beck AT, Steer RA, Brown GK (1996) BDI-II Manual. The psychological corporation, San Antonia
Bentsen H, Boye B, Munkvoid OG, et al. (1996) Emotional overinvolvement in parents of patients with schizophrenia or related psychosis: demographic and clinical predictors. Br J Psych 169:622–630
Birchwood M, Iqbal Z, Chadwick P, Trower P (2000) Cognitive approach to depression and suicidal thinking in psychosis: I Ontogeny of post-psychotic depression. Br J Psych 177:516–528
Brewin CR, MacCarthy B, Duda K, Vaughn CE (1992) Attribution and expressed emotion in the relatives of patients with schizophrenia. J Abnorm Psychol 101(2):313
Bustillo JR, Lauriello J, Horan WP, Keith SJ (2001) The psychosocial treatment of schizophrenia: an update. Am J Psych 158:163–175
Butzlaff RL, Hooley JM (1998) Expressed emotion and psychiatric relapse: a meta-analysis. Arch General Psych 55:547–552
Cuijpers P, Stam H (2000) Burnout among relatives of psychiatric patients attending psychoeducational support groups. Psychiatric Services 51(3):375–379
Falloon IRH (1985) Family management of schizophrenia. John Hopkins University Press, Baltimore
Figueiras MJ, Weinman J (2003) Do similar patient and spouse perceptions of myocardial infarction predict recovery? Psychol Health 18(2):201–216
Foldemo A, Gullberg M, Ek AC, Bogren L (2005) Quality of life and burden in parents of outpatients with schizophrenia. Social Psych Psychiatric Epidemiol 40(2):133–138
Fortune DG, Smith JV, Garvey K (2005) Perceptions of psychosis, coping, appraisals, and psychological distress in the relatives of patients with schizophrenia: An exploration using self-regulation theory. Br J Clin Psychol 44:319–331
Goldberg DP, Williams P (1988) A user’s guide to the General Health Questionnaire. NFER Nelson, Windsor
Haggar M, Orbell S (2003) A meta-analytic review of the common-sense model of illness representations. Psychol Health 18(2):141–184
Heijmans M, de Ridder D, Bensing J (1999) Dissimilarity in patients, and spouses representations of chronic illness; exploration of relations to patient adaption. Psychol Health 14(3): 451–466
Jolley S, Garety PA (2004) Insight and delusions: a cognitive psychological approach. In: Amador X, David A (eds) Chapter in insight and psychosis, 2nd edn. OUP, Oxford
Kay SR (1991) Positive and negative syndromes in schizophrenia: assessment and research. Brunner/Mazel, New York, NY, USA
Kuipers E, Leff J, Lam D (2002) Family work for schizophrenia: a practical guide, 2nd edn. Gaskell Press, London
Kuipers E, Bebbington P, Dunn G, Fowler D, Freeman D, Watson P, Hardy A, Garety P (2006) The influence of carer expressed emotion and affect on relapse in non-affective psychosis. Br J Psych 188: 173–179
Leventhal H, Nerenz DR, Steele DF (1984) Illness representations and coping with health threats. In: Baum A, Singer J (eds) Handbook of psychology and health vol IV, Erlbaum, Hillsdale, NJ
Lobban F, Barrowclough C, Jones S (2003) A review of the role of illness models in severe mental illness. Clin Psychol Rev 23:171–196
Lobban F, Barrowclough C, Jones S (2004) The impact of beliefs about mental health problems and coping on outcome in schizophrenia. Psychol Med 37(7):1165–1174
Lobban F, Barrowclough C, Jones S (2006) Does expressed emotion need to be understood within a more systemic framework? An examination of discrepancies in appraisals between patients diagnosed with schizophrenia and their relatives. Social Psych Psychiatric Epidemiol 41: 50–55
Lysaker PH, Davis LW, Lightfoot J, Hunter N, Stasburger A (2005) in press. Association of neurocognition, anxiety, positive and negative symptoms with coping preference in schizophrenia spectrum disorders. Schizophrenia Research 80:163–171
Magliano L, Fiorillo A, De Rosa C, Maj M (2006) Family burden and social network in schizophrenia vs. physical diseases: preliminary results from an Italian national study. Acta Psychiatrica Scandinavica 113(Suppl 429):60–63
NICE (National Institute for Clinical Excellence) (2003) Schizophrenia; full National Clinical Guideline for schizophrenia. Gaskell Press
Patterson P, Birchwood M, Cochrane R (2005) Expressed emotion as an adaptation to loss. Prospective study in first-episode psychosis. Br J Psych 187(48):s59-s64
Pitschel-Walz G, Leucht S, Bauml J, Kissling W, Engel RR (2001) The effect of family interventions on relapse and rehospitalization in schizophrenia–a meta-analysis. Schizophrenia Bull 27(1):73–92
Richards HL, Fortune DG, Chong SLP, Mason DL, Sweeney SKT, Main CJ, Griffiths CEM, et al. (2004) Divergent beliefs about psoriasis are associated with increased psychological distress. J Investigative Dermatol 123:49-56
Rosenberg M (1965) Society and the adolescent self-image. Princeton University Press, Princeton
Scazufca M, Kuipers E (1996) Links between EE and burden of care in relatives of patients with schizophrenia. Br J Psych 168:580–587
Scazufca M, Kuipers E (1999) Coping strategies in relatives of people with schizophrenia before and after psychiatric admission. Br J Psych 174:154–158
Tennakoon L, Fannon D, Doku V, Santamaria M, O’Ceallaigh Kuipers E, Sharma T (2000) The experience of caregiving: relatives of first episode psychotic people. Br J Psych 117:529–533
Thompson SC, Pitts JS (1992) In sickness and in health: chronic illness, marriage, and spousal care-giving. In: Spacapan S, Oskamp S (eds) Helping and being helped: naturalistic studies. Sage publications, Newbury Park, pp 115–151
Vaughn CE, Leff J (1976) The influence of family and social factors on the course of psychiatric illness. Br J Psych 129:125–137
Watson P (2006) The role of illness perception in psychosis. Unpublished PhD thesis, University of London
Wearden AJ, Tarrier N, Barrowclough C (2000) A review of expressed emotion research in health care. Clin Psychol Rev 20(5):633–666
Weinman J, Petrie K, Moss-Morris R, Horne R (1996) The illness perception questionnaire: a new method for assessing the cognitive representation of illness. Psychol Health 11:431–445
Weinman J, Heijmans M, Figueiras M (2003) Carer perceptions in chronic illness. In: Cameron LD, Leventhal H (eds) The self-regulation of Health and Illness Behaviour. Harwood Academic Publishers, London
Acknowledgements
This study was supported by a Wellcome programme grant no: 06452.
We are grateful to all the participants and carers who consented to take part in the study, and to the clinical teams in the South London and Maudsley NHS Trust, Camden and Islington Mental Health and Social Care Trust, North East London Mental Health Trust and Norwich Mental Health Trust. We are also grateful to Louise Isham and Katherine Ruffell who helped with EE ratings.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kuipers, E., Watson, P., Onwumere, J. et al. Discrepant illness perceptions, affect and expressed emotion in people with psychosis and their carers. Soc Psychiat Epidemiol 42, 277–283 (2007). https://doi.org/10.1007/s00127-007-0165-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-007-0165-4