
Abstract
Background
Problems relating to alcohol use are very common among deliberate self-harm (DSH) patients, and alcohol abuse increases the risk of both DSH and suicide. In the UK, per capita consumption of alcohol has risen by 50% since 1970. The proportion of women (but not men) drinking in excess of government-recommended limits has also increased. We investigate trends, by gender and age group, in alcohol problems and usage among DSH patients.
Method
Data collected by the Oxford Monitoring System for Attempted Suicide were used to examine trends in alcohol disorders and alcohol consumption shortly before, or at, the time of self-harm by patients aged 15 years or over between 1989 and 2002.
Results
Data were available on 10,414 patients who were involved in 17,511 episodes of DSH. The annual numbers of both male and female DSH patients rose progressively over the study period. Although rates of alcohol disorders and consumption remained higher in males than females, substantial increases were seen in females of all ages in rates of alcohol problems, excessive drinking and consumption of alcohol within 6 h of DSH and as part of the act of DSH. Rates for males largely remained unchanged.
Conclusions
There has been a significant increase in excessive drinking and consumption of alcohol around the time of DSH by females but not males. These changes may relate to increases in the affordability and availability of alcohol and to social changes in drinking patterns. They have implications for services for DSH patients and may have an impact on future patterns of suicidal behaviour.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Alcohol dependence and misuse are strongly associated with suicidal behaviour [15]. The lifetime risk of suicide in patients with alcohol abuse or dependence is almost six times the expected risk [7]. Problems related to alcohol use are commonly found among patients presenting with deliberate self-harm (DSH). For example, in a study of DSH patients presenting to the Regional Poisoning Treatment Centre in Edinburgh between 1968 and 1987, 16.9% of men and 4.6% of women were alcohol-dependant, and 41.5% and 16.4%, respectively, had problem use of alcohol [19]. In another UK study of DSH patients, 51% of men and 31% of women were drinking more than the government-recommended limits (21 U a week for men and 14 U a week for women) [14]. DSH patients who misuse alcohol are at greater risk of both repetition of DSH and of suicide than those without alcohol misuse [9, 20]. They frequently have co-morbid psychiatric disorders, most commonly depression [8, 23].
During the last few decades in the UK there have been changes in the consumption of alcohol by the general population. Per capita consumption of alcohol in the UK has doubled since the late 1950s [1]. Between 1984 and 1996 the proportion of men drinking more than 21 U a week remained fairly constant, while the proportion of women drinking more than 14 U per week rose [5]. Among women the increase in the proportion drinking in excess of government-recommended limits was seen across all age groups. In the UK, mortality rates for deaths related to alcohol consumption (mostly chronic liver disease and cirrhosis) increased steadily in both males and females between 1979 and 2000 [2]. Studies carried out in Oxford suggest that between 1976 and 1997, the proportion of DSH patients with alcohol disorders and excessive drinking may have increased [9, 11].
In this study we have used data from the Oxford Monitoring System for Attempted Suicide [12] to examine DSH patients with alcohol dependence and excessive drinking over a 14-year period. We have also studied trends in the consumption of alcohol within 6 h of the act of self-harm and also the use of alcohol as part of the act. We have particularly focused on trends by gender and age.
Method
The study population consisted of all those patients aged 15 years and over who presented to the general hospital in Oxford following an act of DSH between 1989 and 2002. Most acts involved self-poisoning, whereas the rest involved self-injury or both methods. Self-poisoning is defined as the intentional self-administration of more than the prescribed dose of any drug, whether or not there is evidence that the act was intended to result in death. This also includes poisoning with non-ingestible substances and gas and overdoses of recreational drugs and severe alcohol intoxication, where the clinical staff consider that these cases of DSH.
The majority of patients (70.7% in 2002) undergo detailed psychosocial assessment by a member of the general hospital psychiatric service (usually a psychiatric nurse or junior psychiatrist). Following this assessment the staff member records detailed information about the patient and the episode of DSH on a data entry form. This information includes an item on the misuse of alcohol which is categorised as follows: chronic alcoholism with physical symptoms (for example, liver disease, peptic ulcer, peripheral neuropathy and organic psychological impairment), alcohol dependence (excessive drinking with features of alcohol dependence such as withdrawal symptoms, subjective need of alcohol, progression of drinking behaviour, relief drinking and increased tolerance) and alcohol misuse (regular weekly alcohol consumption in excess of 21 U for men and 14 U for women). The assessing staff member records if, in their opinion, the patient has a problem with alcohol (defined as causing current distress for the patient and/or contributing to the act of DSH). Data are also collected on whether or not alcohol had been consumed within 6 h of the act of DSH or as part of the act. Limited information, derived from case notes and accident and emergency department records, is recorded on those DSH patients who present to the general hospital but who do not undergo assessment by the general hospital psychiatric service. Information from the coded data sheets is then entered into a computerised database. This method of data collection has been demonstrated to be reliable [21].
For the purposes of this study those patients categorised as having chronic alcoholism with physical symptoms and those with alcohol dependence were combined to give a single category of alcohol dependence. The term excessive drinking was used to define those who drank in excess of government-recommended limits but did not have a diagnosis of alcohol dependence.
The data were analysed using SPSS version 11.5 [22] and EpiInfo [4]. The χ 2 test, with Yates correction, and χ 2 for trend, where trends were approximately linear, were used.
For each section in the “Results” we first present summary data based on each patient's first episode during the study period for which they were clinically assessed. We then describe trends over the study period using data based on each patient's first assessed episode in each year of the study period.
Results
Study population
During the 14-year study period, 1989–2002, a total of 10,414 DSH patients presented to the general hospital in Oxford. Of these 10,414 patients, 8,686 (83.4%) were assessed by the general hospital psychiatric service at their first presentation in the study period. Of those who were assessed, it was known for 7,916 (91.1%) whether or not they were misusing alcohol. The 10,414 patients were involved in a total of 17,511 episodes of DSH. For 12,092 of these episodes a psychosocial assessment was carried out.
Alcohol dependence and misuse of alcohol among DSH patients
A total of 8.6% of DSH patients were diagnosed as suffering from alcohol dependence at the first assessed episode during the study period (see Table 1). Alcohol dependence was more common in males than in females. Excessive drinking, present in a total of 23.4% of DSH patients, was also significantly more common in males than in females.
Method of DSH
Of the 12,092 assessed episodes during the study period, 88.2% involved self-poisoning, 7.0% involved self-injury and 4.8% involved both methods. Female patients with alcohol dependence or excessive drinking were more likely to present with an episode involving self-injury than those with no misuse of alcohol (12.4 vs. 8.6%, χ 2=24.1%, 1 df, P<0.00001). The findings for male patients were not statistically significant.
Trends in alcohol dependence, 1989–2002
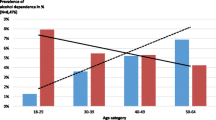
The annual overall number of male DSH patients showed a progressive rise throughout the study period, while the proportion of male patients with a diagnosis of alcohol dependence did not change significantly (see Table 2). Rates of alcohol dependence were highest in the oldest age group (≥45 years) and lowest in those aged 15–24 years (see Fig. 1). Rates of male alcohol dependence fell over the study period in the 25- to 44-years age group (χ 2 for trend 10.2; P<0.005), which was the age group with the largest number of patients.

Alcohol dependence by gender and age groups, 1989–2002 (3-year moving averages)
The annual number of female DSH patients rose progressively during the study period (see Table 2). Although the absolute numbers of female patients with a diagnosis of alcohol dependence increased with time, there was no significant increase in the overall proportion of female patients with a diagnosis of alcohol dependence. However, rates of alcohol dependence in females aged at least 45 years did increase during the study period (χ 2 for trend 4.99; P<0.05). Rates of alcohol dependence in females in those aged 25–44 and at least 45 years and over were higher than those for the 15- to 24-years age group (see Fig. 1).
Trends in excessive drinking, 1989–2002
The proportion of DSH patients with a diagnosis of excessive drinking rose during the study period (see Table 3). For males, rates of excessive drinking showed no significant overall change, although the rate for males aged at least 45 years and over rose during the mid-1990s (see Table 3 and Fig. 2). The absolute numbers of males with excessive drinking did, however, increase (223 for the years 1989–1991 compared with 305 for 2000–2002).

Excessive drinking by gender and age groups, 1989–2002 (3-year moving averages)
For females, there was a substantial increase from the mid-1990s in the proportion with a diagnosis of excessive drinking (see Table 3 and Fig. 2). The proportion of female patients with excessive drinking rose from 191/1,064 (18.0%) for the period 1989–1991 to 378/1,418 (26.7%) for the period 2000–2002 (χ 2 for trend 32.2; P<0.00001). The absolute number of female excessive drinkers almost doubled between 1989–1991 and 2000–2002. Rates of excessive drinking were highest throughout for the 25- to 44-years age group. Rates of excessive drinking increased significantly in all three age groups during the study period (15–24 years: χ 2 for trend 22.2, P<0.00001; 25–44 years: χ 2 for trend 18.6, P<0.00005; and ≥45 years: χ 2 for trend 7.28, P<0.01).
Alcohol as a problem
During the study period, a total of 23.5% of DSH patients were regarded as having a problem with alcohol (alcohol was causing current distress and/or contributing to the attempt). Males were much more likely than females to have a problem with alcohol [1,085/3,441 (31.5%) vs. 885/4,943 (17.9%); χ 2=208.8, 1 df, P<0.00001]. The proportion of males with an alcohol problem fell during the early 1990s and then rose, but there was no significant increase overall (see Fig. 3). There was a steady increase in the proportion of females in all three age groups with an alcohol problem (15–24 years: χ 2 for trend 5.90, P<0.05; 25–44 years: χ 2 for trend 12.8, P<0.0005; and ≥45 years: χ 2 for trend 11.8, P<0.001).

Alcohol recorded as a problem for the patient, by age group, 1989–2002 (3-year moving averages)
Alcohol consumed within 6 h of DSH
Overall, 46.1% of DSH patients (at first assessed episode during the study period) consumed alcohol within 6 h of DSH. Males were more likely than females to have consumed alcohol [1,799/3,356 (53.6%) vs. 1,987/4,849 (41.0%); χ 2=126.8, 1 df, P<0.00001].
Patients with alcohol dependence or excessive drinking at their first assessed episode during the study period were more likely to have consumed alcohol within 6 h of DSH than those without either of these diagnoses [alcohol dependence (90.1%) vs. excessive drinking (80.0%) vs. no alcohol misuse (28.9%); χ 2=1,969.1, 2 df, P<0.00001].
Trends in consumption of alcohol within 6 h of DSH
The proportion of males consuming alcohol within 6 h of DSH (at their first assessed episode in each year) remained fairly constant during the study period, with slightly higher rates in those aged 25–44 and 44 years and over than in those aged 15–24 years (see Fig. 4). For females, there was a significant increase in all three age groups in the proportion consuming alcohol within 6 h of DSH (15–24 years: χ 2 for trend 4.44, P<0.05; 25–44 years: χ 2 for trend 11.4, P<0.001; and ≥45 years: χ 2 for trend 35.4, P<0.00001). Rates were higher in those aged 25–44 years than in those aged 15–24 years. The largest increase was seen in those aged 45 years and over.

Alcohol consumed within 6 h of DSH, by gender and age groups, 1989–2002 (3-year moving averages)
Alcohol consumed as part of the act of DSH
Alcohol was consumed as part of the act of DSH by 26.0% of patients at their first assessed episode during the study period. Males consumed alcohol more frequently than females [984/3,218 (30.6%) vs. 1,081/4,721 (22.9%); χ 2=58.3, df 1, P<0.00001].
Patients with a diagnosis of alcohol dependence or excessive drinking were more likely to have consumed alcohol as part of the act of DSH than those without these diagnoses (alcohol dependence (59.9%) vs. excessive drinking (40.2%) vs. no alcohol misuse (17.0%); χ 2=767.0, 1 df, P<0.00001).
Trends in consumption of alcohol as part of the act of DSH
For males, there was no significant change during the study period in the proportion consuming alcohol as part of the act of DSH (see Fig. 5) (figures based on patients' first assessed episode in each year). The rate was lower in the 15- to 24-years age group than in the two older age groups. By contrast, for females, there was a significant increase in all three age groups in the proportion consuming alcohol as part of the act (15–24 years: χ 2 for trend 15.7, P<0.0001; 25–44 years: χ 2 for trend 19.0, P<0.00005; and ≥45 years: χ 2 for trend 14.1, P<0.0005). Again, the rate was lower in the 15- to 24-years age group than in the two older age groups.

Alcohol consumed as part of the act of DSH, by gender and age groups, 1989–2002 (3-year moving averages)
Discussion
In this study, we have shown that among female DSH patients presenting to the general hospital in Oxford between 1989 and 2002, an increasing proportion had problems related to alcohol use (excessive drinking, alcohol as a problem and consumption of alcohol within 6 h of and at the time of DSH). The increasing rates in females affected all three age groups studied (15–24, 25–44 and ≥45 years). These increases occurred only in female patients, although males continued to have higher rates than females. While males continued to have higher rates of alcohol dependence, excessive drinking and consumption of alcohol at or before DSH than females, there was no marked change in these over the study period.
Overall, alcohol disorders were very common, with 8.6% of DSH patients having a diagnosis of alcohol dependence and 23.4% having a diagnosis of excessive drinking. Our finding of 8.6% of patients with a diagnosis of alcohol dependence is similar to the findings of an earlier study (1976–1985) that also used data from the Oxford Monitoring System for Attempted Suicide, in which 7.9% of patients had a diagnosis of alcohol dependence [9].
It is not clear if our findings among Oxford DSH patients of rising rates of alcohol misuse and consumption of alcohol shortly before, or as part of, the DSH act are part of a national trend. At present there are no contemporary reports from other UK centres with which to compare our findings. In an earlier report from the regional poisoning centre in Edinburgh based on the years 1968–1987, rates of alcohol dependence and the use of alcohol as part of the act of DSH had increased in females but not in males [19]. The population served by the general hospital in Oxford (and hence covered by the Oxford Monitoring System for DSH) includes a relatively large number of young people. However, previous studies of DSH patients in general suggest that trends in DSH seen in Oxford are reasonably representative of trends seen in other UK centres (e.g. [3, 18].
The rise in the proportion of DSH patients with alcohol-related problems places an increasing burden on both medical and psychiatric resources. Co-morbid psychiatric disorders such as depression and personality disorder are commonly present in these patients [8, 23]. Their treatment may require input from and good communication between multiple agencies, e.g. liaison psychiatric services, community mental health teams and substance misuse services. However, DSH patients with alcohol-related problems do not readily engage with traditional alcohol services and, women in particular, may not see alcohol as a major problem. The increasing proportion of DSH patients consuming alcohol within 6 h of, and as part of the act of DSH is also a matter of concern. Alcohol intoxication complicates the medical treatment of DSH and increases the lethality of acts of self-poisoning, e.g. those involving paracetamol, co-proxamol and sedatives. It may also necessitate or prolong hospitalisation for medical treatment. Alcohol intoxication makes psychosocial assessment more difficult, and a detailed assessment may need to be deferred until the patient is sober. This again may prolong hospitalisation.
The increasing use of alcohol by DSH patients reported in Oxford is likely to be a reflection of national changes in the consumption of alcohol. Unlike many other European countries, per capita consumption of alcohol has risen by 50% in the UK since 1970 [1]. Alcohol has become increasingly affordable, as its price relative to income has fallen. Alcohol is also more readily available, given the rise in the number of licensed premises and the progressive relaxation in licensing laws that have taken place in the UK during the last few decades. In 1988 the Licensing Act of 1964 was amended to permit all-day weekday opening for pubs and places selling alcoholic beverages. In 1995 a further amendment was passed allowing all-day opening on Sundays. In a prospective study of Scottish DSH patients, the proportions of both male and female patients consuming alcohol at the time of DSH showed a substantial increase from 1977 onwards following the relaxation of Scotland's liquor licensing laws in December 1976 [17]. Lifestyle changes, an increase in the acceptability of drinks and heavy drinking and the impact of advertising have also been cited as important influences on alcohol consumption [1]. While alcohol consumption by men remained roughly constant between 1984 and 1996 at a mean of 16 U/week, consumption by women increased from 4.9 U/week in 1984 to 6.3 U/week in 1996 [5]. During this time period, the proportion of men drinking in excess of government-recommended limits remained constant at 27%, while the proportion of women rose from 10% in 1984 to 14% in 1996.
The increases in the proportion of DSH patients misusing alcohol and consuming alcohol shortly before, or as part of, the act of DSH have implications for mental health services. All DSH patients should have a psychosocial assessment [16], including an inquiry about past and current alcohol consumption and patterns of drinking. Patients with problem use of alcohol require careful assessment after DSH. Alcohol use is a risk factor for suicide [15] and, in addition, DSH patients with alcohol misuse have a higher repetition rate than those without alcohol misuse [9, 11]. Co-morbid psychiatric disorders need treatment, and this may require a liaison between multiple treatment agencies [10]. In the past, many alcohol treatment services have concentrated more resources on people with alcohol dependency rather than on the much larger number of people using alcohol in a harmful way, despite the fact that this latter group contributes the greater share of alcohol-related harm to society [13]. Given our finding of an increasing proportion of female DSH patients with excessive drinking, alcohol services may need to shift their focus onto this group. Their presentation at the general hospital in the context of DSH should be seen as an opportunity for engagement in the treatment of their problem drinking. There is inconclusive evidence that opportunistic brief interventions are effective for psychiatric patients with hazardous and harmful drinking [6], although further trials are needed and should be extended to include DSH patients. It is likely that DSH patients with excessive drinking would require more than a brief intervention, and might benefit from a more tailored intervention, including motivational enhancement therapy and coping skills training. The increases in excessive drinking and problem use of alcohol are also likely to impact upon patterns of suicidal behaviour.
References
Academy of Medical Sciences (2004) Calling time: the nation's drinking as a major health issue. http://www.acmedsci.ac.uk/p_callingtime.pdf. Cited September 2004
Baker A, Rooney C (2003) Recent trends in alcohol-related mortality, and the impact of ICD-10 on the monitoring of these deaths in England and Wales. Health Stat Q 17:5–14
Bialas MC, Reid PG, Beck P, Lazarus JH, Smith PM, Scorer RC, Routledge PA (1996) Changing patterns of self-poisoning in a UK health district. Q J Med 89:893–901
Dean AG, Dean JA, Coulombier D, Brendel KA, Smith DC, Burton AH, Dicker RC, Sullivan K, Fagan RF, Arner TG (1994) EpiInfo version 6: a word processing database and statistics program for epidemiology on microcomputers. Centers for Disease Control and Prevention, Atlanta, GA
Department of Health (1999) Statistics on alcohol: 1976 onwards. Statistical Bulletin 1999/24. http://www.dh.gov.uk/assetRoot/04/02/15/12/04021512.pdf. Cited September 2004
Emmen MJ, Schippers GM, Bleijenberg G, Wollersheim H (2004) Effectiveness of opportunistic brief interventions for problem drinking in a general hospital setting: systematic review. BMJ 328:318–320
Harris EC, Barraclough B (1997) Suicide as an outcome for mental disorders. A meta-analysis. Br J Psychiatry 170:205–228
Haw C, Houston K, Townsend E, Hawton K (2001) Deliberate self harm patients with alcohol disorders: characteristics, treatment and outcome. Crisis 22:93–101
Hawton K, Fagg J, McKeown S (1989) Alcoholism, alcohol and attempted suicide. Alcohol Alcohol 24:3–9
Hawton K, Houston K, Haw C, Townsend E, Harriss L (2003) Comorbidity of Axis 1 and Axis II disorders in patients who attempted suicide. Am J Psychiatry 160:1494–1500
Hawton K, Simkin S, Fagg J (1997) Deliberate self-harm in alcohol and drug misusers: patient characteristics and patterns of clinical care. Drug Alcohol Rev 16:123–129
Hawton K, Fagg J, Simkin S, Bale E, Bond A (1997) Trends in deliberate self-harm in Oxford, 1985–1995. Implications for clinical services and the prevention of suicide. Br J Psychiatry 171:556–560
Humphries K, Tucker JA (2002) Towards more responsive and effective intervention systems for alcohol-related problems. Addiction 97:126–132
Merrill J, Milner G, Owens J, Vale A (1992) Alcohol and attempted suicide. Br J Addict 87:83–89
Murphy G (2000) Psychiatric aspects of suicidal behaviour: substance abuse. In: Hawton K, Van Heeringen K (eds) The International handbook of suicide and attempted suicide. Wiley, Chichester, pp 135–146
National Institute for Clinical Excellence (2004) Clinical guideline 16. Self-harm: the short-term physical and psychological management and secondary prevention of self-harm in primary and secondary care. NICE, London
Northridge DB, McMurray J, Lawson AAH (1986) Association between liberalisation of Scotland's liquor licensing laws and admissions for self poisoning in West Fife. BMJ 293:1466–1468
Platt S, Hawton K, Kreitman N, Fagg J, Foster J (1988) Recent clinical and epidemiological trends in parasuicide in Edinburgh and Oxford: a tale of two cities. Psychol Med 18:405–418
Platt S, Robinson A (1991) Parasuicide and alcohol: a 20 year survey of admissions to a regional poisoning treatment centre. Int J Soc Psychiatry 37:159–172
Sakinofsky I (2000) Repetition of suicidal behaviour. In: Hawton K, Van Heeringen K (eds) The International handbook of suicide and attempted suicide. Wiley, Chichester, pp 385–404
Sellar C, Goldacre MJ, Hawton K (1990) Reliability of routine hospital data on poisoning as measures of deliberate self poisoning in adolescents. J Epidemiol Community Health 44:313–315
SPSS (2002) SPSS Base 11.5 Windows users guide. SPSS, Chicago
Suominen KH, Isometsä ET, Henriksson MM, Ostamo AI, Lönnqvist JK (1999) Treatment received by alcohol-dependent suicide attempters. Acta Psychiatr Scand 99:214–219
Acknowledgements
The Oxford Monitoring System for Attempted Suicide is supported by a grant from the Department of Health. K.H. is also supported by Oxfordshire Mental Healthcare Trust. C.H. is supported by St. Andrew's Hospital, Northampton. We thank the staff of the Department of Psychological Medicine, John Radcliffe Hospital (Drs. Christopher Bass and Eleanor Feldman, Karen Carroll, Sharon Codd, Hilary Corcoran, Ann Dolan, Claire Lewin-Leigh, John Ryall, Heather Weizel and Linda Whitehead) for their considerable assistance with the data collection.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Haw, C., Hawton, K., Casey, D. et al. Alcohol dependence, excessive drinking and deliberate self-harm. Soc Psychiat Epidemiol 40, 964–971 (2005). https://doi.org/10.1007/s00127-005-0981-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-005-0981-3