
Abstract
Background
Global assessment of functioning, quality of life (QOL) and patient needs have been discussed as inter-related domains important for care planning and outcome assessment in care for the severely mentally ill. The study was conducted to investigate relationships of functioning level, subjective QOL and unmet needs in a cross-sectional study of 404 patients with schizophrenia spectrum disorders in five European centres with a focus on the patient group with low function scores.
Methods
Patient groups with low, medium and high function scores were compared with regard to subjective QOL and unmet needs. QOL variability was assessed in subgroups according to function scores. Regression analyses were used to examine the impact of illness-related and other unmet patient needs on QOL. The influence of individual needs in the low and medium/high function score subgroup was compared.
Results
QOL increased and unmet needs decreased from the low to high function score subgroup. There was greater QOL variability in patients with low function scores compared to those with medium and high function scores, with some low-function score patients having relatively high QOL. In the low function score subgroup, both illness-related and other needs had an impact on QOL, whereas non-illness needs influenced QOL in medium and high function score patients.
Conclusion
Scores of functioning level, in people with schizophrenia spectrum disorders, are related to QOL in a complex way, and types of unmet need impinge on the relationship. In order to improve QOL in people with low function scores, both illness-related and other needs should be met.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The improvement of subjective quality of life (QOL) is regarded as a key challenge in providing mental health care for people with severe mental illness (SMI), in particular for those with very low scores on global functioning scales [18, 19]. To accomplish this target, it is necessary to understand what particular type of care persons with severe functional impairment due to mental illness require, and whether mental health services are suited to provide it. Currently, however, the interrelations between levels of functioning, subjective QOL and mental health care needs are not fully understood.
While Gaite et al. [12] found that the level of functioning as measured by the DSM-III Axis 5 Global Assessment of Functioning (GAF) scale was positively related to subjective QOL when used as a single predictor, the relationship disappeared when other clinical variables were included in the regression model. Similarly, the authors of the UK 700 study discovered that functional disability as assessed by the Disability Assessment Scale (DAS) had a negative impact on subjective QOL when only social variables were included in data analysis, but the relationship disappeared when the severity of psychopathological symptoms was added to the regression equation [29]. In a regression model, Ruggeri et al. [25, 26] found that friction with social contacts was the only DAS subscale associated with more than one QOL domain. In a longitudinal study, Kilian et al. [16] found a cross-sectional but no longitudinal positive effect of general functioning assessed by the GAF on subjective QOL. In contrast, met and unmet needs for care were found to be negatively related to subjective QOL in all of the few studies published so far. In the UK 700 trial, patients’ unmet basic, social and functioning needs were the strongest single predictors of subjective QOL [29]. Wiersma and Busschbach [30] found the number of needs and QOL to be negatively correlated, and the same applied to patient satisfaction. Hansson et al. [13] also detected a strong negative relationship between unmet need and QOL (in all QOL domains), and this relationship was strongest for subjective QOL.
In order to better understand the unclear relationship between functioning level and subjective QOL on one hand, and the clear negative QOL impact of needs for care on the other, reference to more generic QOL findings in persons with SMI may be helpful. Many studies on the QOL of persons with psychiatric disorders have reported that objective indicators of QOL and subjective QOL are only poorly related [3, 4, 22, 23, 25, 26, 28, 31]. In discussing this finding, some authors suggested that the subjective evaluation of objective living conditions is influenced by processes of human adaptation [2, 14, 31]. Results presented by Franz et al. [9, 10] confirm the role of adaptation processes particularly in deprived living situations. In one study they found that long-stay in-patients with SMI tended to compare their living conditions mainly with those of other inmates, whereas short-stay in-patients compared their living conditions mainly with healthy people [9]. As a consequence of their “upward” comparisons, short-stay patients assessed their subjective QOL worse than long-stay in-patients who made internal or “downward” comparisons. In a further quasi-experimental study including long-stay patients with SMI, Franz et al. [10] discovered that while a sudden decrease in objective QOL caused a short-term decrease in subjective QOL most of the study participants regained their former QOL level after a short period.
Against the background of these findings, it can be suspected that the relationship between level of functioning, needs for care and subjective QOL is mediated by processes of adaptation. Needs for mental health care can be regarded as being caused by functional impairment, but patient needs may vary at different levels of functioning due to adaptation processes. As a consequence, the needs and components of care which are relevant for subjective QOL could differ between patients with low scores on functioning scales and those with higher functioning scores.
In order to improve the understanding of the relationships between functioning levels, needs for care and subjective QOL this paper will address the following research questions:
-
1.
How do patient subgroups with high, medium and low functioning scores differ with respect to their QOL appraisal, in terms of both QOL level and QOL variability?
-
2.
How do patients with low scores on functioning scales differ from subgroups with medium and high functioning scores with respect to the association of QOL with specific types of need?
Materials and methods
The EU-funded EPSILON study was conducted with the following aims: (1) to develop research instruments applicable in different European countries, and (2) to develop a cross-sectional description of care for people with schizophrenia and schizophrenia spectrum disorders in five European sites. It was performed in community mental health services for catchment areas in Amsterdam, Copenhagen, London, Santander and Verona. Mental health services in the sites, patient recruitment and study methodology have been described elsewhere [5–7, 27].
Patient sample
A total of 404 patients were recruited, and all patients suffered from a severe mental disorder with ICD-10 diagnoses ranging from F20 to F25. The majority of patients were male, mean age was 42 years, 65% of patients were single, and there were substantial differences in terms of ethnicity (white European 54–100%), living situation (living alone 7–65%), and occupational status (unemployed 57–92%) across the sites. The average GAF score was 57.3 [17].
Instruments
To assess functioning, the Global Assessment of Functioning scale was used [1]. To assess QOL, we used the Lancashire Quality of Life Profile–European Version (LQoLP-EU), which is focused on satisfaction with life in different life domains on a 7-point Likert scale ranging from ‘can’t be better’ (rating of 7) to ‘can’t be worse’ (rating of 1) [11]. In addition to the life domain scores (which can be averaged to produce a single score), there is also a two-item global well being question. The Camberwell Assessment of Need–European Version (CAN-EU) was used to assess (met and) unmet patient needs [20].
Statistical methods
GAF scores were categorised into three severity levels: low (≤50), medium (51–70) and high (>71) [24]. Average domain-specific QOL, defined as the average of domain scores of the LQoLP-EU, was analysed in terms of unmet needs. These were divided into two groups: mental illness-related (symptoms, psychological distress, treatment information, safety to self, safety to others, alcohol and drugs), and non-illness related needs (all 15 others). These two groups of needs were used as potential explanatory variables in regressions with the average domain QOL measure as dependent variable and controlling for centre. Interactions between the GAF score level (low, medium, high) and types of need were also tested to assess whether different models applied to patients at different levels of functioning scores. The models were refitted controlling for length of illness in case this would turn out to be a confounding factor. Other characteristics of the three subgroups according to GAF (low, medium, high) were compared using regression (linear regressions, and multiple and binary logistic regressions), both unadjusted and adjusted for centre. Risk ratios for individual unmet needs (comparing the low to the combined medium and high functioning groups) were estimated. SPSS version 11 and STATA version 8 were used for the analyses.
Results
Overall comparisons between subgroups based on global function scores
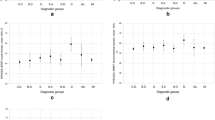
Table 1 describes the subgroups with low, medium and high functioning (GAF) scores in terms of socio-demographic variables, age, QOL, and needs. When the analyses were adjusted for centre effects, the functioning subgroups differed (1) in terms of living situation (more living alone, and fewer with spouse in the group with low function scores), and (2) in terms of occupational status (more patients being unemployed in the group with low function scores). Both average domain-specific QOL and Global Well Being scores increased steadily from the group with low function scores to that with high function scores. However, the standard deviations declined, significantly in the case of Global Well Being, P<0.001 for test of differences in standard deviations, ‘low functioning’ group compared to the other two, P=0.001 comparing ‘low’ to ‘medium’ group). The group with low function scores had a relatively wide spread of global well being: while some individuals in this group report a very much worse QOL than average, there is also a proportion of individuals with relatively high QOL.
Unmet needs decreased throughout the functioning groups from low to high, both for illness and non-illness needs. These two types of need were correlated with each other (r=0.36, P<0.001; r=0.280, P<0.001 controlling for functioning group). In the ‘low’ functioning group, 18% had no needs and 48% at least one of each type of need. In the ‘medium’ group, 30% had no needs and 24% had at least one of each type of need; in the ‘high’ functioning group, 64 and 8% had at least one of each type of need.
Association between quality of life and unmet needs by subgroup based on function scores
Average domain-specific QOL was used as the dependent variable in regression analyses. Totals of unmet (illness and non-illness) needs were used as potential explanatory variables in regressions, controlling for centre, and regressions were fitted for each of the three subgroups according to functioning scores. In a global model based on the whole sample, the P for the interaction between type of need and low GAF category vs medium/high GAF category was 0.78 for illness needs, and 0.026 for other needs. The models were refitted for each GAF category separately (Table 2). The beta weights for illness needs decreased from the low to high function score subgroups, whereas the opposite was true for non-illness needs. In the low function score subgroup, there was a smaller difference between the betas for illness and other needs, and the unstandardised coefficients were almost the same (and both types of need were significant). For the medium function score and high function score groups, on the other hand, the illness needs had a relatively low association with QOL compared to other needs.
The mean lengths of illness differed significantly between the functioning groups (see Table 1). However, quality of life was only weakly (negatively) correlated with length of illness (r=0.1, P=0.056). When length of illness was included in the above regressions, the results were very little changed and showed the same progression from illness to non-illness needs as with the better functioning groups.
Specific quality of life domains and function score level
Domain-specific QOL was classified as low vs medium/high at 4.3 (the lowest QOL tertile from the average domain-specific QOL rating). In the high function score group, no individual QOL domain was rated lower than this. In the medium function score group work and finance were rated lower than this level, and in the low function score group, ratings for four domains (work, finance, health and social) were in the low QOL range.
Specific types of unmet need and function score level
Table 3 shows the complete list of unmet needs by low and medium/high function score groups combined, ordered according to the most commonly reported needs in the group with low GAF scores. Unmet needs that were significantly more common among the low function score group are shown in bold, and those needs significantly associated with QOL in the low function score group are also indicated by superscripts (see footnotes). The individual unmet needs that were significantly associated with QOL for the low function score group were as follows: psychotic symptoms, daytime activities, information, benefits and self-harm; psychological distress and food were also associated at a borderline level of significance.
Discussion
In this cross-national study, QOL improved from the subgroup with low global function scores to that with high GAF scores. In the low function score group a marked QOL variability was found, especially in Global Wellbeing, with some patients having very QOL low and others having reasonably high QOL (question 1). The association with QOL was strong for both illness and non-illness related needs in the low function score subgroup, whereas only non-illness related needs were associated with QOL in the intermediate and high function score subgroup (question 2). The number of QOL domains that were below a cut-off level increased in the low function score subgroup and included health and social domains as well as work and finance.
There is a group of specific unmet needs that are (1) more common among the group with low function scores than among patients with higher function scores, and that are (2) associated with QOL in the low function score group. These are illness-related needs (symptoms, distress, self-harm and information about treatment) and a few non-illness needs (daytime activities, benefits and food) (question 2). In other words, both illness needs and basic non-illness needs appear to be important in understanding QOL among patients with low function scores, and this finding is helpful in identifying priorities for care in this patient subgroup.
Limitations and strengths
The many variables involved may have led to a problem of multiple testing. For this reason, the analysis has first considered only two concepts (total illness needs and total non-illness needs). The findings regarding individual needs and QOL domains are thus exploratory and serve to expand on the conclusions from the initial analysis. P values for these are indicative of associations for which there is most evidence in this study sample. On the other hand, this is one of a small number of cross-national studies of care for people with schizophrenia, and there are few patient samples of this size studied with research instruments which were translated, back-translated and validated for use in the respective countries [8]. Another limitation to be borne in mind is the cross-sectional design of the EPSILON study.
Suggestions for further work
The present study had a cross-sectional design; ideally, a longitudinal design would lead to more clear-cut conclusions. However, study results can be used to suggest areas for further research. The specific unmet needs that are particularly associated with the group with low function scores can be linked to QOL domains: psychotic symptoms, psychological distress, information about treatment, self-harm and physical health (health domain); daytime activities and company (social domain); benefits, money and, perhaps more tenuously, food (finance domain). While the study of these associations is beyond the scope of the EPSILON study (in terms of study scope and sample size), it could be achieved by studies providing targeted interventions for patients with very low function scores and assessing these against improvements in the relevant QOL domains.
If, in a sample of people with SMI, some or all illness needs could be met among those patients with low function scores, one might hope to observe prospectively an improvement in QOL, with the health domain in particular improving. Introducing information about treatment or measures to alleviate psychological distress might improve QOL without affecting the level of functioning. Future studies should also deal with the problem that concepts used in such studies (e.g., QOL or needs) may not be sufficiently distinct to avoid circular reasoning [21].
Importance of illness needs in the patient group with low function scores
Differential effects of types of need on QOL according to the functioning level, with both illness and non-illness needs being important in low function score patients and non-illness needs impinging more in patients with high function scores, may reflect a shift in the patient perspective on the relative importance of core needs depending on his/her functioning level. Kemmler et al. [15] found psychiatric symptom levels to correlate negatively with subjective QOL among patients with a low to medium level of psychopathological impairment. In those with high symptom levels there was a trend towards higher subjective QOL ratings, and patients with very marked negative symptoms also had higher QOL levels. This type of finding could be due to adaptation processes with regard to QOL occurring in some patients with low function scores. The present study, being cross-sectional, cannot address the issue of adaptation processes in QOL appraisal by patients with SMI. However, the finding of relatively high QOL ratings in some patients with low function scores is compatible with adaptation processes occurring in some members of this subgroup.
Implications for clinicians
In this study illness needs were found, in general, to have a strong impact on QOL in patients with low function scores, whereas non-illness needs contributed relatively more to QOL in the patient group with high function scores. Illness needs included ‘psychotic symptoms’, ‘psychological distress’, ‘information about treatment’, ‘safety to self and others’, and ‘alcohol and drugs’, whereas non-illness needs included all 15 other needs assessed by the CAN. In an intuitive model severe illness would imply high levels of suffering and distress, and the condition would require much of the attention of an individual suffering from the condition. Our findings suggest that the weight of directly illness-related needs declines relative to other needs as the level of functioning improves. The individual non-illness related needs that were found to be relevant in the low function score group were of a very basic type, and could be partially met, for instance, by providing more day-care facilities providing company, activities and food. In designing a service for people with schizophrenia with low function scores, one should therefore take into account a wide range of illness and non-illness needs. In planning adequate mental health services, it should also be borne in mind that the emphasis may shift from illness-related needs to a wider range of social, financial and other daily life needs as the functioning level of those suffering from SMI improves.
References
American Psychiatric Association (1987) Diagnostic and statistical manual of mental disorders (DSM-III-R), 3rd edn. APA, Washington, DC
Angermeyer MC, Kilian R (1997) Theoretical models of quality of life for mental disorders. In: Katschnig H, Freeman H, Sartorius N (eds) Quality of life in mental disorders. Wiley, Chichester, pp 19–30
Atkinson M, Zibin S, Chuang H (1997) Characterizing quality of life among patients with chronic mental illness: a critical examination of the self-report methodology. Am J Psychiatry 154:99–105
Bechdolf A, Klosterkötter J, Hambrecht M, Knoost B, Kuntermann C, Schiller S et al (2003) Determinants of subjective quality of life in post acute patients with schizophrenia. Eur Arch Psychiatr Clin Neurosci 253:235–328
Becker T, Knapp M, Knudsen HC, Schene A, Tansella M, Thornicroft G et al (1999) The EPSILON study of schizophrenia in five European countries. Design and methodology for standardising outcome measures and comparing patterns of care and service costs. Br J Psychiatry 175:514–521
Becker T, Knapp M, Knudsen H, Schene A, Tansella M, Thornicroft G et al (2000) Aims, outcome measures, study sites and patient sample. EPSILON study 2. Br J Psychiatry 39(Suppl):s1–s7
Becker T, Hülsmann S, Knudsen H (2002) Provision of services for people with schizophrenia in five European regions. Soc Psychiatry Psychiatr Epidemiol 37:465–474
Beecham J, Munizza C (2000) Introduction: assessing mental health in Europe. Acta Psychatr Scand 102(Suppl. 4054):5–7
Franz M, Meyer T, Reber T, Gallhofer B (2000) The importance of social comparisons for high levels of subjective quality of life in chronic schizophrenic patients. Qual Life Res 9:481–489
Franz M, Meyer T, Spitznagel A, Schmidth H, Wening K, Gallhofer B (2001) Responsiveness of subjective quality of life assessment in schizophrenic patients: a quasi-experimental pilot study. Eur J Psychiatry 16:99–103
Gaite L, Vázques-Barquero JL, Arraiga Arrizabalaga A, Schene AH, Welcher B, Thornicroft G et al (2000) Internal consistency of the Lancashire Quality of Life Profile–EU Version (LQoLP-EU) EPSILON study 8. Br J Psychiatry 39(suppl):s49–s54
Gaite L, Vázques-Barquero JL, Borra C, Ballesteros J, Schene A, Welcher B et al (2002) Quality of life in patients with schizophrenia in five European countries: the EPSILON study. Acta Psychiatr Scand 105:283–292
Hansson L, Sandlund M, Bengtsson-Tops A et al (2003) The relationship of needs and quality of life in persons with schizophrenia living in the community. A Nordic multi-center study. Nord. J Psychiatry 57:5–11
Katschnig H (2000) Schizophrenia and quality of life. Acta Psychiatr Scand 102(Suppl. 407):33–37
Kemmler G, Meise U, Tasser A, Liensberger D, Schifferle I, Braitenberg M et al (1999) Subjektive Lebensqualität schizophren Erkrankter. Einfluss von Behandlungssetting, Psychopathologie und extrapyramidalmotorischen Medikamentennebenwirkungen. Psychiat Prakt 26:9–15
Kilian R, Dietrich S, Toumi M, Angermeyer MC (2004) Quality of life in persons with schizophrenia in out-patient treatment with first- or second-generation antipsychotics. Acta Psychiatr Scand 110(2):108–118
Knapp M, Chisholm D, Leese M, Amaddeo F, Tansella M, Schene A et al (2002) Comparing pattern and costs of schizophrenia care in five European countries: the EPSILON study. Acta Psychiatr Scand 105:42–54
Lamb HR (1981) What did we really expect from deinstitutionalization? Hosp Commun Psychiatr 32:105–109
Lamb HR (1982) Treating the long-term mentally ill. Jossey-Bass, San Francisco
McCrone P, Leese M, Thornicroft G, Schene A, Knudsen HC, Vázques-Barquero JL et al (2000) The reliability of the Camberwell Assessment of Need–EU Version CAN-EU). Br J Psychiatry 39(suppl):s34–s40
Priebe S, Kaiser W, Huxley PJ, Roder-Wanner UU, Rudolf H (1998) Do different subjective evaluation criteria reflect distinct constructs? J Nerv Ment Dis 186(7):385–392
Röder-Wanner UU, Priebe S (1998) Objective and subjective quality of life of first-admitted women and men with schizophrenia. Eur Arch Psychiatr Clin Neurosci 248:250–258
Rössler W, Salize HJ, Cucchiaro G, Reinhard I, Kernig C (1999) Does the place of treatment influence the quality of life of schizophrenics? Acta Psychiatr Scand 100:142–148
Ruggeri M, Leese M, Thornicroft G, Bisoffi G, Tansella M (2000) Definition and prevalence of severe and persistent mental illness. Br J Psychiatry 177:149–155
Ruggeri M, Warner R, Bisoffi G, Fontecedro L (2001) Subjective and objective dimensions of quality of life in psychiatric patients: a factor analytical approach. Br J Psychiatry 178:268–275
Ruggeri M, Gater R, Bisoffi G, Barbui G, Tansella M (2002) Determinants of subjective quality of life in patients attending community-based mental health services. The South-Verona Outcome Project 5. Acta Psychiatr Scand 105:131–140
Thornicroft G, Tansella M, Becker T, Knapp M, Leese, M, Schene A, Vázquez-Barquero JL, and the EPSILON Study Group (2004) The personal impact of schizophrenia in Europe. Schizophr Res 69:125–132
Trauer T, Duckmanton RA, Chiu E (1998) A study of the quality of life of the severely mentally ill. Int J Soc Psychiatr 44:79–91
UK 700 Group (1999) Predictors of quality of life in people with severe mental illness. Study methodology with baseline analysis in the UK 700 trial. Br J Psychiatry 175:426–432
Wiersma D, Busschbach J (2001) Are needs and satisfaction of care associated with quality of life? An epidemiological survey among the severely mentally ill in the Netherlands. Eur Arch Psychiatr Clin Neurosci 251:239–246
Zissi A, Barry MM, Chochrane R (1998) A mediational model of quality of life for individuals with severe mental health problems. Psychol Med 28:1221–1230
Acknowledgements
The following colleagues contributed to the EPSILON Study: Amsterdam—Dr. Maarten Koeter, Dr. Karin Meijer, Dr. Marcel Monden, Professor Aart Schene, Dr. Madelon Sijsenaar, Dr. Bob van Wijngaarden; Copenhagen—Dr. Helle Charlotte Knudsen, Dr. Anni Larsen, Dr. Klaus Martiny, Dr. Carsten Schou, Dr. Birgitte Welcher; London—Professor Thomas Becker, Dr. Jennifer Beecham, Liz Brooks, Daniel Chisholm, Gwyn Griffiths, Professor Martin Knapp, Dr. Morven Leese, Paul McCrone, Sarah Padfield, Professor Graham Thornicroft, Dr. Ian White; Santander—Andres Arriaga Arrizabalaga, Dr. Luis Gaite, Modesto Perez Retuerto, Professor José Luis Vázquez-Barquero, Elena Vázquez Bourgon; Verona—Dr. Francesco Amaddeo, Dr. Giulia Bisoffi, Dr. Doriana Cristofalo, Dr. Rosa Dall’Agnola, Dr. Antonio Lasalvia, Dr. Mirella Ruggeri, Professor Michele Tansella.
We would also like to acknowledge the sustained and valuable assistance of the users, carers and clinical staff of the services in the five study sites. Reinhold Kilian provided helpful comments and suggestions on an earlier version of this paper. This study was supported by the European Commission BIOMED 2 Programme (Contract BMH4-CT95-1151). In Santander the EPSILON Project was partially supported by the Spanish Institute of Health (FIS Exp. 97/1240). Additional funding for studying patterns of care and costs of a cohort of patients with schizophrenia were provided by the Regione del Veneto, Giunta Regionale, Ricerca Sanitaria Finalizzata (Grant no. 723/01/96 to Professor M. Tansella).
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article
Cite this article
Becker, T., Leese, M., Krumm, S. et al. Needs and quality of life among patients with schizophrenia in five European centres. Soc Psychiat Epidemiol 40, 628–634 (2005). https://doi.org/10.1007/s00127-005-0937-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-005-0937-7