
Abstract
Aims/hypothesis
Liraglutide can modulate insulin secretion by directly stimulating beta cells or indirectly through weight loss and enhanced insulin sensitivity. Recently, we showed that liraglutide treatment in overweight individuals with prediabetes (impaired fasting glucose and/or impaired glucose tolerance) led to greater weight loss (−7.7% vs −3.9%) and improvement in insulin resistance compared with placebo. The current study evaluates the effects on beta cell function of weight loss augmented by liraglutide compared with weight loss alone.
Methods
This was a parallel, randomised study conducted in a single academic centre. Both participants and study administrators were blinded to treatment assignment. Individuals who were 40–70 years old, overweight (BMI 27–40 kg/m2) and with prediabetes were randomised (via a computerised system) to receive liraglutide (n = 35) or matching placebo (n = 33), and 49 participants were analysed. All were instructed to follow an energy-restricted diet. Primary outcome was insulin secretory function, which was evaluated in response to graded infusions of glucose and day-long mixed meals.
Results
Liraglutide treatment (n = 24) significantly (p ≤ 0.03) increased the insulin secretion rate (% mean change [95% CI]; 21% [12, 31] vs −4% [−11, 3]) and pancreatic beta cell sensitivity to intravenous glucose (229% [161, 276] vs −0.5% (−15, 14]), and decreased insulin clearance rate (−3.5% [−11, 4] vs 8.2 [0.2, 16]) as compared with placebo (n = 25). The liraglutide-treated group also had significantly (p ≤ 0.03) lower day-long glucose (−8.2% [−11, −6] vs −0.1 [−3, 2]) and NEFA concentrations (−14 [−20, −8] vs −2.1 [−10, 6]) following mixed meals, whereas day-long insulin concentrations did not significantly differ as compared with placebo. In a multivariate regression analysis, weight loss was associated with a decrease in insulin secretion rate and day-long glucose and insulin concentrations in the placebo group (p ≤ 0.05), but there was no association with weight loss in the liraglutide group. The most common side effect of liraglutide was nausea.
Conclusions/interpretation
A direct stimulatory effect on beta cell function was the predominant change in liraglutide-augmented weight loss. These changes appear to be independent of weight loss.
Trial registration
ClinicalTrials.gov NCT01784965
Funding
The study was funded by the ADA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Glucagon-like peptide 1 (GLP-1) receptor agonists are currently approved for the treatment of type 2 diabetes. In addition to improving glucose tolerance, this class of drugs enhances satiety and weight loss. As a result, there is growing interest in broadening the target population for these drugs to include individuals with prediabetes (impaired fasting glucose [IFG] and/or impaired glucose tolerance [IGT]) [1]. Modest weight loss is well known to reduce the risk of future diabetes in individuals with prediabetes [2–5]. Although mechanisms are not completely understood, weight loss leads to improvement in insulin resistance [6], which can reduce insulin secretory demands [7], and potentially ameliorate gluco- and lipotoxic effects on pancreatic beta cells [8]. There is also evidence that GLP-1 receptor agonists act directly on pancreatic beta cells to stimulate insulin secretion. For example, similar to native GLP-1, short-term treatment with liraglutide, a GLP-1 derivative, has been shown to increase insulin response to intravenous glucose [9] and increase beta cell sensitivity to oral glucose [10] in patients with type 2 diabetes. Therefore, the effects of GLP-1 receptor agonists on insulin secretory function are not simple; these agents are capable of decreasing insulin secretion secondary to weight loss and enhanced insulin sensitivity, as well as acting directly on the beta cell to increase insulin secretion.
In view of the dichotomous effects of GLP-1 receptor agonists on insulin secretory function, it is not clear what the net effect would be when they are given to individuals with prediabetes. We recently showed that overweight/obese individuals randomised to receive liraglutide and an energy-restricted diet lost more weight, and had a greater improvement in insulin sensitivity than a placebo-treated group [11]. Consequently, both the indirect and direct effects of liraglutide on beta cell function should be operative in this situation. The goal of this study was to determine the combined effects of weight loss and liraglutide treatment on beta cell function in individuals with prediabetes and evaluate the relative impact of the indirect effect of weight loss and decreased insulin resistance vs the direct effect of the GLP-1 agonist.
Methods
Participants
Individuals were eligible for the study if they were 40–70 years of age, overweight or obese (BMI 27–40 kg/m2) and had prediabetes (fasting glucose 5.6–6.9 mmol/l and/or elevated 2 h glucose 7.8–11.0 mmol/l after a 75 g oral glucose challenge). Participants were otherwise healthy with no known cardiac, liver or kidney disease. Recruitment through online and print advertisements occurred from December 2009 to December 2012. The protocol was approved by the Stanford Institutional Review Board and informed consent was obtained from all participants. The results of studies on the effects of liraglutide treatment on weight and insulin resistance have been published [11].
Study design
This was a double-blind, randomised, placebo-controlled, parallel-group study. Participants were randomised to receive either liraglutide (n = 35) or matching placebo (n = 33) by block randomisation by sex and BMI (<31 vs ≥31 kg/m2) via a computerised randomisation system. Treatment was given by subcutaneous injection before breakfast and titrated weekly from 0.6 mg to 1.2 mg and then to 1.8 mg. Liraglutide or placebo injections were continued until all end-of-study testing was completed. Study medication was given before the mixed-meal tolerance test (MMTT) and after the insulin suppression test or graded-glucose infusion test (GGIT). Both participants and study administrators (physicians, nurses, dietitian and coordinators) were blinded to treatment assignment.
Weight-loss intervention
Study participants attended meetings with a research dietitian weekly for the first 4 weeks and then bimonthly. They were counselled to decrease total energy intake by 2,092 kJ (500 kcal) per day and to continue baseline physical activity. During the last 2 weeks of the study, participants were instructed to maintain their weight for 2 weeks before repeat testing.
Metabolic studies
Participants were studied in the Stanford Clinical and Translational Research Unit. They were instructed to fast for 12 h overnight before any testing.
OGTT
Diagnosis of prediabetes was confirmed using a standard 75 g OGTT. Individuals with normal glucose tolerance or with diabetes were excluded.
Insulin suppression test
An insulin suppression test was conducted to measure peripheral insulin resistance at baseline and after 14 weeks of intervention [12]. After an overnight fast, participants were given a 180 min infusion of octreotide (0.27 μg m−2 min−1), insulin (32 mU m−2 min−1) and glucose (267 mg m−2 min−1). Steady-state plasma glucose (SSPG) concentrations were measured during the last 30 min and represented the degree of insulin resistance.
GGIT
Pancreatic beta cell function was assessed during graded infusions of intravenous glucose. The glucose infusion rate was started at 1 mg kg−1 min−1 and increased every 40 min up to 8 mg kg−1 min−1 [13, 14]. Blood was drawn for measurement of glucose, insulin, C-peptide and NEFA at baseline and before each rate change. We calculated the AUC for glucose, insulin, C-peptide and NEFA using the trapezoidal method.
Plasma C-peptide concentrations were used to derive the insulin secretion rates, as previously described [15]. A dose–response relationship between glucose and insulin secretion rate was constructed. The change in insulin secretion rate per molar increase in plasma glucose (slope) during the GGIT represented the pancreatic beta cell sensitivity to glucose.
The metabolic clearance rate of insulin was estimated by calculating the ratio of the total production of insulin to the area under the peripheral insulin curve during the GGIT [13]. The metabolic clearance rate of insulin was adjusted for body surface area.
MMTT
Day-long glucose, insulin and NEFA concentrations were measured before and at hourly intervals after breakfast (20% of daily energy intake given at 08:00 hours) and lunch (40% of daily energy intake given at 12:00 hours). Each meal was composed of 15% protein, 43% carbohydrate and 42% fat.
Glucose was determined by the oxidase method (Analyzer 2; Beckman, Brea, CA, USA). Insulin and C-peptide concentrations were measured at Washington University (St Louis, MO, USA) using radioimmunoassay (Millipore, St Charles, MO, USA). The inter- and intra-assay coefficient of variation ranged between 4.7% and 9.7% for insulin and between 5.2% and 10.9% for C-peptide. NEFA were measured enzymatically with a NEFA C kit (Wako Chemicals, Richmond, VA, USA).
Statistical analysis
The primary outcomes of the study were change in weight and SSPG concentration; these results have been previously reported [11]. Sample size was based on a 20% difference in SSPG concentration; the rationale has been previously reported [11]. Change in insulin secretion was a planned secondary outcome.
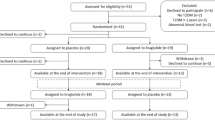
Originally, 68 individuals were randomised; 11 out of 35 individuals (31%) assigned to receive liraglutide dropped out of the study compared with 6 out of 33 (18%) assigned to receive placebo (p = 0.26) (see electronic supplementary material [ESM] Fig. 1). Reasons for dropping out and adverse effects have been previously reported [11]. The most common side effect of liraglutide treatment was nausea; two-thirds (67%) of participants receiving liraglutide experienced nausea compared with 26% on placebo (p = 0.005). Two individuals assigned to receive placebo did not have a GGIT at study end. Therefore, the final analyses included 24 individuals who received liraglutide and 25 individuals receiving placebo.
All statistical analyses were conducted using SPSS (version 21 for Windows; SPSS, Chicago, IL, USA). Differences between liraglutide and placebo groups were assessed using an independent t test or χ 2 test. Mean differences within groups were assessed using paired t tests. Regression analyses were performed to understand the relationship between weight loss and changes in pancreatic beta cell function and meal-associated profile in the two groups. The analyses were adjusted for age, sex and ethnicity. Results were not adjusted for multiple comparisons, and p < 0.05 was considered to indicate statistical significance.
Results
As seen in Table 1, individuals randomised to receive liraglutide and placebo had similar baseline characteristics including age (mean 58 years) and BMI (mean 31.9 kg/m2). In addition, the degree of hyperglycaemia was similar with no difference in fasting and 2 h glucose concentrations.
It has reported previously [11] that individuals treated with liraglutide lost approximately double the weight of individuals taking placebo (–7.7% vs −3.9%, p < 0.001). Weight loss was associated with significant improvement in insulin resistance in individuals treated with liraglutide as compared with placebo (change in SSPG, −27% vs 2.6%, p < 0.001). As seen in ESM Fig. 2, there was a significant direct association between percentage of weight lost and decrease in SSPG concentration in the entire study population (r = 0.36, p = 0.01). However, the distribution of weight loss differed between the liraglutide and placebo groups; 88% of individuals on liraglutide lost greater than 5% of baseline weight compared with 22% of those on placebo (p < 0.001). Therefore, there was little overlap in the degree of weight loss between the two groups.
Comparison of the changes in the responses to the GGIT between the two groups are presented in Table 2 and ESM Fig. 3. Treatment with placebo had no effect on the glucose rise in response to graded increases in intravenous glucose. In contrast, liraglutide treatment significantly attenuated the glucose rise. The insulin response significantly changed in both groups but in opposing directions; the insulin response modestly decreased in the placebo group by 7% whereas it increased in the liraglutide group by 34%. Placebo treatment had no effect on the C-peptide AUC whereas liraglutide treatment significantly increased the C-peptide AUC by 29%. Finally, placebo treatment had no effect on the NEFA AUC whereas liraglutide treatment enhanced the fall in NEFA concentration during the GGIT.
Figure 1 illustrates the dose–response relationship between plasma glucose and insulin secretion rate during the GGIT. Although there was no change with placebo treatment (Fig. 1a), there was a dramatic shift to the left in the dose–response curve following liraglutide treatment (Fig. 1b). The slope of the line plotting insulin secretion rate against glucose increased by 229% following liraglutide treatment (p < 0.001) whereas there was no significant change following placebo. Therefore, liraglutide significantly enhanced the glucose sensitivity of pancreatic beta cells.

Pancreatic beta cell sensitivity to glucose following weight loss before (black circles) and after (white circles) treatment with placebo (a) or liraglutide (b). Data are means ± SEM. Treatment with liraglutide, but not placebo, significantly increased beta cell sensitivity to glucose (slope) (p < 0.001)
Table 2 also presents the metabolic clearance rate of insulin calculated during the GGIT. Although there was no significant within-group difference in insulin clearance rate in either group, the insulin clearance tended to increase following placebo but decrease following liraglutide treatment, with a statistically significant difference between groups (p = 0.03).
Responses to eating two mixed meals are illustrated in Fig. 2 and summarised in Table 3. Fasting glucose concentration significantly declined after liraglutide treatment but not after placebo. However, there was no change in fasting plasma insulin concentration in either group. Day-long glucose concentrations also significantly decreased following treatment with liraglutide (Fig. 2b) but there was no change in those receiving placebo (Fig. 2a). In contrast to the increase in the insulin response following intravenous glucose, day-long insulin concentrations decreased modestly following liraglutide treatment (Fig. 2d), with no change seen in the placebo-treated group (Fig. 2c). However, the difference between the two groups was not significant (p = 0.46; Table 3). Finally, day-long NEFA concentrations decreased following liraglutide treatment (Fig. 2f) but they did not change in the placebo-treated group.

Response to mixed meals following weight loss before (black circles) and after (white circles) treatment with placebo (a, c, e) or liraglutide treatment (b, d, f). Meals were given at 08:00 hours and 12:00 hours. Data are means ± SEM. Liraglutide treatment was associated with decrease in the AUC for glucose (p < 0.001), insulin (p = 0.03) and NEFA (p < 0.001); there was no significant change following treatment with placebo
Regression analyses were performed in an effort to obtain information as to the effect of weight loss, per se, on changes in pancreatic beta cell function and meal-associated profile in the placebo and liraglutide groups individually. As seen in Table 4, in the placebo group, weight loss was associated with a significant decline in insulin secretion rate during the GGIT and decline in day-long glucose and insulin concentrations during the meal tolerance test. In contrast, weight loss was not associated with any changes in the liraglutide group. Weight loss was not associated with changes in NEFA AUC in either group. Changes in NEFA AUC were also not predicted by changes in insulin resistance (SSPG) or insulin AUC during the MMTT in a regression analysis adjusted for age, sex and ethnicity (data not shown).
Finally, as the study population included different prediabetes subgroups (IFG, IGT and IFG/IGT), we evaluated whether the changes associated with treatment assignment varied with these subgroups. As seen in ESM Table 1, differences between placebo and liraglutide groups remained regardless of whether individuals had IFG or IFG/IGT (no comparisons were made using data from the individuals with isolated IGT due to small sample size).
Discussion
Very few studies have evaluated the effect of GLP-1 receptor agonists in individuals without diabetes [11, 16–18], and we are unaware of any that have evaluated changes in beta cell function after treatment with a GLP-1 derivative in individuals with prediabetes. In our previous work [11] we demonstrated that treatment with liraglutide can augment weight loss and improve insulin resistance in a population of older, overweight individuals with prediabetes. In the current study we have evaluated the combined effects of weight loss and GLP-1 stimulation on pancreatic beta cell function. For reasons to be discussed below, we believe the changes we observed represent primarily a direct stimulatory effect of liraglutide on insulin secretion, rather than being the expected consequences of weight loss and enhanced insulin sensitivity.
One of the benefits of treatment with a GLP-1 receptor agonist is its potential to enhance weight loss. Weight loss is an important treatment goal for patients with prediabetes [19, 20] and has been shown in several clinical trials to decrease risk for future diabetes [2–5]. Although the mechanisms are not fully understood, weight loss improves insulin resistance [6] and reduces insulin secretory demands [7]. In the current study, despite greater weight loss and improvement in insulin resistance in the liraglutide group, the insulin secretion rate significantly increased (Fig. 1). In addition, although degree of weight loss significantly predicted fall in insulin secretion rate and day-long insulin concentration in the placebo group, there was no association between weight loss and changes in insulin secretion rate or concentration in the liraglutide group (Table 4). Thus, the changes following liraglutide treatment are not those that occur following weight loss and enhanced insulin sensitivity, but rather similar to effects seen after acute infusion of GLP-1 [21].
Liraglutide treatment had less dramatic effects on glucose and insulin responses to mixed meals than it did on the responses to the intravenous glucose infusion. The effect of liraglutide treatment on insulin secretion rate is easier to discern following intravenous glucose than mixed meals. During a GGIT, the glucose rate is controlled and continually increases whereas the glucose intake following mixed meals can depend on more than the carbohydrate content of the meal (e.g. macronutrient composition of the meal, rate of glucose absorption from the gut). Therefore, the GGIT is ideally suited to evaluate the relationship between rising glucose concentration and insulin secretion rate (or pancreatic beta cell function). Based on the GGIT results, the modest decrease in day-long insulin concentration following mixed meals seems paradoxical. Although the reasons for this discrepancy are unclear, even treatment with a sulfonylurea compound, a known insulin secretagogue, does not necessary lead to a sustained increase in insulin concentration after glucose ingestion due to a concomitant fall in plasma glucose concentration [22]. Mari and associates observed a decrease in day-long plasma glucose concentrations, without any change in insulin concentrations, following mixed meals in patients with type 2 diabetes treated with liraglutide for 1 week [10]. Using modelling analysis, the authors suggested that these changes reflected an increase in pancreatic beta cell sensitivity to glucose. In the current study, in addition to the decrease in day-long glucose concentrations, the day-long insulin concentrations modestly decreased following liraglutide treatment, although the levels were not different from those in the placebo group. In addition, the study population and study protocol differed with longer duration of liraglutide treatment and a weight-loss intervention. Therefore, it is unclear whether the results following MMTT, as opposed to the GGIT, reflect changes in pancreatic beta cell function.
As the placebo group lost less weight than the liraglutide group, the impact of comparable degrees of weight loss with and without liraglutide remains unclear. We have, however, previously shown similar degree of improvement in insulin resistance following rosiglitazone treatment in an overweight, non-diabetic group with insulin resistance [13]. Using similar metabolic studies as in this study, we showed that treatment with rosiglitazone for 12 weeks decreased SSPG concentration by 27% and reduced day-long glucose response following two mixed meals by 9%. Thus, the improvement in insulin resistance and glucose concentrations were similar to the current results following liraglutide treatment. On the other hand, the resultant changes in insulin metabolism were quite different. For example, rosiglitazone led to a shift to the right of the insulin secretion rate dose–response curve with a fall in insulin secretion rate and an increase in insulin clearance rate. In contrast, as seen in Fig. 1, liraglutide treatment led to a dramatic left shift in the insulin secretion rate dose–response curve and a decrease in insulin clearance rate. In addition, rosiglitazone treatment led to a 41% decline in day-long insulin response to mixed meals compared with the 8% decrease seen with liraglutide treatment. Although not conclusive, this comparison suggests that the direct GLP-1 action may play a greater role in changing beta cell function after liraglutide treatment than weight loss or improvement in insulin resistance.
Although the opposite changes are seen after weight loss alone or drug-enhanced insulin sensitivity, the effects of liraglutide treatment on pancreatic beta cell function may be beneficial. Individuals with prediabetes, similar to those with type 2 diabetes, are known to have altered pancreatic beta cell glucose sensitivity [23]. As seen in Fig. 1, treatment with liraglutide may restore beta cell sensitivity towards normal and improve insulin secretory response. Indeed, the mean fasting glucose level in individuals became normal (< 5.6 mmol/l) after liraglutide treatment and integrated day-long glucose concentration in response to mixed meals declined by 8.2%. Although difficult to compare with other studies, the decline in fasting glucose was greater than has been reported during moderate weight loss in the prediabetes population [3, 5]. Ability to normalise glucose, regardless of mechanism, may have an independent effect on decreasing the risk for type 2 diabetes in individuals with prediabetes [24]. Therefore, direct GLP-1 action on beta cells may offer additional benefits to weight loss.
NEFA levels also decreased after liraglutide treatment in response to both intravenous glucose and mixed meals. Although weight loss and improvement in insulin resistance may mediate the decrease, a moderate weight loss of 5–10% generally does not lower day-long NEFA concentrations due to a concomitant decrease in day-long insulin concentrations in response to mixed meals [25, 26]. In support, weight loss was not associated with a decrease in NEFA in either the placebo or the liraglutide group (Table 4). Previous studies have shown that an acute infusion of GLP-1 [27], or single injection of exenatide [28], another GLP-1 receptor agonist, lowers NEFA concentrations following mixed meals. Although the mechanisms involved are not entirely clear, the changes in NEFA concentrations seen after liraglutide treatment are not likely to be due to weight loss or improvement in insulin resistance.
Although we studied a relatively small population, we are unaware of published reports evaluating changes in pancreatic beta cell function and day-long insulin concentrations following liraglutide-augmented weight loss in a prediabetic population. The results clearly demonstrate that liraglutide has direct GLP-1 actions on pancreatic beta cell function and this counterbalances effects seen after weight loss alone. Future studies are needed to determine whether the ability of GLP-1 receptor agonists to directly stimulate insulin secretion in patients with prediabetes will be more, or less, beneficial compared with weight loss alone.
Abbreviations
- GGIT:
-
Graded-glucose infusion test
- GLP-1:
-
Glucagon-like peptide 1
- IFG:
-
Impaired fasting glucose
- IGT:
-
Impaired glucose tolerance
- MMTT:
-
Mixed-meal tolerance test
- SSPG:
-
Steady-state plasma glucose
References
Holst JJ, Deacon CF (2013) Is there a place for incretin therapies in obesity and prediabetes? Trends Endocrinol Metab 24:145–152
Knowler WC, Barrett-Connor E, Fowler SE et al (2002) Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346:393–403
Tuomilehto J, Lindstrom J, Eriksson JG et al (2001) Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 344:1343–1350
Pan XR, Li GW, Hu YH et al (1997) Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care 20:537–544
Saito T, Watanabe M, Nishida J et al (2011) Lifestyle modification and prevention of type 2 diabetes in overweight Japanese with impaired fasting glucose levels: a randomized controlled trial. Arch Intern Med 171:1352–1360
McLaughlin T, Carter S, Lamendola C et al (2006) Effects of moderate variations in macronutrient composition on weight loss and reduction in cardiovascular disease risk in obese, insulin-resistant adults. Am J Clin Nutr 84:813–821
Utzschneider KM, Carr DB, Barsness SM, Kahn SE, Schwartz RS (2004) Diet-induced weight loss is associated with an improvement in beta-cell function in older men. J Clin Endocrinol Metab 89:2704–2710
Hanley AJ, Zinman B, Sheridan P, Yusuf S, Gerstein HC, Investigators DRAWRaRMD (2010) Effect of Rosiglitazone and Ramipril on β-cell function in people with impaired glucose tolerance or impaired fasting glucose: the DREAM trial. Diabetes Care 33:608–613
Degn KB, Juhl CB, Sturis J et al (2004) One week’s treatment with the long-acting glucagon-like peptide 1 derivative liraglutide (NN2211) markedly improves 24-h glycemia and alpha- and beta-cell function and reduces endogenous glucose release in patients with type 2 diabetes. Diabetes 53:1187–1194
Mari A, Degn K, Brock B, Rungby J, Ferrannini E, Schmitz O (2007) Effects of the long-acting human glucagon-like peptide-1 analog liraglutide on beta-cell function in normal living conditions. Diabetes Care 30:2032–2033
Kim SH, Abbasi F, Lamendola C et al (2013) Benefits of liraglutide treatment in overweight and obese older individuals with prediabetes. Diabetes Care 36:3276–3282
Greenfield MS, Doberne L, Kraemer F, Tobey T, Reaven G (1981) Assessment of insulin resistance with the insulin suppression test and the euglycemic clamp. Diabetes 30:387–392
Kim SH, Abbasi F, Chu JW et al (2005) Rosiglitazone reduces glucose-stimulated insulin secretion rate and increases insulin clearance in nondiabetic, insulin-resistant individuals. Diabetes 54:2447–2452
Jones CN, Pei D, Staris P, Polonsky KS, Chen YD, Reaven GM (1997) Alterations in the glucose-stimulated insulin secretory dose-response curve and in insulin clearance in nondiabetic insulin-resistant individuals. J Clin Endocrinol Metab 82:1834–1838
Van Cauter E, Mestrez F, Sturis J, Polonsky KS (1992) Estimation of insulin secretion rates from C-peptide levels. Comparison of individual and standard kinetic parameters for C-peptide clearance. Diabetes 41:368–377
Astrup A, Rössner S, Van Gaal L et al (2009) Effects of liraglutide in the treatment of obesity: a randomised, double-blind, placebo-controlled study. Lancet 374:1606–1616
Rosenstock J, Klaff LJ, Schwartz S et al (2010) Effects of exenatide and lifestyle modification on body weight and glucose tolerance in obese subjects with and without pre-diabetes. Diabetes Care 33:1173–1175
Elkind-Hirsch K, Marrioneaux O, Bhushan M, Vernor D, Bhushan R (2008) Comparison of single and combined treatment with exenatide and metformin on menstrual cyclicity in overweight women with polycystic ovary syndrome. J Clin Endocrinol Metab 93:2670–2678
Nathan DM, Davidson MB, DeFronzo RA et al (2007) Impaired fasting glucose and impaired glucose tolerance: implications for care. Diabetes Care 30:753–759
American Diabetes Association (2013) Standards of medical care in diabetes–2013. Diabetes Care 36(Suppl 1):S11–S66
Kjems LL, Holst JJ, Vølund A, Madsbad S (2003) The influence of GLP-1 on glucose-stimulated insulin secretion: effects on beta-cell sensitivity in type 2 and nondiabetic subjects. Diabetes 52:380–386
Reaven G, Dray J (1967) Effect of chlorpropamide on serum glucose and immunoreactive insulin concentrations in patients with maturity-onset diabetes mellitus. Diabetes 16:487–492
Gumbiner B, Van Cauter E, Beltz WF et al (1996) Abnormalities of insulin pulsatility and glucose oscillations during meals in obese noninsulin-dependent diabetic patients: effects of weight reduction. J Clin Endocrinol Metab 81:2061–2068
Perreault L, Pan Q, Mather KJ et al (2012) Effect of regression from prediabetes to normal glucose regulation on long-term reduction in diabetes risk: results from the Diabetes Prevention Program Outcomes Study. Lancet 379:2243–2251
McLaughlin T, Abbasi F, Lamendola C, Kim HS, Reaven GM (2001) Metabolic changes following sibutramine-assisted weight loss in obese individuals: role of plasma free fatty acids in the insulin resistance of obesity. Metabolism 50:819–824
Abbasi F, Chen YD, Farin HM, Lamendola C, Reaven GM (2008) Comparison of three treatment approaches to decreasing cardiovascular disease risk in nondiabetic insulin-resistant dyslipidemic subjects. Am J Cardiol 102:64–69
Meier JJ, Gethmann A, Götze O et al (2006) Glucagon-like peptide 1 abolishes the postprandial rise in triglyceride concentrations and lowers levels of non-esterified fatty acids in humans. Diabetologia 49:452–458
Schwartz EA, Koska J, Mullin MP, Syoufi I, Schwenke DC, Reaven PD (2010) Exenatide suppresses postprandial elevations in lipids and lipoproteins in individuals with impaired glucose tolerance and recent onset type 2 diabetes mellitus. Atherosclerosis 212:217–222
Acknowledgements
The authors thank P. Schaaf, the research dietitian, and the staff and nurses in the Stanford Clinical and Translational Research centre for their invaluable assistance with the study.
Funding
The study was funded by the ADA (7-09-NOVO-15 to GR). Liraglutide and matching placebo were provided by Novo Nordisk. The ADA and Novo Nordisk were not involved in the design or conduct of the study, the collection, management, analysis and interpretation of the data or the preparation, review or approval of the manuscript.
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
SHK and GR conceptualised and designed the study and interpreted the analyses. SHK performed data analysis and drafted the manuscript. GR revised the manuscript for critical intellectual content. AL, DA, FA, CL, KG and VT helped acquire the data and edited the manuscript. All authors approved the final version of the manuscript. SHK is the guarantor of this work and, as such, had full access to all of the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM Fig. 1
(PDF 7 kb)
ESM Fig. 2
(PDF 25 kb)
ESM Fig. 3
(PDF 91 kb)
ESM Table 1
(PDF 15 kb)
Rights and permissions
About this article
Cite this article
Kim, S.H., Liu, A., Ariel, D. et al. Pancreatic beta cell function following liraglutide-augmented weight loss in individuals with prediabetes: analysis of a randomised, placebo-controlled study. Diabetologia 57, 455–462 (2014). https://doi.org/10.1007/s00125-013-3134-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-013-3134-3