
Abstract
Aims/hypothesis
This study aimed to systematically review what has been reported on the incidence and prevalence of type 2 diabetes in children and adolescents, to scrutinise the methodological issues observed in the included studies and to prepare recommendations for future research and surveillances.
Methods
PubMed, the Cochrane Database of Systematic Reviews, Scopus, EMBASE and Web of Science were searched from inception to February 2013. Population-based studies on incidence and prevalence of type 2 diabetes in children and adolescents were summarised and methodologically evaluated. Owing to substantial methodological heterogeneity and considerable differences in study populations a quantitative meta-analysis was not performed.
Results
Among 145 potentially relevant studies, 37 population-based studies met the inclusion criteria. Variations in the incidence and prevalence rates of type 2 diabetes in children and adolescents were mainly related to age of the study population, calendar time, geographical regions and ethnicity, resulting in a range of 0–330 per 100,000 person-years for incidence rates, and 0–5,300 per 100,000 population for prevalence rates. Furthermore, a substantial variation in the methodological characteristics was observed for response rates (60–96%), ascertainment rates (53–99%), diagnostic tests and criteria used to diagnose type 2 diabetes.
Conclusions/interpretation
Worldwide incidence and prevalence of type 2 diabetes in children and adolescents vary substantially among countries, age categories and ethnic groups and this can be explained by variations in population characteristics and methodological dissimilarities between studies.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Global prevalence of diabetes is increasing rapidly [1]. With an estimated 285 million patients (aged 20–79 years) in 2010, diabetes is becoming one of the main threats to human health in the 21st century in both developed and developing countries [1, 2]. Globally, type 2 diabetes accounts for more than 90% of the cases of diabetes [2]. Until recently, type 2 diabetes was barely diagnosed in children, since it was considered to be a disease of adulthood. Over the past two decades, an increase in prevalence of type 2 diabetes in children and adolescents has been reported in several countries [1, 3]. Early onset of type 2 diabetes is associated with increased risk of morbidity and mortality [4, 5]. Type 2 diabetes has a disrupting effect on young individuals during their most productive years and leads to increased healthcare costs. In addition, (severe) complications of type 2 diabetes, such as nephropathy, retinopathy, neuropathy, dyslipidaemia and cardiovascular disease are an ongoing threat [4–7].
An overview of global trends in the incidence and prevalence of type 2 diabetes in children and adolescents is important, since type 2 diabetes has significant effects on health and quality of life, use of medical services and reduced employability resulting in a huge economic burden [6–9]. To support appropriate healthcare policies, population-based epidemiological studies are required to show the actual burden of the disease and its secular trends [7]. We have performed a systematic search to detect systematic reviews or meta-analyses summarising the existing data on incidence and prevalence of type 2 diabetes in young age groups and the different methodologies used to estimate these population data. However, such studies have not been published. Therefore, the aims of our study are to review what is known about the incidence and prevalence of type 2 diabetes in children and adolescents, to scrutinise the methodological issues observed in the included studies and to prepare recommendations for future research and surveillances.
Methods
Data sources and searches
This systematic review follows the guidelines of ‘Meta-analysis of Observational Studies in Epidemiology (MOOSE)’ [10]. After defining the research question and consulting a medical librarian in the library of Utrecht University, a search was performed in PubMed, the Cochrane Database of Systematic Reviews, Scopus, EMBASE and Web of Science. Our search covered all publications in the above databases, from the inception of each database up to the third week of February 2013. The search terms and search strategy are listed in Table 1. All search results were imported to a Refworks file (www.refworks.com).
Study selection
After removing duplicates, the title and abstract of each article were screened by two of the authors (S. Fazeli Farsani and M. P. van der Aa) to exclude irrelevant studies. Articles were selected based on inclusion and exclusion criteria (Table 2). Reference lists of included articles were assessed to find additional articles. Full texts of all included articles were retrieved via the library of Utrecht University or through contact with the authors. Abstracts of conferences were not included in this review. Studies were excluded based on title and abstract if they were not population-based (e.g. studies were performed in specific populations like obese children and adolescents) or if they described prevalence or incidence of concurrent diseases in patients with type 2 diabetes.
Full text screening was performed when it was not clear whether the study population involved children and adolescents, or when the abstract was unclear about the type of diabetes. In case of disagreement the study was checked by a third author (A. de Boer or M. M. J. van der Vorst).
Data extraction and quality assessment
Once consensus on the included articles was achieved, data was extracted from the full text articles. The following data—author, country of the study, calendar time, study design and denominator used, diagnostic criteria, characteristics of the study population (age, sex and ethnicity), excluded cases, incidence (per 100,000 person-years) and prevalence (per 100,000 population)—were separately extracted, entered into a table by two of the authors (S. Fazeli Farsani and M. P. van der Aa) and then compared for similarity (see Table 3 and electronic supplementary material [ESM] Table 1).
Data synthesis and analysis
Two authors (S. Fazeli Farsani and M. P. van der Aa) checked the extracted data. For the methodological evaluation the following aspects were assessed: response rates of population-based screening studies (the percentage of the invited population that consented to participate), ascertainment rate of studies in which children diagnosed by doctors were captured (the percentage of children with type 2 diabetes identified and registered by healthcare providers of all diagnosed children with type 2 diabetes), the performed diagnostic tests (e.g. measurement of glucose concentration in urine or in plasma), diagnostic guidelines, classification and differentiation between type 1 and 2 diabetes, quality of denominators used to calculate incidence and prevalence rates, sample size of the population on which the rate estimates were based and representativeness of the evaluated population for the whole population in the defined geographic area.
Due to substantial methodological heterogeneity and considerable variations in study populations a quantitative meta-analysis of the data was not performed.
Results
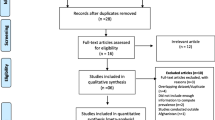
The search of the five electronic databases yielded 5,920 articles, of which 145 were potentially relevant after screening title and abstract. Out of these papers, 37 articles met the inclusion criteria. Manual reference screening did not result in additional articles (Fig. 1). All included articles were written in English. Of the total of 37 included articles, 12 described prevalence studies, 16 described incidence studies and 9 contained both incidence and prevalence data. As shown in Table 3, the included studies originated from four continents (13 different countries). Most of the studies were conducted in the USA and North European countries, while there were no studies from African or South American countries or from a major part of Asia. Three Japanese [11–13], two Austrian [14, 15] and two American studies [16, 17] were based on the same data source, albeit the data were analysed differently and comprised other study periods. There was a substantial variation in population characteristics and methodological aspects in the identified studies (Table 3), as described below.

Flowchart of search results. DSR, Database of Systematic Reviews
Study population and ethnicities
The number of children in the populations in which type 2 diabetes was detected ranged from 1,647 [18] to several millions [11–13, 19–25] and covered different age categories. The 37 included studies described data about many different ethnicities—Japanese, Taiwanese, multi-ethnic, New Zealand-Maori, New Zealand-European, Turkish, South Asian, Black, Aboriginal, African-American, American Indian, Pima Indian, Ojibwa-Cree, non-Hispanic whites, Hispanic, etc. (ESM Table 1).
Calendar time and duration of the study
Calendar time of the 37 studies varied widely. The first population-based study that reported on the epidemiology of type 2 diabetes in children and adolescents was started in 1965 in Pima Indians in the USA [17], while the most recent study was a Canadian study performed between 2006 and 2008 [26]. Pavkov et al reported the longest follow-up of 39 years [17], followed by a Japanese study with a follow-up of 30 years [11–13]. The shortest follow-up was 1 year [27–30].
Study design and case ascertainment methods
Different methods were used in the studies for investigating incidence and prevalence of type 2 diabetes. In nine studies, cases of type 2 diabetes were found through population screening [11–13, 16–18, 31–33]. The population that was invited for screening also varied between studies. The complete Pima Indian population was screened regardless of their health situation [16, 17], in Japan and Taiwan school children from all schools were screened [11–13, 31, 32] and in Ankara (Turkey) only children in six randomly selected schools participated in the screening programme [18]. In a Canadian study, all school children (aged 4–19 years) in the remote northern Ojibwa-Cree community of St Theresa Point First Nation were screened [33].
The second method, which was the one most commonly applied (in 20 studies), was to capture all cases of type 2 diabetes in children and adolescents that had been diagnosed by the healthcare provider. In these 20 studies, healthcare providers with different backgrounds (e.g. general practitioners, paediatric endocrinologists, adult endocrinologists, diabetes nurses, etc.) participated in a surveillance system [14, 15, 19–28, 30, 34–40]. The numbers of diagnosed cases were related to denominators of numbers of children in the relevant geographical areas (Table 3).
A third method, applied in six studies, involved the use of administrative databases (e.g. using prescriptions for glucose-lowering treatment listed in a database as a proxy for finding cases of diabetes [41]) or medical chart reviews in hospitals or medical centres [29, 42–45].
Two of the included studies (Fagot-Campagna et al and Craig et al) used a combination of methods for identifying cases of type 2 diabetes [7, 46]. Fagot-Campagna et al used both population screening and medical chart reviews while Craig et al used administrative databases and a surveillance system to find cases of type 2 diabetes.
In the population-based screening studies, when reported, response rates varied from 60% to 96%. In the studies that used healthcare provider diagnosis or administrative databases, case ascertainment ranged from 53% to 99% (Table 3).
Diagnosis of type 2 diabetes and classification
Another source of variation in the methodology of the included studies was the use of different diagnostic guidelines for type 2 diabetes. In most studies, the ADA or WHO guidelines were used to identify cases. In a few studies, national guidelines were used to diagnose type 2 diabetes [26, 37, 38].
Different diagnostic tests were used to identify type 2 diabetes cases (e.g. in two screening programmes, urine strips were used to diagnose glycosuria and children with two positive results were checked with additional diagnostic tests) [11–13, 31, 32]. In most studies diabetes was diagnosed based on clinical presentation in combination with diagnostic tests (e.g. OGTT, fasting plasma glucose (FPG), fasting plasma insulin and/or C-peptide level, etc.). Classification of the type of diabetes was another major issue. Differentiation between type 2 and type 1 diabetes was difficult, especially in the earliest and retrospective studies and in studies in which questionnaires (or telephone surveys) were used. In the 37 included studies, different criteria were used to differentiate between type 1 and type 2 diabetes (Table 3) (e.g. 26 of the included studies reported that they used tests for detecting auto-antibodies or beta cell function [11–15, 19–27, 29–31, 34, 36, 39, 40, 42–46]).
In almost all studies, the healthcare providers or investigators confirmed the type of diabetes, except in two studies in which the type of diabetes was reported by parents or children themselves via questionnaire or telephone survey [32, 39].
Incidence and prevalence estimates
Data on incidence and prevalence from all studies are summarised in Figs 2 and 3. Incidence and prevalence rates were found to vary widely depending on age, sex and ethnicity of the study population and geographical region, resulting in a range of 0–330 per 100,000 person-years for incidence and 0–5,300 per 100,000 children and adolescents for prevalence [7, 17, 18, 37]. Detailed information from all studies is presented in ESM Table 1.

Overview of the reported incidences of type 2 diabetes per 100,000 person-years (because of considerable variations in the observed rates, incidence data are graphed on a base 10 logarithmic scale). The incidence rates were calculated for male/female populations. White bars represent children (0–9 years), grey bars represent adolescents (10–19 years) and black bars represent children and adolescents (0–19 years)

Overview of the reported prevalences of type 2 diabetes per 100,000 children and/or adolescents (because of considerable variations in the observed rates, prevalence data are graphed on a base 10 logarithmic scale). The prevalence rates were calculated for male/female populations, except for the prevalence rate of 3,600 per 100,000 which was for Ojibwa-Cree females. White bars represent children (0–9 years), grey bars represent adolescents (10–19 years) and black bars represent children and adolescents (0–19 years)
The lowest incidence rates were observed in European countries. The Netherlands, with no new cases of type 2 diabetes during the 1998–2000 period, and Austria, with an incidence rate of 0.29 per 100,000 person-years for the 1999–2007 period, had the lowest reported incidences [14, 15, 37].
The highest incidence of type 2 diabetes in youth was observed in 4- to 15-year-old Pima Indians in the USA (330 per 100,000 person-years) [17]. This was followed by the Navajo population (USA), American Indians (USA) and African-Americans (USA) (27.7, 23.3 and 19, respectively, per 100,000 person-years) [20, 23, 44]. The Aboriginal population in Canada also had a high incidence rate (23.3 per 100,000 person-years) [26] (Fig. 2).
Among European countries, a study from the UK showed incidence rates of type 2 diabetes stratified by ethnicity: black individuals had 3.9 cases per 100,000 person-years, while South Asian and white individuals had rates of 1.25 and 0.35 per 100,000 person-years, respectively [30].
In Europe, the UK had the highest number of prevalence studies [27–29, 41]. Of four prevalence studies in the UK, two covered the whole country but produced different results. In one study, the prevalence for the population 0–16 years of age in 2000 was reported to be 0.21 per 100,000 children/adolescents, while in another study in the same year the reported prevalence rate was 1.9 per 100,000 for the 0- to 18-year-old study population [27, 41]. Among the European countries, the highest prevalence rate of type 2 diabetes was reported in 15- to 19-year-old adolescents in Leeds (UK) with a prevalence of 9 per 100,000 adolescents in 2000 [29].
The highest prevalence of type 2 diabetes in youth was observed in female Pima Indians (USA) aged 15–19 years (5,300 per 100,000 in 1987–1996), while for male Pima Indians the rate was lower (3,800 per 100,000) [16, 17]. For 10- to 14-year-old Pima Indians in the same time period, the respective prevalence for female and male subjects was 2,900 and 1,400 per 100,000 [7]. The Ojibwa-Cree population in Canada had the second highest prevalence rate with 3,600 per 100,000 for 10- to 19-year old females and 1,100 per 100,000 for 4- to 19-year-old male and female children and adolescents in 1996–1997 [33] (Fig. 3). High prevalence rates were also reported in American Indians, Navajo population and African-American children and adolescents [20, 23–25]. Among the different ethnicities in the USA, non-Hispanic white individuals had the lowest prevalence of type 2 diabetes [24, 25] (ESM Table 1).
Discussion
According to the findings of this systematic review, the epidemiological studies of type 2 diabetes in children and adolescents differed widely in population characteristics and study methods, which resulted in a substantial variation in incidence and prevalence estimates. While these differences in the rates of type 2 diabetes could in part be explained by differences in age, ethnicity, country and calendar time, methodological dissimilarities contributed as well. Referring to two studies performed in the UK in 2000, Hsia et al reported a prevalence rate for type 2 diabetes which was almost ten times higher than that reported by Ehtisham et al [27, 41]. Although there was only a slight difference in age between the two study populations, the different methods used (Ehtisham et al used a survey to find cases of type 2 diabetes while Hsia et al used an administrative database) and the lower case ascertainment in the study by Ehtisham et al probably led to an underestimation of the type 2 diabetes cases. Another example of the impact of methodological differences on the rate estimates is the study of Fagot-Campagna et al, which compared the prevalence of type 2 diabetes in adolescents aged 15–19 years, obtained from two different sources using different methods of data collection and analysis. The prevalence estimate of 5.1% vs 0.46% shows the remarkable effect of methodological differences on rate estimation [7].
In most of the studies included in this review, cases of type 2 diabetes were reported by healthcare providers who participated in a surveillance system. There are several drawbacks of using this method to estimate the occurrence of type 2 diabetes. First, children and adolescents with type 2 diabetes may remain asymptomatic and undiagnosed for a long period of time [47, 48] leading to underestimation of the number of type 2 diabetes cases [14, 15, 19–27, 29, 30, 34, 37, 39, 43, 44, 46]. Although the Princeton study recently showed that undiagnosed type 2 diabetes is very uncommon in adolescents and that this has not changed over the last decades [49], the findings from the Princeton study probably cannot be extrapolated to countries in which patients have only limited access to healthcare and/or the healthcare system has a suboptimal quality. Second, the quality of detection and classification of type 2 diabetes might differ between healthcare providers [29, 32, 35, 36]. This may be related to the different backgrounds of the healthcare providers (e.g. general practitioners, paediatricians and endocrinologists have different test strategies) and also to the lack of an internationally agreed diagnostic method and classification system for identifying cases of type 2 diabetes in children and adolescents. Third, case ascertainment rates in surveillance systems showed substantial differences, again leading to different rates and underestimation of incidence and prevalence rates [27, 41].
Administrative databases (e.g. prescription databases) are sometimes used for incidence and prevalence estimation, with the advantage that this approach for some aspects is less susceptible to ascertainment and selection biases. For instance when a prescription record database of pharmacies is used, the registration of prescriptions is often similar and complete [50]. However, the problem of missing undiagnosed cases of type 2 diabetes and differences in testing and treatments of diabetes between healthcare providers remain important limitations [41].
Retrospectively reviewing the medical charts and patient files in medical centres to find cases of diabetes, and to classify them based on the retrieved data, is often suboptimal because of missing information and differences by which healthcare providers test for diabetes and record medical information [44].
For all three methods mentioned above (capturing of cases by participation of healthcare providers in surveillance systems, administrative databases and reviewing of medical charts) an important difficulty is that of retrieving a valid denominator. Often the denominator originates from organisations registering vital statistics. A valid demarcation of the area from which the cases derive is a challenge.
Although population-based screening was not often applied among our 37 studies, it has a number of important advantages when compared with the other methods discussed. The starting point is that all people, regardless of their health situation, are screened and the same valid screening method and diagnostic criteria can be used. Thereby, the chance of finding all (and even asymptomatic undiagnosed) type 2 diabetes cases will increase. Furthermore, the denominator is directly available, being the total number of screened children and adolescents. However, in these population-based screening programmes some important issues should also be taken into account. For instance, non-participation of invited children (suboptimal response rate) can lead to biased estimations. Also, just as in the other methods, the sensitivity and specificity of the diagnostic tests, with the potential risks of under- or over-diagnosis, respectively, can be a problem. Wei et al reported that the sensitivity of the glycosuria test used in the screening for diabetes ranged from 20% to more than 80% [32]. Finally, the performance of a population-based screening is probably more costly than the other methods. As far as we know the different methods have not been compared with respect to cost-effectiveness. Recently Wu et al conducted a cost-effectiveness analysis of screening strategies for identifying type 2 diabetes and dysglycaemia (prediabetes) in children and adolescents (aged 10–17 years) [51]. Although they found that the cost of screening per case was high for diabetes, they mentioned that screening for diabetes in youth could be more cost-effective if dysglycaemia was explicitly considered as a screening outcome. However, Wu et al did not address the benefits and harms of early detection of type 2 diabetes and prediabetes in children and adolescents.
Even if case ascertainment, classification and definition of type 2 diabetes and response rates are satisfactory, the researchers involved in all methods face the challenge of choosing the right sample(s) of the population to be really representative for the intended population [7]. Regional differences may be expected in vital statistics, reflecting geographical, ethnic, genetic, environmental and socioeconomic factors. For this reason, the demographic characteristics of the population sample should be well described and the analysis should take into account such differences.
After considering all methodological differences, we can state in general that ethnic minorities have higher rates of type 2 diabetes than white individuals in almost all countries. There is also a great difference among type 2 diabetes rates in ethnic minorities in the USA and Canada compared with ethnic groups in other locations (e.g. in Europe and Australia) [19–27, 30, 34, 46]. Although genetics plays an important role in the development of diabetes, environmental and lifestyle factors, such as dietary habits and having a sedentary lifestyle, are also relevant. For instance, Pima Indians in Arizona have the highest reported prevalence of type 2 diabetes in the world [7] while Pima Indians in Mexico with the same ethnicity have a much lower prevalence [7]. Pima Indians in Mexico have a healthier and more active lifestyle than Arizona Pima Indians, which indicates the importance of environmental factors in the development of type 2 diabetes [7].
Both incidence and prevalence data were considerably higher in female vs male subjects and, in addition, there was a great difference between adolescents (aged 10–19 years) and children (aged 0–9 years) [24, 25].
Concerning changes in the occurrence of type 2 diabetes over time, existing data are limited for most countries. Only a few studies (e.g. Urakami et al in Japan and Pavkov et al in the USA) evaluated trends in incidence/prevalence of type 2 diabetes over a prolonged period of time [11–13, 17]. Pavkov’s study demonstrated a significant increase in type 2 diabetes rates while the Japanese study showed a decrease in incidence of type 2 diabetes in Japanese school children [11–13, 17].
The lack of studies performed in some parts of the world, mostly developing countries, and the absence of data on the socioeconomic status of the study populations are limitations of our review. In addition, the heterogeneity of study designs and population characteristics did not allow for a more rigorous quantitative analysis (such as a meta-analysis).
In conclusion, the incidence and prevalence of type 2 diabetes in children and adolescents show important variations among countries and ethnic groups worldwide, caused by both population characteristics and methodological differences. Based on our findings it is important to continue to follow global trends in the incidence and prevalence of type 2 diabetes in the young population and to use a valid study design, appropriate diagnostic tools and the same diagnostic criteria. Population-based screening programmes appear to fulfil most of these requirements although the cost-effectiveness of such programmes is not clear yet.
Abbreviations
- AIHW:
-
Australian Institute of Health And Welfare
- BPSU:
-
British Paediatric Surveillance Unit
- CCDR:
-
Chicago Childhood Diabetes Registry
- CFPC-NaReS:
-
College of Family Physicians of Canada National Research System
- CPSP:
-
Canadian Paediatric Surveillance Program
- DIARY:
-
Diabetes Registry
- FPG:
-
Fasting plasma glucose
- IHS:
-
Indian Health Service
- NIH:
-
National Institute of Health
- NZHIS:
-
New Zealand Health Information Service
- NZPSU:
-
New Zealand Paediatric Surveillance Unit
- RLDR:
-
Richmond/Lexington County Childhood and Adolescents Diabetes Registry
- US PHS:
-
United States Public Health Service
- WACDD:
-
Western Australian Children’s Diabetes Database
References
Chen L, Magliano DJ, Zimmet PZ (2011) The worldwide epidemiology of type 2 diabetes mellitus—present and future perspectives. Nat Rev Endocrinol 8:228–236
Zimmet P, Alberti KG, Shaw J (2001) Global and societal implications of the diabetes epidemic. Nature 414:782–787
Botero D, Wolfsdorf JI (2005) Diabetes mellitus in children and adolescents. Arch Med Res 36:281–290
D’Adamo E, Caprio S (2011) Type 2 diabetes in youth: epidemiology and pathophysiology. Diabetes Care 34(suppl 2):S161–S165
Pinhas-Hamiel O, Zeitler P (2007) Acute and chronic complications of type 2 diabetes mellitus in children and adolescents. Lancet 369:1823–1831
Lipton RB (2007) Incidence of diabetes in children and youth—tracking a moving target. JAMA 297:2760–2762
Fagot-Campagna A, Burrows NR, Williamson DF (1999) The public health epidemiology of type 2 diabetes in children and adolescents: a case study of American Indian adolescents in the Southwestern United States. Clin Chim Acta 286:81–95
Cali AM, Caprio S (2008) Prediabetes and type 2 diabetes in youth: an emerging epidemic disease? Curr Opin Endocrinol Diabetes Obes 15:123–127
American Diabetes Association (2008) Economic costs of diabetes in the U.S. In 2007. Diabetes Care 31:596–615
Stroup DF, Berlin JA, Morton SC et al (2000) Meta-analysis of observational studies in epidemiology. JAMA 283:2008–2012
Urakami T, Kubota S, Nitadori Y, Harada K, Owada M, Kitagawa T (2005) Annual incidence and clinical characteristics of type 2 diabetes in children as detected by urine glucose screening in the Tokyo metropolitan area. Diabetes Care 28:1876–1881
Urakami T, Morimoto S, Nitadori Y, Harada K, Owada M, Kitagawa T (2007) Recent change in the annual incidence of childhood type 2 diabetes in the Tokyo metropolitan area. Clin Pediatr Endocrinol 16:53–58
Urakami T, Owada M, Kitagawa T (2006) Recent trend toward decrease in the incidence of childhood type 2 diabetes in Tokyo. Diabetes Care 29:2176–2177
Rami B, Schober E, Nachbauer E, Waldhor T, Austrian Diabetes Incidence Study Group (2003) Type 2 diabetes mellitus is rare but not absent in children under 15 years of age in Austria. Eur J Pediatr 162:850–852
Schober E, Waldhoer T, Rami B, Hofer S, Austrian Diabetes Incidence Study Group (2009) Incidence and time trend of type 1 and type 2 diabetes in Austrian children 1999-2007. J Pediatr 155:190–193
Dabelea D, Hanson RL, Bennett PH, Roumain J, Knowler WC, Pettitt DJ (1998) Increasing prevalence of type II diabetes in American Indian children. Diabetologia 41:904–910
Pavkov ME, Hanson RL, Knowler WC, Bennett PH, Krakoff J, Nelson RG (2007) Changing patterns of type 2 diabetes incidence among Pima Indians. Diabetes Care 30:1758–1763
Uckun-Kitapci A, Tezic T, Firat S et al (2004) Obesity and type 2 diabetes mellitus: a population-based study of adolescents. J Pediatr Endocrinol Metab 17:1633–1640
Bell RA, Mayer-Davis EJ, Beyer JW et al (2009) Diabetes in non-Hispanic white youth: prevalence, incidence, and clinical characteristics: the SEARCH for Diabetes in Youth Study. Diabetes Care 32(suppl 2):S102–S111
Dabelea D, DeGroat J, Sorrelman C et al (2009) Diabetes in Navajo youth: prevalence, incidence, and clinical characteristics: the SEARCH for Diabetes in Youth Study. Diabetes Care 32(suppl 2):S141–S147
Lawrence JM, Mayer-Davis EJ, Reynolds K et al (2009) Diabetes in Hispanic American youth: prevalence, incidence, demographics, and clinical characteristics: the SEARCH for Diabetes in Youth Study. Diabetes Care 32(suppl 2):S123–S132
Liu LL, Yi JP, Beyer J et al (2009) Type 1 and type 2 diabetes in Asian and Pacific Islander U.S. youth: the SEARCH for Diabetes in Youth Study. Diabetes Care 32(suppl 2):S133–S140
Mayer-Davis EJ, Beyer J, Bell RA et al (2009) Diabetes in African American youth: prevalence, incidence, and clinical characteristics: the SEARCH for Diabetes in Youth Study. Diabetes Care 32(suppl 2):S112–S122
Group SEARCH for Diabetes in Youth Study, Liese AD, D’Agostino RB Jr et al (2006) The burden of diabetes mellitus among US youth: prevalence estimates from the SEARCH for Diabetes in Youth Study. Pediatrics 118:1510–1518
Writing Group for the SEARCH for Diabetes in Youth Study Group, Dabelea D, Bell RA et al (2007) Incidence of diabetes in youth in the United States. JAMA 297:2716–2724
Amed S, Dean HJ, Panagiotopoulos C et al (2010) Type 2 diabetes, medication-induced diabetes, and monogenic diabetes in Canadian children: a prospective national surveillance study. Diabetes Care 33:786–791
Ehtisham S, Hattersley AT, Dunger DB, Barrett TG, British Society for Paediatric Endocrinology and Diabetes Clinical Trials Group (2004) First UK survey of paediatric type 2 diabetes and MODY. Arch Dis Child 89:526–529
Ehtisham S, Kirk J, McEvilly A et al (2001) Prevalence of type 2 diabetes in children in Birmingham. BMJ 322:1428
Feltbower RG, McKinney PA, Campbell FM, Stephenson CR, Bodansky HJ (2003) Type 2 and other forms of diabetes in 0-30 year olds: a hospital based study in Leeds, UK. Arch Dis Child 88:676–679
Haines L, Wan KC, Lynn R, Barrett TG, Shield JP (2007) Rising incidence of type 2 diabetes in children in the U.K. Diabetes Care 30:1097–1101
Kitagawa T, Owada M, Urakami T, Tajima N (1994) Epidemiology of type 1 (insulin-dependent) and type 2 (non-insulin-dependent) diabetes mellitus in Japanese children. Diabetes Res Clin Pract 24 (Suppl):S7–S13
Wei JN, Sung FC, Lin CC, Lin RS, Chiang CC, Chuang LM (2003) National surveillance for type 2 diabetes mellitus in Taiwanese children. JAMA 290:1345–1350
Dean HJ, Young TK, Flett B, Wood-Steiman P (1998) Screening for type-2 diabetes in aboriginal children in northern Canada. Lancet 352:1523–1524
Campbell-Stokes PL, Taylor BJ, New Zealand Children’s Diabetes Working Group (2005) Prospective incidence study of diabetes mellitus in New Zealand children aged 0 to 14 years. Diabetologia 48:643–648
Perez-Perdomo R, Perez-Cardona CM, Allende-Vigo M, Rivera-Rodriguez MI, Rodriguez-Lugo LA (2005) Type 2 diabetes mellitus among youth in Puerto Rico, 2003. P R Health Sci J 24:111–117
Neu A, Feldhahn L, Ehehalt S, Hub R, Ranke MB, DIARY group Baden-Wurttemberg (2009) Type 2 diabetes mellitus in children and adolescents is still a rare disease in Germany: a population-based assessment of the prevalence of type 2 diabetes and MODY in patients aged 0-20 years. Pediatr Diabetes 10:468–473
Ubink-Veltmaat LJ, Bilo HJ, Groenier KH, Houweling ST, Rischen RO, Meyboom-de Jong B (2003) Prevalence, incidence and mortality of type 2 diabetes mellitus revisited: a prospective population-based study in The Netherlands (ZODIAC-1). Eur J Epidemiol 18:793–800
Dean HJ, Mundy RL, Moffatt M (1992) Non-insulin-dependent diabetes mellitus in Indian children in Manitoba. CMAJ 147:52–57
Oeltmann JE, Liese AD, Heinze HJ, Addy CL, Mayer-Davis EJ (2003) Prevalence of diagnosed diabetes among African-American and non-Hispanic white youth, 1999. Diabetes Care 26:2531–2535
Jefferies C, Carter P, Reed PW et al (2012) The incidence, clinical features, and treatment of type 2 diabetes in children <15 yr in a population-based cohort from Auckland, New Zealand, 1995-2007. Pediatr Diabetes 13:294–300
Hsia Y, Neubert AC, Rani F, Viner RM, Hindmarsh PC, Wong IC (2009) An increase in the prevalence of type 1 and 2 diabetes in children and adolescents: results from prescription data from a UK general practice database. Br J Clin Pharmacol 67:242–249
McMahon SK, Haynes A, Ratnam N et al (2004) Increase in type 2 diabetes in children and adolescents in Western Australia. Med J Aust 180:459–461
Thunander M, Petersson C, Jonzon K et al (2008) Incidence of type 1 and type 2 diabetes in adults and children in Kronoberg, Sweden. Diabetes Res Clin Pract 82:247–255
Moore KR, Harwell TS, McDowall JM, Helgerson SD, Gohdes D (2003) Three-year prevalence and incidence of diabetes among American Indian youth in Montana and Wyoming, 1999 to 2001. J Pediatr 143:368–371
Smith TLS, Drum ML, Lipton RB (2007) Incidence of childhood type 1 and non-type 1 diabetes mellitus in a diverse population: The Chicago Childhood Diabetes Registry, 1994 to 2003. J Pediatr Endocrinol Metab 20:1093–1107
Craig ME, Femia G, Broyda V, Lloyd M, Howard NJ (2007) Type 2 diabetes in indigenous and non-indigenous children and adolescents in New South Wales. Med J Aust 186:497–499
Shaw J (2007) Epidemiology of childhood type 2 diabetes and obesity. Pediatr Diabetes 8(suppl 9):7–15
Ludwig DS, Ebbeling CB (2001) Type 2 diabetes mellitus in children: primary care and public health considerations. JAMA 286:1427–1430
Dolan LM, Bean J, D’Alessio D et al (2005) Frequency of abnormal carbohydrate metabolism and diabetes in a population-based screening of adolescents. J Pediatr 146:751–758
Herings RM, de Boer A, Stricker BH, Bakker A, Sturmans F (1995) A rapid method to estimate the incidence rate and prevalence of insulin-dependent diabetes mellitus in children 0-19 years of age. Pharm World Sci 17:17–19
Wu EL, Kazzi NG, Lee JM (2013) Cost-effectiveness of screening strategies for identifying pediatric diabetes mellitus and dysglycemia. JAMA Pediatr 167:32–39
Acknowledgements
The authors would like to thank N. Zuiverloon (librarian at the library of Utrecht University) for her helpful suggestions for searching databases.
Funding
No funding source had any role in the design and conduct of the study, the collection, management, analysis and interpretation of the data or the preparation, review or approval of the manuscript.
The Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht Institute for Pharmaceutical Sciences, has received unrestricted funding from the Netherlands Organisation for Health Research and Development (ZonMW), the Dutch Health Care Insurance Board (CVZ), the Royal Dutch Pharmacists Association (KNMP), the private-public funded Top Institute Pharma (www.tipharma.nl, includes co-funding from universities, government, and industry), the EU Innovative Medicines Initiative (IMI), the EU 7th Framework Program (FP7) and the Dutch Ministry of Health and industry (including GlaxoSmithKline, Pfizer, and others).
Duality of interest
The authors declare that there is no duality of interest associated with this manuscript, no support from any organisation for the submitted work, no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work.
Contribution statement
SFF and MPA searched the literature and extracted data. In case of disagreement AB and MMJV checked the study. All authors discussed the data and interpreted the results. SFF and MPA wrote the manuscript. MMJV, CAJK and AB reviewed and edited the manuscript. All authors approved the final version and take full responsibility for the contents of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM Table 1
(XLSX 207 kb)
Rights and permissions
About this article
Cite this article
Fazeli Farsani, S., van der Aa, M.P., van der Vorst, M.M.J. et al. Global trends in the incidence and prevalence of type 2 diabetes in children and adolescents: a systematic review and evaluation of methodological approaches. Diabetologia 56, 1471–1488 (2013). https://doi.org/10.1007/s00125-013-2915-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-013-2915-z