
Abstract
Aims/hypothesis
Ghrelin is a natural growth hormone-releasing peptide thought to be involved in the regulation of energy metabolism. The recent studies concerning the association between ghrelin and insulin-like growth factor-I (IGF-I) concentrations have shown either negative correlation or no correlation at all. The aims of this study were to clarify the association between ghrelin and IGF-I concentrations in a large cohort and to characterize whether obesity, insulin resistance and type 2 diabetes affect this association.
Methods
We analysed fasting plasma ghrelin and IGF-I concentrations of 1,004 middle-aged subjects of the population-based OPERA study. Insulin resistance was estimated using QUICKI.
Results
IGF-I concentrations were negatively associated with ghrelin concentrations in the analysis of all subjects before (β=−0.32, p<0.001) and after adjustments for BMI, insulin levels, sex and age (β=−0.40, p<0.001). The association was particularly strong in males and in the higher BMI tertiles. The degree of association varied in relation to the glycaemic status: no insulin resistance: r 2=6.5% (p<0.001), insulin resistance without type 2 diabetes: r 2=21.0% (p<0.001), type 2 diabetes: r 2=25.4 (p<0.001). IGF-I levels explained larger proportion (r 2=9.8%) of the variation in ghrelin concentrations compared to fasting insulin concentration (r 2=3.0%) and BMI (r 2=1.5%).
Conclusions/interpretation
There is a negative and independent association between ghrelin and IGF-I concentrations in middle-aged subjects. The interaction between IGF-I and ghrelin is modified by obesity, IR and type 2 diabetes. Further studies are warranted to elucidate the role of ghrelin in the development of these states.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Ghrelin is a recently discovered peptide hormone, which is mainly secreted from the stomach [1]. The effects of ghrelin are mediated through the growth hormone secretagogue receptor (GHSR), which is widely distributed in the body [2]. In addition to its marked growth hormone (GH)-releasing activity [1], ghrelin acts as a powerful orexigenic hormone [3, 4] and this effect appears to be independent of changes in GH [5]. Recent studies have shown that ghrelin also modulates insulin and glucose metabolism [6], and it has further been shown to have beneficial hemodynamic properties [7, 8]. It is a somatotrophic, orexigenic and adipogenic hormone, which may link the regulatory systems for growth and energy balance [9].
The determinants and the regulation of ghrelin concentrations in physiological conditions are poorly known at the moment. Fasting state and meal ingestion probably have the most significant effect on the variation of ghrelin concentration. Food intake and hyperglycaemia suppress ghrelin secretion [10, 11] but it is controversial whether changes in glucose or insulin mediate this effect [10, 12]. Several studies have shown ghrelin to be negatively associated with BMI [13–15] and insulin [13, 15, 16].
Despite the fact that ghrelin has a powerful, rapid, and dose-dependent effect on GH release in experimental studies [1, 17, 18], the functional role of ghrelin in the long-term regulation of GH concentrations in physiological conditions has not yet been clarified. The recent studies are either for [19–22] or against [23–26] the role of ghrelin in the regulation of GH concentrations. If ghrelin has a significant role in the long-term regulation of GH concentration, there should be a detectable association between ghrelin and IGF-I, the most important peripheral effector protein of GH action. However, the results of the recent studies concerning the association between ghrelin and IGF-I are somewhat conflicting showing negative correlation in children and adolescents [27–30] but no correlation at all in adult subjects [31–33]. Sample sizes of these studies have been relatively small.
Based on the strong GH-releasing effect of ghrelin, it can be hypothesised that there is a positive correlation between ghrelin and IGF-I concentrations. On the other hand, based on the recent studies demonstrating negative correlation between ghrelin and IGF-I concentrations in children and adolescents [27–30], a negative correlation can be hypothesised in adults as well. In order to test these competing hypotheses, we analysed the fasting plasma IGF-I and ghrelin concentrations in a large, randomly selected, population-based sample of middle-aged subjects. Since we have previously shown ghrelin to be associated with type 2 diabetes and insulin resistance (IR) [15], our further aim was to analyse whether these metabolic disturbances affect the association between ghrelin and IGF-I. In addition, we wanted to test whether IGFBP-1, the only acute regulator of IGF-I bio-availability [34], is associated with ghrelin concentrations.
Subjects and methods
Subjects
OPERA (Oulu Project Elucidating the Risk of Atherosclerosis) is a population-based epidemiological study addressing the risk factors and disease endpoints of atherosclerotic cardiovascular diseases. The detailed study design has been previously described [35]. The control cohort and hypertensive cohort were randomly selected from Finnish national population registers by age stratification. The hypertensive cohort consists of 600 unrelated subjects (300 men and 300 women aged 40–59 at the time of recruitment) from the city of Oulu entitled to the reimbursement of the costs of antihypertensive medication. For each hypertensive subject, an age- and sex-matched control subject was randomly selected from the same register, excluding the subjects entitled to reimbursement for antihypertensive medication. The overall participation rate of the hypertensive cohort was 86.5% and that of the controls 87.7%. In this study, a total of 1,004 subjects with IGF-I and ghrelin measurements available were screened. An informed consent was obtained from each participant. The study was conducted according to the principles of the Declaration of Helsinki and approved by the Ethical Committee of the Faculty of Medicine, University of Oulu.
Biomedical factors and laboratory analyses
Blood glucose concentration was measured with the glucose dehydrogenase method and plasma insulin concentration with the double RIA method (AIA-PACK IRI, Tosoh Corp., Tokyo, Japan). Insulin sensitivity was assessed using fasting plasma insulin concentrations and a quantitative insulin sensitivity check index (QUICKI=1/[log (fasting insulin)+log(fasting glucose)]) [36]. Type 2 diabetes and IR were determined according to the WHO criteria. The subjects with insulin sensitivity below the lowest quartile of the control cohort (QUICKI<0.563) were regarded as insulin-resistant. The questionnaire presented to all participants elicited detailed information about their smoking habits, alcohol consumption, physical activity, use of medication and medical history.
To obtain a measure of overall ghrelin concentrations, we analysed fasting plasma ghrelin concentrations, which have been shown to correlate strongly with the 24-h integrated AUC values [37]. We used a commercial RIA kit (Phoenix Pharmaceuticals, Belmont, CA, USA), which recognizes both acylated and desacylated ghrelin [15]. The sensitivity of the assay was 12 pg/ml (ED80), and the inter- and intra-assay coefficients of variation (CV), as given by the manufacturer, were 7.5 and 4.0%, respectively. Inter-assay CV in our analyses was 11.2%. Due to the low intra-assay CV of the method [38], only a single measurement for each sample was performed.
IGF-I assay (DSL-10-2800 ACTIVE Non-Extraction IGF-I ELISA; Diagnostic Systems Laboratories, Webster, TX, USA) uses a modified version of the standard acid–ethanol extraction procedure with intra- and interassay CVs of 4.5–8.6 and 3.3–6.8%, respectively. IGFBP-1 was measured with an immunoenzymometric assay (IGFBP-1 IEMA test; Oy Medix Biochemica, Kauniainen, Finland) with an intra-assay CV of 2.4–3.4% and an interassay CV of 4.9–7.4%.
Statistical methods
The association between ghrelin and the variables studied was assessed using analysis of covariance (ANCOVA), linear regression analysis, and partial correlation analysis. The following variables were entered into the multivariate model: BMI, fasting insulin, IGF-I, IGFBP-1, age, sex and study group. To compare the means of the variables measured, Student’s t-test and ANCOVA with Bonferroni corrections were used. Chi square test was carried out to assess the frequency differences in the sex ratio or the ratio of the study cohorts between the ghrelin quartiles.
The interaction between the explanatory variables was tested using ANCOVA. Linear regression analysis was used to adjust the individual ghrelin concentrations for inter-assay variation. Three subjects with very high ghrelin concentrations (>3 SD over the mean) and three subjects with very low IGF-I concentrations (>3 SD below the mean) were excluded from the analyses as outliers. Furthermore, the three subjects found to have type 1 diabetes were excluded from this study. Altogether, the data of 995 subjects were analysed.
Log-transformed values of IGF-I, IGFBP-1, insulin and QUICKI were used to normalise the skewed distributions. All calculations were made with the SPSS (version 9.0; SPSS, Inc.) statistical package. A p value of less than 0.05 was regarded as statistically significant.
Results
The mean fasting plasma ghrelin concentration of the whole study cohort was 668 pg/ml (range 117–1,513 pg/ml). The mean values of ghrelin concentration were 657 and 678 pg/ml in males and females, respectively (p=0.169), and 661 and 674 pg/ml in the hypertensive and control cohorts, respectively (p=0.359). The main characteristics of the study subjects by ghrelin quartiles (Table 1) showed ghrelin concentration to be negatively associated with IGF-I and fasting insulin concentrations and BMI. There was a positive association between ghrelin and insulin sensitivity, but no association between ghrelin and IGFBP-1 levels. Correlation analyses showed statistically significant inter-correlation between ghrelin, IGF-I, IGFBP-1, BMI and insulin (Table 2).
Linear regression analyses of all study subjects showed IGF-I concentration to be negatively associated with ghrelin concentration before (p<0.001) (Fig. 1, Table 3) and after adjustments for the potential confounding factors (p<0.001) (Table 3). Out of the individual factors, IGF-I was the most significant determinant of the plasma ghrelin concentration explaining 9.8% (adjusted r 2) of the variation in ghrelin concentrations. Since the interaction between IGF-I and sex was statistically significant in the multivariate analysis as a predictor of ghrelin concentration (ANCOVA, p<0.05), the analyses were further carried out in both sexes separately (Table 3). IGF-I explained a higher proportion of the variation in ghrelin concentration in males (adjusted r 2=18.9%) compared to females (adjusted r 2=4.4%).

Linear regression between ghrelin and IGF-I concentrations. Open square and segment line, males: n=484, r 2=19.1%, p<0.001; black dot and dash line, females: n=511, r 2=4.6%, p<0.001; solid line, all subjects: n=995, r 2=9.9%, p<0.001
In order to assess whether glycaemic status affects the association between ghrelin and IGF-I, the interaction between glycaemic status (no IR, IR or type 2 diabetes) and IGF-I concentration was tested in the multivariate analysis of all study subjects (ANCOVA), and it was statistically significant (p<0.05). The negative association between ghrelin and IGF-I concentrations is illustrated by simple linear regression (Fig. 2) and stepwise multivariate linear regression analyses (Table 4) separately for the subjects with no IR, with IR and with type 2 diabetes. IGF-I was negatively associated with ghrelin levels in all groups. However, the regression models explained the highest proportion of variation in subjects with type 2 diabetes (r 2=33.7%) and they had the highest regression coefficient for IGF-I as well (β=−0.56, p<0.001). When the sexes were analysed separately, the trends were similar in both groups (data not shown). The subjects with IR had lower IGFBP-1 concentrations (3.2 ng/ml) compared to the subjects without IR (4.6 ng/ml) or with type 2 diabetes (5.9 ng/ml) (ANCOVA adjusted for BMI, age, sex and study group, p<0.001 in pairwise comparisons).

Linear regression between ghrelin and IGF-I concentrations in relation to glycaemic status. a Subjects with no insulin resistance: n=602, r 2=6.5%, p<0.001. b Subjects with insulin resistance: n=304, r 2=21.0%, p<0.001. c Subjects with type 2 diabetes: n=89, r 2=25.4%, p<0.001
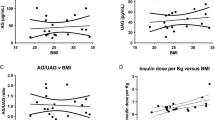
Figure 3 shows the variation of ghrelin concentration in relation to BMI and IGF-I levels in both sexes. The interactions between sex and IGF-I as well as between BMI and IGF-I as a predictor of ghrelin concentrations were significant (p<0.05). When IGF-I and fasting insulin levels were entered into the linear regression analysis stratified according to sex and sex-specific BMI tertiles, IGF-I was the only statistically significant predictor of ghrelin in males in all BMI tertiles (p<0.001), whereas in females, IGF-I was statistically significant only in the second (p=0.002) and third BMI tertiles (p<0.001) (Table 5).

Variation of fasting plasma ghrelin concentrations in relation to sex-specific BMI tertiles and IGF-I quartiles. The first BMI tertile and the first IGF-I quartile refer to the lowest BMI and IGF-I values, respectively. a Males (n=484). b Females (n=511)
Discussion
Our findings in the large, population-based cohort of middle-aged subjects pointed out that IGF-I concentration is a significant determinant of ghrelin concentration, being negatively associated with it. This association was stronger in males and in subjects with high BMI, IR or type 2 diabetes. BMI explained a larger proportion of the variation in ghrelin concentrations in women than in men. IGFBP-1 concentrations were associated with ghrelin concentrations only in subjects with IR.
Since ghrelin has a powerful GH-releasing effect in experimental settings [1, 8, 17, 18], it has been proposed to serve as a regulator of somatotroph function together with GHRH and somatostatin [39, 40]. However, the physiological role of ghrelin in the regulation of GH/IGF-I axis has not yet been established. Several lines of evidence argue against the role of ghrelin in this regulation. Previous studies have shown no change in ghrelin levels in GH-deficient subjects after GH treatment [41, 42]. Pubertal GH surge is not associated with ghrelin levels [27]. Furthermore, GH pulsatility is not explained by changes in ghrelin concentration [43] and acute GH response in exercise is not associated with the changes in ghrelin levels [25, 31]. Interestingly, ghrelin-deficient mice are viable and exhibit a normal growth rate, demonstrating that ghrelin is not critical for normal growth [23]. On the other hand, contrasting findings exist reporting a decrease in ghrelin levels after GH treatment [19], hyperghrelinemia in GH deficiency [20] and relatedness between ghrelin and GH pulsatility [21].
IGF-I has been considered a surrogate measure of GH secretion because of its long circulating half-life and its regulation by GH. Even though IGF-I is not universally regarded as an ideal discriminator of GH status [44], IGF-I measurement is currently the best indirect method to assess GH secretion [45]. The recent studies have reported negative association between ghrelin and IGF-I concentrations in children and adolescents [27–30] whereas nihilistic results has been reported in adult subjects [31–33].
To our best knowledge the results of the present study for the first time show clear and independent negative association between ghrelin and IGF-I concentrations in adult subjects. Our large sample size compared to the sample sizes of the previous studies might explain why association was detected in this study. However, the clear association between IGF-I and ghrelin was somewhat unexpected finding in the light of the several previous studies showing no association between ghrelin and GH/IGF-I axis. Nonetheless, our finding implies that there might be a negative feedback effect of either GH or IGF-I or both on ghrelin concentrations. The elevated ghrelin concentrations and decreased IGF-I concentrations, despite the high GH concentrations, in subjects with chronic liver disease [46] suggest that the regulation may preferably take place between ghrelin and IGF-I and not between ghrelin and GH.
The interpretation of our cross-sectional results is complicated by the complex regulation of IGF-I levels by a series of IGFBPs that control the bio-availability of IGFs [47], and by several other factors like age, sex, nutritional status and peripheral hormones, such as insulin and glucocorticoids that, in addition to GH status, affect IGF-I and/or ghrelin concentrations. In order to control some of these potentially confounding factors, we added them into the multivariate analyses as covariates. In addition, the analyses were carried out as stratified by sex, glycaemic status and BMI tertile. The multivariate analysis of all subjects showed that the association between ghrelin and IGF-I was statistically significant even after adjustments for sex, age, insulin concentration and BMI. In further analyses both sex, BMI and glycaemic status were found to modify the association between ghrelin and IGF-I levels. Nevertheless, the effect of IGF-I in the models remained even after stratifications. However, based on our cross-sectional results we can not definitively tell whether this association reflects mutual regulation between ghrelin and IGF-I or similar regulatory pathways behind ghrelin and IGF-I.
Interestingly, the negative association between ghrelin and IGF-I concentrations was clearly modified by IR and type 2 diabetes. This association was more pronounced among subjects with IR and particularly in a state of extreme insulin resistance, type 2 diabetes. Therefore, serum insulin concentrations seem to be an important determinant of the relationship between ghrelin and IGF-I. Subjects with type 2 diabetes also have decreased ghrelin [15] and IGF-I concentrations [48], which might also modify the association. The roles of IGF-I [49] and ghrelin [50] in the pathophysiology of insulin metabolism are complicated and not yet fully clarified. Whether ghrelin deficiency has a functional role in the development of IR and type 2 diabetes (e.g. by decreasing insulin sensitivity), remains to be explored in further prospective and experimental studies. Based on our findings we can only speculate that ghrelin/IGF-I interactions might also be involved in the development of IR and type 2 diabetes.
We found the association between ghrelin and IGF-I to be modulated by sex, suggesting that there might be a sex-dependent difference in the regulation of ghrelin despite the sex-independent GH-releasing effect of ghrelin [51] and the sex-independent ghrelin levels [15, 29]. Ghrelin concentrations have been reported to depend on sex only in young subjects [52]. The sex difference in the role of ghrelin in the regulation of GH has been previously shown in animal models [53, 54].
To obtain a measure of overall ghrelin concentrations, we used fasting plasma ghrelin concentrations, which have been shown to correlate strongly with the 24-h integrated AUC values [37]. Therefore, the single measurement of fasting plasma ghrelin concentration is well reasoned. Fasting plasma ghrelin concentrations were analysed using antibody that recognises both acylated and des-acylated ghrelin. Although only acylated ghrelin is thought to have endocrine activity [1], non-endocrine functions have been reported for the non-acylated form of ghrelin [55] and, therefore, the measurement of total ghrelin is reasoned. Another reason for the measurement of total ghrelin concentration is that total ghrelin concentration remains significantly better in all conditions compared to acylated ghrelin concentration [56]. Furthermore, total ghrelin is a good surrogate of acylated ghrelin since they are well correlated [57], and the ratio of these two remains constant under a wide variety of conditions [58].
In conclusion, we showed in a large, population-based study that there is an independent negative association between ghrelin and IGF-I concentrations. This association is modified by BMI, gender, IR and type 2 diabetes. Further studies are warranted to elucidate the role of ghrelin in the development of obesity and type 2 diabetes.
Abbreviations
- GH:
-
Growth hormone
- IGF-I:
-
Insulin-like growth factor-I
- IGFBP-1:
-
Insulin-like growth factor binding protein 1
- IR:
-
Insulin resistance
References
Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K (1999) Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature 402:656–660
Gnanapavan S, Kola B, Bustin SA et al. (2002) The tissue distribution of the mRNA of ghrelin and subtypes of its receptor, GHS-R, in humans. J Clin Endocrinol Metab 87:2988–2991
Wren AM, Small CJ, Ward HL et al. (2000) The novel hypothalamic peptide ghrelin stimulates food intake and growth hormone secretion. Endocrinology 141:4325–4328
Shintani M, Ogawa Y, Ebihara K et al. (2001) Ghrelin, an endogenous growth hormone secretagogue, is a novel orexigenic peptide that antagonizes leptin action through the activation of hypothalamic neuropeptide Y/Y1 receptor pathway. Diabetes 50:227–232
Tschöp M, Smiley DL, Heiman ML (2000) Ghrelin induces adiposity in rodents. Nature 407:908–913
Date Y, Nakazato M, Hashiguchi S et al. (2002) Ghrelin is present in pancreatic alpha-cells of humans and rats and stimulates insulin secretion. Diabetes 51:124–129
Nagaya N, Kojima M, Uematsu M et al. (2001) Hemodynamic and hormonal effects of human ghrelin in healthy volunteers. Am J Physiol Regul Integr Comp Physiol 280:R1483–R1487
Enomoto M, Nagaya N, Uematsu M et al. (2003) Cardiovascular and hormonal effects of subcutaneous administration of ghrelin, a novel growth hormone-releasing peptide, in healthy humans. Clin Sci (Lond) 105:431–435
Ukkola O, Pöykkö S (2002) Ghrelin, growth and obesity. Ann Med 34:102–108
Caixas A, Bashore C, Nash W, Pi-Sunyer F, Laferrere B (2002) Insulin, unlike food intake, does not suppress ghrelin in human subjects. J Clin Endocrinol Metab 87:1902
Nakagawa E, Nagaya N, Okumura H et al. (2002) Hyperglycaemia suppresses the secretion of ghrelin, a novel growth-hormone-releasing peptide: responses to the intravenous and oral administration of glucose. Clin Sci (Lond) 103:325–328
Saad MF, Bernaba B, Hwu CM et al. (2002) Insulin regulates plasma ghrelin concentration. J Clin Endocrinol Metab 87:3997–4000
Tschöp M, Weyer C, Tataranni PA, Devanarayan V, Ravussin E, Heiman ML (2001) Circulating ghrelin levels are decreased in human obesity. Diabetes 50:707–709
Shiiya T, Nakazato M, Mizuta M et al. (2002) Plasma ghrelin levels in lean and obese humans and the effect of glucose on ghrelin secretion. J Clin Endocrinol Metab 87:240–244
Pöykkö SM, Kellokoski E, Hörkkö S, Kauma H, Kesäniemi YA, Ukkola O (2003) Low plasma ghrelin is associated with insulin resistance, hypertension, and the prevalence of type 2 diabetes. Diabetes 52:2546–2553
Ikezaki A, Hosoda H, Ito K et al. (2002) Fasting plasma ghrelin levels are negatively correlated with insulin resistance and PAI-1, but not with leptin, in obese children and adolescents. Diabetes 51:3408–3411
Arvat E, Di Vito L, Broglio F et al. (2000) Preliminary evidence that Ghrelin, the natural GH secretagogue (GHS)-receptor ligand, strongly stimulates GH secretion in humans. J Endocrinol Invest 23:493–495
Takaya K, Ariyasu H, Kanamoto N et al. (2000) Ghrelin strongly stimulates growth hormone release in humans. J Clin Endocrinol Metab 85:4908–4911
Eden EB, Burman P, Holdstock C, Karlsson FA (2003) Effects of growth hormone (GH) on ghrelin, leptin, and adiponectin in GH-deficient patients. J Clin Endocrinol Metab 88:5193–5198
Meyer CW, Korthaus D, Jagla W et al. (2004) A novel missense mutation in the mouse growth hormone gene causes semidominant dwarfism, hyperghrelinemia, and obesity. Endocrinology 145:2531–2541
Koutkia P, Canavan B, Breu J, Johnson ML, Grinspoon SK (2004) Nocturnal ghrelin pulsatility and response to growth hormone secretogogues in healthy men. Am J Physiol Endocrinol Metab 287:E506–E512
Tannenbaum GS, Epelbaum J, Bowers CY (2003) Interrelationship between the novel peptide ghrelin and somatostatin/growth hormone-releasing hormone in regulation of pulsatile growth hormone secretion. Endocrinology 144:967–974
Wortley KE, Anderson KD, Garcia K et al. (2004) Genetic deletion of ghrelin does not decrease food intake but influences metabolic fuel preference. Proc Natl Acad Sci U S A 101:8227–8232
Tolle V, Kadem M, Bluet-Pajot MT et al. (2003) Balance in ghrelin and leptin plasma levels in anorexia nervosa patients and constitutionally thin women. J Clin Endocrinol Metab 88:109–116
Schmidt A, Maier C, Schaller G et al. (2004) Acute Exercise has no effect on ghrelin plasma concentrations. Horm Metab Res 36:174–177
Murdolo G, Lucidi P, Di Loreto C et al. (2003) Circulating ghrelin levels of visceral obese men are not modified by a short-term treatment with very low doses of GH replacement. J Endocrinol Invest 26:244–249
Whatmore AJ, Hall CM, Jones J, Westwood M, Clayton PE (2003) Ghrelin concentrations in healthy children and adolescents. Clin Endocrinol (Oxf) 59:649–654
Bellone S, Rapa A, Vivenza D et al. (2003) Circulating ghrelin levels in newborns are not associated to gender, body weight and hormonal parameters but depend on the type of delivery. J Endocrinol Invest 26:RC9–RC11
Bellone S, Rapa A, Vivenza D et al. (2002) Circulating ghrelin levels as function of gender, pubertal status and adiposity in childhood. J Endocrinol Invest 25:RC13–RC15
Kitamura S, Yokota I, Hosoda H et al. (2003) Ghrelin concentration in cord and neonatal blood: relation to fetal growth and energy balance. J Clin Endocrinol Metab 88:5473–5477
Dall R, Kanaley J, Hansen TK et al. (2002) Plasma ghrelin levels during exercise in healthy subjects and in growth hormone-deficient patients. Eur J Endocrinol 147:65–70
Malik IA, English PJ, Ghatei MA, Bloom SR, MacFarlane IA, Wilding JP (2004) The relationship of ghrelin to biochemical and anthropometric markers of adult growth hormone deficiency. Clin Endocrinol (Oxf) 60:137–141
Rigamonti AE, Pincelli AI, Corra B et al. (2002) Plasma ghrelin concentrations in elderly subjects: comparison with anorexic and obese patients. J Endocrinol 175:R1–R5
Jones JI, Clemmons DR (1995) Insulin-like growth factors and their binding proteins: biological actions. Endocr Rev 16:3–34
Rantala AO, Kauma H, Lilja M, Savolainen MJ, Reunanen A, Kesäniemi YA (1999) Prevalence of the metabolic syndrome in drug-treated hypertensive patients and control subjects. J Intern Med 245:163–174
Katz A, Nambi SS, Mather K et al. (2000) Quantitative insulin sensitivity check index: a simple, accurate method for assessing insulin sensitivity in humans. J Clin Endocrinol Metab 85:2402–2410
Cummings DE, Purnell JQ, Frayo RS, Schmidova K, Wisse BE, Weigle DS (2001) A preprandial rise in plasma ghrelin levels suggests a role in meal initiation in humans. Diabetes 50:1714–1719
Gröschl M, Wagner R, Dotsch J, Rascher W, Rauh M (2002) Preanalytical influences on the measurement of ghrelin. Clin Chem 48:1114–1116
Pombo M, Pombo CM, Garcia A et al. (2001) Hormonal control of growth hormone secretion. Horm Res 55(Suppl 1):11–16
Veldhuis JD, Bowers CY (2003) Three-peptide control of pulsatile and entropic feedback-sensitive modes of growth hormone secretion: modulation by estrogen and aromatizable androgen. J Pediatr Endocrinol Metab 16(Suppl 3):587–605
Janssen JA, van der Toorn FM, Hofland LJ et al. (2001) Systemic ghrelin levels in subjects with growth hormone deficiency are not modified by one year of growth hormone replacement therapy. Eur J Endocrinol 145:711–716
Hoybye C, Barkeling B, Espelund U, Petersson M, Thoren M (2003) Peptides associated with hyperphagia in adults with Prader–Willi syndrome before and during GH treatment. Growth Horm IGF Res 13:322–327
Tolle V, Bassant MH, Zizzari P et al. (2002) Ultradian rhythmicity of ghrelin secretion in relation with GH, feeding behavior, and sleep–wake patterns in rats. Endocrinology 143:1353–1361
Aimaretti G, Corneli G, Baldelli R et al. (2003) Diagnostic reliability of a single IGF-I measurement in 237 adults with total anterior hypopituitarism and severe GH deficiency. Clin Endocrinol (Oxf) 59:56–61
Clemmons DR (2001) Commercial assays available for insulin-like growth factor I and their use in diagnosing growth hormone deficiency. Horm Res 55(Suppl 2):73–79
Tacke F, Brabant G, Kruck E et al. (2003) Ghrelin in chronic liver disease. J Hepatol 38:447–454
Le Roith D (1997) Seminars in medicine of the Beth Israel Deaconess Medical Center. Insulin-like growth factors. N Engl J Med 336:633–640
Janssen JA, Lamberts SW (2002) The role of IGF-I in the development of cardiovascular disease in type 2 diabetes mellitus: is prevention possible? Eur J Endocrinol 146:467–477
Le Roith D, Scavo L, Butler A (2001) What is the role of circulating IGF-I? Trends Endocrinol Metab 12:48–52
Ukkola O (2003) Ghrelin and insulin metabolism. Eur J Clin Invest 33:183–185
Broglio F, Benso A, Castiglioni C et al. (2003) The endocrine response to ghrelin as a function of gender in humans in young and elderly subjects. J Clin Endocrinol Metab 88:1537–1542
Barkan AL, Dimaraki EV, Jessup SK, Symons KV, Ermolenko M, Jaffe CA (2003) Ghrelin secretion in humans is sexually dimorphic, suppressed by somatostatin, and not affected by the ambient growth hormone levels. J Clin Endocrinol Metab 88:2180–2184
Shuto Y, Shibasaki T, Otagiri A et al. (2002) Hypothalamic growth hormone secretagogue receptor regulates growth hormone secretion, feeding, and adiposity. J Clin Invest 109:1429–1436
Liu YL, Yakar S, Otero-Corchon V, Low MJ, Liu JL (2002) Ghrelin gene expression is age-dependent and influenced by gender and the level of circulating IGF-I. Mol Cell Endocrinol 189:97–103
Baldanzi G, Filigheddu N, Cutrupi S et al. (2002) Ghrelin and des-acyl ghrelin inhibit cell death in cardiomyocytes and endothelial cells through ERK1/2 and PI 3-kinase/AKT. J Cell Biol 159:1029–1039
Hosoda H, Doi K, Nagaya N et al. (2004) Optimum collection and storage conditions for ghrelin measurements: octanoyl modification of ghrelin is rapidly hydrolyzed to desacyl ghrelin in blood samples. Clin Chem 50:1077–1080
Marzullo P, Verti B, Savia G et al. (2004) The relationship between active ghrelin levels and human obesity involves alterations in resting energy expenditure. J Clin Endocrinol Metab 89:936–939
Ariyasu H, Takaya K, Hosoda H et al. (2002) Delayed short-term secretory regulation of ghrelin in obese animals: evidenced by a specific RIA for the active form of ghrelin. Endocrinology 143:3341–3350
Acknowledgements
The Research Council for Health of the Academy of Finland, the Finnish Foundation for Cardiovascular Research, the Finnish Medical Foundation, the Aarne Koskelo Foundation, and the Ida Montin Foundation supported this study. We acknowledge the excellent technical assistance of Ms. Helena Kalliokoski, Ms.Saija Kortetjärvi, Ms. Liisa Mannermaa, and Ms. Sirpa Rannikko.
Duality of Interest
There is no duality of interest concerning any financial or other interests directly or indirectly related to the subject of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pöykkö, S.M., Ukkola, O., Kauma, H. et al. The negative association between plasma ghrelin and IGF-I is modified by obesity, insulin resistance and type 2 diabetes. Diabetologia 48, 309–316 (2005). https://doi.org/10.1007/s00125-004-1635-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-004-1635-9