
Abstract
Aims/hypothesis
We have examined markers of haemostasis and inflammation in men with diabetes, coronary heart disease (CHD) or both, and assessed their associations with insulin resistance in men with Type 2 diabetes.
Methods
The study was carried out in 4066 British men aged 60 to 79 years who were not on warfarin or insulin, of whom there were 426 men with prevalent Type 2 diabetes and 842 with prevalent CHD.
Results
Men with Type 2 diabetes were more likely to have multiple risk factors and higher levels of haemostatic and inflammatory markers than men without, irrespective of CHD status. Compared with men with CHD only, men with diabetes only showed increased levels of tissue plasminogen activator antigen, increased plasma and blood viscosity, and increased levels of coagulation factors VII, VIII and IX. They also had dyslipidaemia. In men with diabetes, increased insulin resistance (homeostasis model assessment, HOMA) was associated with increased levels of haemostatic markers and dyslipidaemia. The prevalence of CHD increased significantly with increasing tertiles of HOMA (adjusted odds ratio 1.32 [95% CI: 0.72–2.42] in the second, and 1.70 [95% CI: 0.92–3.44] in the third tertile; p=0.04 for trend).
Conclusions/interpretation
Increased insulin resistance among men with Type 2 diabetes is associated with increased prevalence of CHD and of activated haemostasis and dyslipidaemia. Reducing insulin resistance in men with diabetes may reduce their tendency to develop thrombosis and hence CHD risk.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus is associated with a markedly increased risk of cardiovascular mortality compared with the risk in people without diabetes [1]. It has been suggested that CHD risk in diabetic patients is equivalent to that associated with prior myocardial infarction in non-diabetic people [2], although some studies, especially in men, found previous myocardial infarction to be associated with higher risk than diabetes [3, 4, 5]. However, virtually all studies observed that diabetes worsens the prognosis for survival in the presence of CHD [2, 3, 4, 5]. The increased risk of CHD in persons with diabetes does not appear to be adequately explained by the presence of the major conventional CHD risk factors such as smoking, hypertension and hypercholesterolaemia, and attention has consequently turned to other mechanisms [6]. Abnormalities of haemostasis, impaired fibrinolysis, hypercoagulability and increased platelet aggregation are often present in diabetes and are potentially contributory factors [6, 7, 8]. While several studies have documented haemostatic abnormalities in diabetes, few have compared markers of haemostasis and inflammation in subjects with diabetes only and subjects with CHD only. It has been suggested that insulin-resistant subjects with Type 2 diabetes have more atherogenic risk factors than insulin-sensitive subjects with Type 2 diabetes [9], and persons with Type 2 diabetes and established CHD have been shown to be more insulin resistant than those without CHD [10]. There is increasing evidence, mostly in non-diabetic subjects, that insulin resistance is associated with markers of activated haemostasis and inflammation, which could contribute to the development of CHD [11, 12, 13, 14, 15, 16]. The relationship between insulin resistance and haemostatic and inflammatory markers in persons with diabetes has been less extensively studied. The aims of this study were two-fold: (i) to examine the cardiovascular risk profile (including haemostatic and inflammatory markers) in older men according to Type 2 diabetes and CHD status, in order to identify factors that may contribute to the excess risk of cardiovascular disease (CVD) mortality in men with diabetes and to the exceptionally poor prognosis of men with both diabetes and CHD; and (ii) to assess the relationship of homeostasis model assessment (HOMA; a marker of insulin resistance) to haemostatic and inflammatory markers and to CHD risk factors in men with Type 2 diabetes. We hypothesised that men with both diabetes and CHD would have a more adverse cardiovascular risk profile than men with CHD only, and that men with diabetes and marked insulin resistance would be more likely to have increased atherogenic and prothrombotic risk factors than men with diabetes who were not markedly insulin resistant.
Subjects and methods
Subjects
The British Regional Heart Study is a prospective study of cardiovascular disease involving 7735 men aged 40 to 59 years, selected from the age–sex registers of one general practice in 24 British towns, who were screened between 1978 and 1980 and have been followed up for all-cause mortality and for the development of cardiovascular morbidity and diabetes through regular 2-yearly reviews of general practice records [17, 18]. Ethics approval was provided by all relevant local research ethics committees. All men provided informed written consent to participate in the investigation, and procedures were carried out in accordance with the Declaration of Helsinki. Between 1998 and 2000, all surviving men, now aged 60 to 79 years, were invited for a 20th-year follow-up examination. All men completed a questionnaire (referred to as Q20) providing information on their medical history and lifestyle characteristics and had a physical examination. The men were asked to fast for a minimum of 6 hours, during which they were instructed to drink only water and to attend for measurement at a pre-specified time between 08.00 and 18.00 hours. They then provided a blood sample, collected using the Sarstedt Monovette system. Of the 5565 surviving subjects, 4252 (77%) attended for examination. All men on warfarin, which affects levels of several haemostatic variables, were excluded from analyses (n=145).
Cardiovascular risk factors
A number of anthropometric variables were measured, including body weight, height and waist circumference. Details of classification methods for smoking status, physical activity, BMI, alcohol intake and social class, and measurements of blood pressure and blood lipids have been described [17, 19, 20, 21]. Obesity is defined as a BMI of 30 kg/m2 or higher. Blood pressure, measured using a Dinamap 1846, was adjusted for observer variation [22]. HDL cholesterol and triglycerides were measured using established methods [20]. Plasma glucose was measured using a glucose oxidase method [23]. Serum insulin was measured using an ELISA assay that does not cross-react with proinsulin [24]. Triglycerides, glucose and insulin concentrations were adjusted for the effects of fasting duration and time of day in men with no doctor diagnosis of diabetes [20].
Prevalent CHD
The men were asked whether a doctor had ever told them that they had angina or myocardial infarction (heart attack, coronary thrombosis), stroke, diabetes or a number of other disorders.
Prevalent CHD included men who recalled a doctor diagnosis of CHD (heart attack or angina) at Q20 and those who had suffered a major non-fatal myocardial infarction event or angina event prior to Q20 based on biennial reviews of each patient’s general practice records, including all hospital reports and correspondence, between initial screening in 1978–1980 and the completion of Q20. A non-fatal myocardial infarction was defined by the presence of at least two of the following: severe prolonged chest pain, ECG evidence of myocardial infarction, and cardiac enzyme changes consistent with myocardial infarction.
Prevalent diabetes
Information on prevalent diabetes was based on the following: (i) regular reviews of general practice medical records between initial screening in 1978–1980 and the return of Q20; (ii) the subject recalling physician-diagnosed diabetes (data obtained in Q20); and (iii) fasting blood glucose at Q20. Men with a doctor diagnosis of diabetes (documentation in any of the biennial general practice record reviews or subject recalling diagnosis at Q20) and those with a fasting glucose of 7 mmol/l or higher (WHO criteria for diagnosis) at Q20 were all considered to have prevalent diabetes in this study (n=467). To restrict analyses to cases of Type 2 diabetes, we excluded all diabetic patients on insulin injections (n=41), as some of these men are likely to have Type 1 diabetes. Insulin resistance was estimated according to the HOMA model as the product of fasting glucose (mmol/l) and insulin (μU/ml) divided by the constant 22.5 [25]. HOMA was shown to be significantly correlated with insulin sensitivity in men with Type 2 diabetes [25]. The correlation between HOMA and insulin was r=0.96 and the correlation between HOMA and blood glucose was r=0.56.
Metabolic syndrome
The metabolic syndrome, as defined by the US National Cholesterol Education Program [26], includes three or more of the following: (i) a fasting plasma glucose of at least 6.1 mmol/l; (ii) serum triglycerides of at least 1.7 mmol/l; (iii) a serum HDL cholesterol of less than 1.04 mmol/l; (iv) a blood pressure of at least 130/85 mm Hg or patient being on antihypertensive treatment; and (v) waist circumference of more than 102 cm.
Haemostatic and inflammatory variables
Blood was anticoagulated with K2 EDTA (1.5 mg/ml) for measurement of haematocrit, white cell count and platelet count in an automated cell counter, and of plasma viscosity at 37 °C in a semi-automated capillary viscometer (Coulter Electronics, Luton, UK). Blood viscosity was calculated from haematocrit and plasma viscosity [27]. Blood was also anticoagulated with 0.109 mol/l trisodium citrate (9:1, v/v) for measurement of clottable fibrinogen (Clauss method), coagulation factors VII, VIII and IX, and activated partial thromboplastin time (APPT) in an MDA-180 coagulometer (Organon Teknika, Cambridge, UK). Plasma levels of tissue plasminogen activator (t-PA) antigen and d-dimer were measured with ELISA (Biopool AB, Umea, Sweden) as was von Willebrand factor (vWF) antigen (Dako, High Wycombe, UK). C-reactive protein (CRP) was assayed by ultra-sensitive nephelometry (Dade Behring, Milton Keynes, UK).
Statistical analysis
The distributions of white cell count, CRP and fibrin d-dimer were highly skewed and log transformation was used. Analysis of covariance was used to obtain adjusted mean levels according to diabetes and CHD status, and by tertiles of HOMA distribution in men with diabetes. Age and waist circumference were fitted as continuous variables; physical activity, alcohol intake and smoking were used as categorical variables. BMI and waist circumference were highly correlated (r=0.87) and adjustment for body fat distribution was carried out using waist circumference, as it may provide a better measure of visceral adiposity [28]. Logistic regression was used to obtain adjusted odds ratios for CHD and the metabolic syndrome.
Results
There were 426 men with Type 2 diabetes and 842 men with CHD among the 4066 men not on warfarin or on insulin injections. Table 1 shows the mean and SD for the biochemical and haematological factors. Table 2 shows the demographic characteristics and the mean levels of risk factors according to diabetes and CHD status. Irrespective of CHD status, men with diabetes were significantly more obese and had significantly higher fasting insulin levels than men without diabetes.
Men with no CHD
Of the men with no CHD, those with diabetes showed significantly higher levels of insulin, blood glucose and inflammatory markers (CRP, fibrinogen and white cell count), higher plasma viscosity, higher blood viscosity, increased levels of t-PA antigen, vWF antigen and coagulation factors VII, VIII and IX, shorter APPT, lower HDL cholesterol, and higher triglycerides and systolic blood pressure than men with no diabetes (Table 2). These differences persisted after adjustment for smoking, physical activity and alcohol. After further adjustment for abdominal obesity, the relationship with CRP was weaker (p=0.11) and the relationships with fibrinogen and factor VII were only of marginal significance (p=0.08 and p=0.07 respectively).
Men with CHD
Similar patterns were seen among men with CHD. Those with diabetes and CHD showed significantly higher levels of triglycerides, lower concentrations of HDL cholesterol, higher levels of t-PA antigen and factors VIII and IX, and higher levels (marginal significance) of vWF antigen than men with CHD only. They also had higher levels of inflammatory markers (CRP, white cell count), plasma viscosity and factor VII, but these differences were not statistically significant.
Comparisons between men with diabetes only and men with CHD only
Comparisons between men with CHD only and men with diabetes only showed men with diabetes only to have a significantly higher waist circumference and BMI and a higher prevalence of obesity (Table 2). They also had significantly higher levels of HOMA, fasting insulin, systolic and diastolic blood pressure, triglycerides, blood viscosity, haematocrit, t-PA, and factors VII, VIII and IX, as well as reduced APPT, and to a lesser extent, lower levels of HDL cholesterol and higher levels of vWF antigen than men with CHD only (Table 2). On the other hand, men with diabetes only had lower levels of fibrin d-dimer than men with CHD only. Overall, men with diabetes only had more cardiovascular risk factors and more activated haemostasis than men with CHD only.
Metabolic syndrome
We examined the prevalence (%) and adjusted odds ratio of the metabolic syndrome (National Cholesterol Education Program definition) by the presence of diabetes and CHD. Prevalent diabetes without CHD but not prevalent CHD without diabetes was significantly associated with the metabolic syndrome (Table 3). Men with diabetes only were far more likely to have metabolic abnormalities than men with CHD only. This is consistent with the markedly high prevalence of insulin resistance (elevated HOMA) in men with diabetes only (Table 3).
Insulin resistance, CVD risk factors and haemostatic and inflammatory markers among men with diabetes
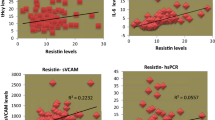
We examined the relationship between tertiles of HOMA as a measure of insulin resistance and the prevalence of CHD (Table 4). HOMA was positively and significantly associated with increased prevalence of CHD even after adjustment for age, smoking, physical activity, alcohol intake and waist circumference. Table 5 shows the relationship of HOMA (tertiles) with CVD risk factors and haemostatic and inflammatory markers in men with Type 2 diabetes. To avoid confounding in assessment of the relationship between HOMA and the biological factors, we excluded all men with CHD. Only factors shown to be associated with HOMA after adjustment for age, physical activity, alcohol intake and smoking are presented. HOMA was significantly associated with HDL cholesterol (inversely), and positively associated with triglycerides, CRP, t-PA antigen, vWF antigen, factors VII, VIII and IX, and to a lesser extent, with plasma viscosity (Table 4). The significant association with HDL cholesterol, triglycerides, factor VIII and vWF antigen persisted after adjustment for waist circumference. The positive association with CRP, fibrinogen, plasma viscosity, factors VII and IX, t-PA antigen and APPT weakened after further adjustment for waist circumference, and the trends were no longer statistically significant. No association was observed between HOMA and systolic or diastolic blood pressure, haematocrit, blood viscosity, white cell count, platelet count or activated protein C ratio (data not shown). Among men with diabetes with low HOMA, levels of HDL cholesterol, triglycerides, vWF antigen, t-PA antigen, factor VII and fibrinogen were similar to levels in men without diabetes (Table 1).
We repeated the analyses in Table 5 adjusting for BMI instead of waist circumference. The relationships shown in Table 5 were broadly similar to those found when adjusting for waist circumference, but the positive associations with CRP, fibrinogen, factor IX, t-PA antigen and APPT, although weakened, remained of marginal significance (p=0.07, p=0.07, p=0.03, p=0.05 and p=0.06 respectively).
Discussion
Diabetes is associated with an excess risk of CHD, which is not adequately explained by the conventional risk factors such as hypertension, dyslipidaemia and smoking. Attention has therefore turned to other mechanisms that may relate to atherogenesis or thrombogenesis in patients with Type 2 diabetes, in particular the role of insulin resistance. In this study of men aged 60 to 79 years, those with diabetes showed significantly increased dyslipidaemia and activated haemostasis and inflammation compared with those without, a finding more apparent in those with no history of CHD. These differences in haemostatic and inflammatory markers were not explained by potential confounders such as smoking, physical activity, alcohol intake and abdominal obesity, although the relationship with CRP was weakened after adjustment for abdominal adiposity. The increased levels of endothelial markers (t-PA antigen, vWF antigen), clotting factors (fibrinogen, factors VII and VIII), inflammatory markers (CRP, white cell count) and plasma viscosity in subjects with diabetes have also been reported in other studies [6, 7, 8, 13, 29], and these factors are also related to CHD risk [27, 30, 31, 32, 33, 34]. In addition we showed that men with diabetes also had markedly increased levels of factor IX and shortened APPT. There are few reports on the association of factor IX and APPT with risk of CHD, although factor IX and APPT have been shown to be associated with venous thromboembolism [35, 36]. Prospective studies have shown elevated CRP, fibrinogen, vWF antigen and fibrinolytic variables (t-PA antigen and plasminogen activator inhibitor-1 [PAI-1]) to predict CHD in subjects with diabetes [37, 38]. Thus, the excess risk of cardiovascular events in subjects with diabetes may in part be mediated by its effects on blood coagulation, fibrinolysis, inflammation and blood rheology. Plasma fibrin d-dimer was not elevated in persons with Type 2 diabetes without CHD in the present study. This finding is consistent with that of the Speedwell study, another UK population study [39]. Previous reports of raised d-dimer in persons with diabetes have tended to come from smaller studies of patients with diabetic vascular complications, and may reflect the presence of vascular disease rather than diabetes itself.
Haemostatic and inflammatory markers in men with CHD only and in men with Type 2 diabetes only
Almost all studies show that persons with both CHD and diabetes have a worse prognosis than persons with CHD but no diabetes [2, 3, 4, 5], but few studies have compared the risk profile of those with diabetes only and those with CHD only. We have shown that men with diabetes only tend to have more activated haemostasis and dyslipidaemia than subjects with CHD only, and that they are more likely to have multiple metabolic abnormalities. The metabolic syndrome was present in almost 70% of men with diabetes only compared with about 30% in subjects with CHD only. These multiple risk factors may contribute to the exceptionally poor prognosis of persons with diabetes and CHD, compared with in those with CHD only. In addition to the haemostatic variables assayed in the present study, PAI-1, an inhibitor of fibrinolysis, has been shown to be higher in persons with both diabetes and myocardial infarction than in patients with myocardial infarction but no diabetes, and it has been suggested that this factor may play a role in increasing the magnitude of the first coronary thrombotic event and in increasing the risk of reinfarction [11]. Although we did not measure PAI-1, t-PA antigen levels, which are strongly correlated with PAI-1 levels [40], were significantly higher in subjects with diabetes and CHD than in men with CHD only. An increase in t-PA antigen may reflect endothelial disturbance and elevated PAI-1 [33]. This antigen has been shown to predict recurrence of myocardial infarction [40] and may play a role in coronary plaque rupture [41]. Factor VIII and vWF antigen, which like t-PA antigen is a marker of endothelial disturbance, were also higher in subjects with CHD and diabetes than in subjects with CHD only. Factor VIII and vWF antigen are closely related and play an important role not only in promoting platelet adhesion and aggregation but also in coagulation, enhancing propagation of thrombi and thereby potentially contributing to risk of CHD [32]. In addition, vWF antigen has been shown to predict recurrent myocardial infarction [40]. Thus, elevated t-PA antigen and vWF antigen in subjects with diabetes may not only be risk factors for CHD, but may also contribute to the poor prognosis of diabetes patients with clinical CHD.
Insulin resistance and haemostatic and inflammatory markers in men with diabetes
While many mechanisms are undoubtedly involved in the development of vascular disease in diabetes, insulin resistance is thought to play a major role in the acceleration of atherosclerosis [6, 9, 42]. Previous studies in diabetes suggest that insulin-resistant subjects are more likely to have atherogenic risk factors and metabolic disorders related to the insulin resistance syndrome [9, 43]. The relationship between insulin resistance and fibrinolysis in diabetes is well documented [6, 8, 11], but other haemostatic and inflammatory markers have been less well studied. In the present study we have shown that among men with diabetes, those with increased insulin resistance (as assessed by HOMA) were more likely to have an increased prevalence of CHD, and were also more likely to have dyslipidaemia as well as elevated t-PA antigen, fibrinogen, coagulation factors VII, VIII and IX, and inflammatory markers even after adjustment for smoking, alcohol intake and physical activity. With the exceptions of dyslipidaemia, vWF antigen and factor VIII, these associations were somewhat attenuated after further adjustment for abdominal obesity. Adjustment for waist circumference tended to attenuate the relationships more than adjusting for BMI, supporting the suggestion that waist circumference is a better marker of visceral obesity [28], and suggesting that waist circumference (visceral adiposity) may be a better marker of inflammatory and haemostatic markers than BMI (general adiposity). Since insulin resistance may mediate some of the effects of abdominal adiposity, adjustment for waist circumference could be an over-adjustment and could lead to underestimation of the effect of insulin resistance. The levels of many of the risk factors in diabetic men with low HOMA values were similar to levels in men without diabetes. Thus, increases in atherogenic and thrombotic risk factors are more likely to occur in men with diabetes who are more insulin resistant. The significant association between insulin resistance and t-PA antigen, vWF antigen and fibrinogen in subjects with diabetes, observed in the present study, has also been reported in the Framingham Offspring Study [13].
The biological mechanisms underlying the association between insulin resistance and haemostatic variables are not yet completely clear. It is now recognised that impaired fibrinolytic potential is a major feature of insulin resistance [12]. The association between HOMA and fibrinogen and CRP is consistent with the suggestion that insulin is associated with inflammatory cytokines, and the strong relationship with vWF antigen and t-PA antigen supports the suggestion that insulin resistance may induce endothelial dysfunction [12] or vice versa. Our findings that insulin resistance is associated with a prothrombotic risk profile and prevalent CHD in men with diabetes are consistent with those of prospective studies that have shown insulin resistance to be associated with increased risk of CVD in Type 2 diabetes, independently of conventional risk factors such as smoking, HDL cholesterol and blood pressure [44, 45]. Thus, insulin resistance may accelerate atherothrombosis in subjects with diabetes through its effect on haemostatic and inflammatory markers.
Limitations
Although we did not use direct measures of insulin resistance [46], and although fasting insulin concentration may not be optimal as a surrogate for insulin resistance in subjects with Type 2 diabetes [9], HOMA (a product of fasting insulin and glucose) has been shown to be significantly correlated with insulin sensitivity and to predict CVD in subjects with diabetes [25, 44]. We have found HOMA to have significant associations with dyslipidaemia and haemostatic and inflammatory markers, which is consistent with the results of the limited number of studies that have used direct measures of insulin sensitivity [9].
Conclusions
We have shown that men with Type 2 diabetes tend to have not only dyslipidaemia but also activated haemostasis and inflammation, which may contribute to risk of cardiovascular events. Overall, men with diabetes had more activated haemostasis than men with CHD only. Insulin-resistant men with diabetes are more likely to have atherogenic and prothrombotic risk profiles and prevalent CHD than insulin-sensitive men with diabetes. These findings have potential implications for understanding CHD risk in older men with Type 2 diabetes. The findings are consistent with the observations of the UK Prospective Diabetes Study (UKPDS), which reported that the improvement in insulin sensitivity with metformin is associated with a significant reduction in diabetes-related endpoints, all-cause mortality and stroke in overweight patients with Type 2 diabetes [47]. Reducing insulin resistance in men with diabetes may reduce their tendency to develop thrombosis, hence reducing risk of CHD. It remains to be seen whether reducing insulin resistance, by non-pharmacological (weight reduction and physical activity) or pharmacological therapy reduces activation of haemostasis and inflammation.
Abbreviations
- APPT:
-
activated partial thromboplastin time
- CRP:
-
C-reactive protein
- CVD:
-
cardiovascular disease
- HOMA:
-
homeostasis model assessment
- PAI-1:
-
plasminogen activator inhibitor-1
- Q20:
-
questionnaire completed at 20th-year follow-up examination
- t-PA:
-
tissue plasminogen activator
- vWF:
-
von Willebrand factor
References
Kannel WB, McGee DL (1979) Diabetes and glucose tolerance as risk factors for CVD: the Framingham study. Diabetes Care 2:120–126
Haffner SM, Lehto S, Ronnema T et al. (1998) Mortality from coronary heart disease in subjects with Type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 339:229–234
Cho E, Rimm EB, Stampfer MJ, Willett WC, Hu FB (2002) The impact of diabetes mellitus and prior myocardial infarction on mortality from all causes and from coronary heart disease in men. J Am Coll Cardiol 40:954–960
Lotufo PA, Gaziano M, Chae CU et al. (2001) Diabetes and all cause and coronary heart disease mortality among US Male Physicians. Arch Intern Med 161:242–247
Becker A, Bos G, de Vegt F et al. (2003) Cardiovascular events in Type 2 diabetes: comparison with nondiabetic individuals without and with prior cardiovascular disease: 10-year follow-up of the Hoorn Study. Eur Heart J 24:1406–1413
Beckman JA, Creager MA, Libby P (2002) Diabetes and atherosclerosis: epidemiology, pathophysiology and management. JAMA 287:2570–2581
Carr ME (2001) Diabetes mellitus: a hypercoagulable state. J Diabetes Compl 15:44–54
Schneider DJ, Nordt TK, Sobel BE (1993) Attenuated fibrinolysis and accelerated atherogenesis in type II diabetic patients. Diabetes 42:1–7
Haffner SM, Rewers M, D’Agostino R et al. (1999) Insulin sensitivity in subjects with type 2 diabetes. Diabetes Care 22:562–568
Inchiostro S, Bertoli G, Zanette G, Donadon V (1994) Evidence of higher insulin resistance in NIDDM patients with ischemic heart disease. Diabetologia 137:597–603
Yudkin JS (1999) Abnormalities of coagulation and fibrinolysis in insulin resistance. Evidence for a common antecedent. Diabetes Care 22 [Suppl 3]:C25–C30
Kohler HP (2002) Insulin resistance syndrome: interaction with coagulation and fibrinolysis. Swiss Med Wkly 132:241–252
Meigs JB, Mittleman MA, Nathan DM et al. (2000) Hyperinsulinemia, hyperglycemia, and impaired hemostasis. JAMA 283:221–228
Marques-Vidal P, Mazoyer E, Bongard V et al. (2003) Prevalence of insulin resistance syndrome in Southwestern France and its relationship with inflammatory and hemostatic markers. Diabetes Care 25:1371–1377
Yudkin JS, Stehouwer CDA, Emeis JJ, Coppack SW (1999) C-reactive protein in healthy subjects: associations with obesity, insulin resistance and endothelial dysfunction. Arterioscler Thromb Vasc Biol 19:972–978
Festa A, D’Agostino R, Howard G, Mykkanen L, Tracey RP, Haffner S (2000) Chronic subclinical inflammation as part of the insulin resistance syndrome: The Insulin Resistance Atherosclerosis Study (IRAS). Circulation 102:42–47
Shaper AG, Pocock SJ, Walker M, Cohen NM, Wale CJ (1981) British Regional Heart Study: cardiovascular risk factors in middle-aged men in 24 towns. BMJ 283:179–186
Walker M, Shaper AG, Lennon L, Whincup PH (2000) Twenty years follow-up of a cohort based in general practices in 24 British towns. J Public Health Med 22:479–485
Wannamethee SG, Lowe GDO, Whincup PH, Rumley A, Walker M, Lennon L (2002) Physical activity and hemostatic and inflammatory variables in elderly men. Circulation 105:1785–1790
Emberson J, Whincup PH, Walker M, Thomas M, Alberti KGMM (2002) Biochemical measures in a population based study: the effect of fasting duration and time of day. Ann Clin Biochem 39:493–501
Whincup PH, Bruce NG, Cook DG, Shaper AG (1992) The Dinamap 1846SX automated blood pressure recorder: comparison with the Hawksley random zero sphygmomanometer under field conditions. J Epidemiol Comm Health 46:164–169
Bruce NG, Cook DG, Shaper AG (1990) Differences between observers in blood pressure measurement with an automatic oscillometric recorder. J Hypertens Suppl 8:S11–S13
Trinder P (1969) Determination of blood glucose in blood using glucose oxidase with an alternative oxygen acceptor. Ann Clin Biochem 6:24–27
Andersen L, Dinesen B, Jorgensen PN, Poulsen F, Roder ME (1993) Enzyme immunoassay for intact human insulin in serum or plasma. Clin Chem 39:578–582
Bonora E, Targher G, Alberiche M, Bonadonna RC, Saggiana F, Zenere MB (2000) Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity. Diabetes Care 23:57–63
Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (2001) Executive summary of the Third Report of the National Cholesterol Education Program (NCEP). Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 385:2486–2497
Danesh J, Collins R, Peto R, Lowe GDO (2000) Haematocrit, viscosity, erythrocyte sedimentation rate: meta-analyses of prospective studies of coronary heart disease. Eur Heart J 21:515–520
Pouliot MC, Despres JP, Lemieux S et al. (1994) Waist circumference and abdominal saggital diameter: best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am J Cardiol 73:460–468
Seligman BGS, Gross JL, Biolo A, Clausell NC, Polanczyk CA (2000) Increased plasma levels of endothelin 1 and von Willebrand Factor in patients with type 2 diabetes and dyslipidemia. Diabetes Care 23:1395–1400
Danesh J, Collins R, Appleby P et al. (1998) Association of fibrinogen, C-reactive protein, albumin or leukocyte count with coronary heart disease: meta-analyses of prospective studies. JAMA 279:1477–1482
Danesh J, Whincup P, Walker M et al. (2001) Fibrin D-dimer and coronary heart disease: prospective study and meta-analysis. Circulation 103:2323–2327
Whincup PH, Danesh J, Walker M et al. (2002) Von Willebrand factor and coronary heart disease: prospective study and meta-analysis. Eur Heart J 23:1764–1770
Lowe GDO, Danesh J, Lewington S et al. (2004) Tissue plasminogen activator antigen and coronary heart disease: prospective study and meta-analysis. Eur Heart J 25:252–259
Jager A, van Hinsbergh VWM, Kostense PJ et al. (1999) von Willebrand Factor, C-reactive protein, and 5 year mortality in diabetic and non-diabetic subjects: the Hoorn Study. Arterioscler Thromb Vasc Biol 19:3071–3078
Lowe GDO (2001) Factor IX and thrombosis. Br J Haematol 115:507–513
Lowe GDO, Haverkate F, Thompson SG et al., on behalf of the ECAT DVT Study Group (1999) Prediction of deep vein thrombosis after elective hip replacement surgery by preoperative clinical and hemostatic variables: the ECAT DVT Study. Thromb Haemostas 81:879–886
Saito I, Folsom AR, Brancati FL, Duncan BB, Chambless LE, McGovern PG (2000) Non-traditional risk factors for coronary heart disease incidence among persons with diabetes: the Atherosclerotic Risk in Communities (ARIC) Study. Ann Intern Med 133:81–91
Matsumoto K, Sera Y, Abe Y, Ueka Y, Tominaga T, Miyake S (2003) Inflammation and insulin resistance are independently related to all-cause death and cardiovascular events in Japanese patients with type 2 diabetes. Atherosclerosis 169:317–321
Lowe GDO, Yarnell JWG, Rumley A, Bainton D, Sweetnam PM (2001) C-reactive protein, fibrin D-dimer, and incident ischemic heart disease in the Speedwell Study. Are inflammation and fibrin turnover linked in pathogenesis? Arterioscler Thromb Vasc Biol 21:603–610
Wiman B, Andersson T, Hallqvist J, Reuterwall C, Ahlbom A, deFaire U (2000) Plasma levels of tissue plasminogen activator/plasminogen activator inhibitor-1 complex and von-Willebrand factor are significant risk markers for recurrent myocardial infarction in the Stockholm Heart Epidemiology Program (SHEEP) study. Arterioscl Thromb Vasc Biol 20:2019–2023
De Bono D (1994) Significance of raised plasma concentrations of tissue-type plasminogen activator and plasminogen activator inhibitor in patients at risk from ischaemic heart disease. Br Heart J 71:504–507
Haffner SM, Valdez RA, Hazuda HP et al. (1992) Prospective analysis of the insulin resistance syndrome (syndrome X). Diabetes 41:715–722
Haffner SM, D’Agostino R Jr, Festa A et al. (2003) Low insulin sensitivity (Si=0) in diabetic and nondiabetic subjects in the Insulin Resistance Atherosclerosis Study: is it associated with components of the metabolic syndrome and nontraditional risk factors? Diabetes Care 26:2796–2803
Bonora E, Perbellini S, Formentini G et al. (2002) HOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in Type 2 diabetic subjects. Diabetes Care 25:1135–1141
Lehto S, Ronnemaa T, Pyorala K, Laakso M (2000) Cardiovascular risk factors clustering with endogenous hyperinsulinaemia predict death from coronary heart disease in patients with type 2 diabetes. Diabetologia 43:148–155
DeFronzo RA, Tobin JD, Andres R (1979) The glucose clamp technique: a method for the quantification of beta cell sensitivity to glucose and tissue sensitivity to insulin. Am J Physiol 237:E214–E223
UK Prospective Diabetes Study (UKPDS) Group (1998) Effect of intensive blood-glucose control with metformin on complications in overweight patients with Type 2 diabetes (UKPDS 34). Lancet 352:854–865
Acknowledgements
The British Regional Heart Study is a British Heart Foundation Research Group and is supported by the Department of Health, UK. The measurements and laboratory analyses reported here were supported by British Heart Foundation Project Grants PG97012 and PG97027. The views expressed in this publication are those of the authors and not necessarily those of the Department of Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wannamethee, S.G., Lowe, G.D.O., Shaper, A.G. et al. Insulin resistance, haemostatic and inflammatory markers and coronary heart disease risk factors in Type 2 diabetic men with and without coronary heart disease. Diabetologia 47, 1557–1565 (2004). https://doi.org/10.1007/s00125-004-1491-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-004-1491-7