
Abstract
Recently, the detection of occult cancer cells in peripheral blood has received a great deal of attention regarding the prediction of postoperative cancer recurrence and for novel strategies of adjuvant therapy. The aim of this study was to establish a new molecular diagnostic method of detecting circulating tumor cells. Gastric cancer SGC-7901 cells in 2 ml blood from healthy volunteers were serially diluted. Additional peripheral blood samples were collected from 90 patients and 27 healthy volunteers. Real-time reverse transcription-polymerase chain reaction was used to detect the levels of microRNA-106a (miR-106a) and microRNA-17 (miR-17). Receiver operating characteristics (ROC) curves were constructed. In recovery experiments, a significant correlation between the number of cancer cells and the levels of both miR-106a (r = −0.906, p = 0.037) and miR-17 (r = −0.912, p = 0.031) was found. In preoperative and postoperative patient groups, miR-106a and miR-17 levels were significantly higher than those in controls. The areas under the ROC curve for miR-106a, miR-17, and combination were 0.684 (p = 0.0066), 0.743 (p = 0.0001), and 0.741 (p = 0.0002), respectively. Our results indicate that the detection of miRNA in peripheral blood may be a novel tool for monitoring circulating tumor cells in patients with gastric cancers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
MicroRNAs (miRNAs) are non-coding RNAs that regulate the expression of target mRNAs [1]. They are encoded by genes that are transcribed into single or clustered primary transcripts, which are processed to produce the mature miRNAs. miRNAs play important roles in the control of many biological processes, such as cellular development, differentiation, proliferation, apoptosis, and metabolism [2–4]. Overexpressed or underexpressed miRNAs in cancers may function as oncogenes or tumor suppressor genes, respectively. Since Calin et al. reported a connection between miR-15/miR-16 and B-cell chronic lymphocytic leukemia, more studies have shown the importance of miRNAs in the initiation, progression, and prognosis of numerous cancers [5].
Gastric cancer is the second leading cause of cancer death in the world and will likely remain as one of the leading causes of all deaths in the near future [6]. However, for the diagnosis of gastric cancer, few highly sensitive or highly specific tumor markers are available. The findings of miRNAs suggest ideal diagnostic markers. Bandres et al. reported that the expression of miR-451 was reduced in gastric and colorectal cancer versus noncancerous tissues [7]. Overexpression of miR-451 in gastric and colorectal cancer cells reduced cell proliferation and increased sensitivity to radiotherapy [7]. Jiang et al. found that miR-421 may involve in the early stage of stomach carcinogenesis and could be used as an efficient diagnostic biomarker [8].
miRNA-106a (miR-106a), a member of the miR-106a-92 cluster located at Xq26.2, has oncogenic activity in humans and often shows altered expression [9]. miRNA-17 (miR-17), a member of the miR-17-92 cluster located at 13q31.3, demonstrates oncogene activity [10]. In fact, the miR-17-92, miR-106b-25, and miR-106a-92 clusters show high homology in their gene structures and have oncogenic potential [11–13]. In our previous studies, we found that miR-106a and miR-17 were overexpressed in gastric cancer compared with noncancerous tissue [14]. Moreover, we found that miR-106a levels were associated significantly with tumor stage, size and differentiation, lymphatic and distant metastasis, and invasion [11].
Recently, the detection of occult cancer cells in peripheral blood or bone marrow has received attention regarding prediction of the postoperative recurrence of cancer and for novel strategies of adjuvant therapy [15]. The objective of the present study was to examine the usefulness of miR-106a or miR-17 in peripheral blood as a marker for the diagnosis of gastric cancers.
Materials and methods
Patients and specimens
Two-milliliter peripheral blood samples were collected from 90 patients (63 male, 27 female; 62.3 ± 9.8 and 59.2 ± 11.8 years old, respectively) with gastric cancer from May 2008 to December 2009 at Ningbo No. 1, No. 2, and No. 3 Hospitals, China. Of the patients, 41 were preoperative and the rest were postoperative, most of which were within 3 weeks of surgery. Peripheral blood samples from 27 healthy volunteers were used as controls. Informed consent was obtained from all subjects, and the Human Research Ethics Committee in Ningbo University approved all aspects of the study. Tumors were staged using the tumor-node metastasis staging of the International Union Against Cancer [16]. Histological grade was assessed according to the World Health Organization criteria [17].
Cell culture
The human gastric cancer cell line, SGC-7901, was obtained from the Shanghai Institute of Biochemistry and Cell Biology, Chinese Academy of Sciences (Shanghai, China). Cells were cultured in culture flasks at 37°C in a humidified atmosphere of 5% CO2 with RPMI-1640 Medium (Life Technologies, Grand Island, NY) containing 10% fetal calf serum with 50 U/ml penicillin and 50 μg/ml streptomycin. Exponentially growing cells were used for experiments. Cells were counted using a hemocytometer.
Recovery experiment
SGC-7901 cells were diluted in 2 ml of blood obtained from healthy volunteers. The number of cancer cells used in the recovery experiments was 100, 101, 102, 104, and 106, respectively.
Total RNA preparation
Mononuclear cells (MNCs) were collected from peripheral blood (patients and recovery experiment) using a Ficoll solution (Shanghai Hengxin Chemical Reagents Company Ltd., Shanghai, China) following the manufacturer’s instruction. Total RNA from MNCs was isolated using Trizol reagent (Invitrogen, Karlsruhe, Germany) following the manufacturer’s protocol. The total RNA was dissolved in 10 μl diethypyrocarbonate-treated water.
Reverse transcription
cDNA was generated using the miScript Reverse Transcription (RT) Kit (Qiagen GmbH, Hilden, Germany), according to the manufacturer’s instructions. Four microliter total RNA, 1 μl miScript Reverse Transcriptase Mix, and 4 μl miScript RT buffer were mixed and incubated for 60 min at 37°C. Then, 80-μl autoclaved-distilled water was added to the reverse transcription product.
Real-time polymerase chain reaction for detection of miR-106a and miR-17
Real-time polymerase chain reaction (PCR) was performed using the miScript SYBR Green PCR Kit (Qiagen) on an Mx3005P QPCR System (Stratagene, La Jolla, CA). The 20 μl PCR mixture included 6 μl reverse transcription product, 10 μl 2× QuantiTect SYBR Green PCR Master Mix, 1 μl 10× miScript Universal Primer, 1 μl 10× miScript Primer Assay (for miR-106a and miR-17; Qiagen), and 2 μl autoclaved-distilled water. The reaction mixtures were incubated at 95°C for 15 min, followed by 40 amplification cycles of 94°C for 15 s, 60°C for 30 s, and 70°C for 30 s. The threshold cycle (Ct) was defined as the fractional cycle number at which the fluorescence passed the fixed threshold. We also quantified transcripts of U6 small RNA using the Hs_RNU6B_2 miScript Primer Assay (Qiagen) for normalizing the levels of miR-106a and miR-17.
The ΔCt method was used for analysis [11]. Firstly, the Ct for each sample was determined. Next, the ΔCt value was calculated. The ΔCt value was the difference between the Ct value of miR-106a or miR-17 and the Ct value of U6. The ΔΔCt value and the normalized miR-106a or miR-17 expression were calculated, respectively. We used a cutoff value of 2.00, with samples having a 2−ΔΔCt value >2.00 considered positive [18]. The experiment was repeated twice. The investigators were blinded to the results of clinical and pathological diagnosis.
Calculation of PCR efficiency
Total RNA isolated from SGC-7901 cells was serially diluted to 100, 50, 25, 12.5, and 6.25 μg/ml, respectively. The RNA was transcribed into cDNA, and miR-106a and miR-17 were amplified. Finally, the linear relationships between the log concentrations of template RNA and Ct values were analyzed.
PCR-specific assay
To determine the PCR specificity, the amplicon size was determined by agarose gel and then by dissociation curve analysis. The PCR products were separated on a 1.5% agarose gel stained with ethidium bromide at 4 V/cm for 2 h. DNA fragments were observed using the Gel Image Analysis System (Bio-Rad, Hercules, CA). Dissociation curve analysis was carried out using a Mx3005P QPCR System (Stratagene) according to the manufacturer’s instruction.
Immunohistochemistry experiment
Cytokeratin (CK) is expressed in epithelial cells, and CK18 and CK20 are commonly used tumor markers of gastric cancer [19]. To demonstrate that the blood used to prepare the sample for RT-PCR analysis contained circulating tumor cells (CTCs) and spiked SGC-7901 cells, immunohistochemistry was performed using CK18 and CK20 monoclonal antibodies as markers of gastric cancer cells. MNCs collected by Ficoll solution from healthy volunteers, spiked with SGC-7901 cells, or gastric cancer patients were smeared on slides. After incubating with monoclonal antibody CK18 or CK20 (Maixin Biotechnology Co., Fujian, China) for an hour, followed by goat antibody mouse immunoglobulin G polymerid (Maixin) for 15 min at room temperature, the cancer cells were visualized using the 3,3′-diaminobenzidine Horseradish Peroxidase Color Development Kit (Maixin). Finally, cells were post-stained by hematoxylin (Maixin) and observed under microscopy.
Statistical analysis
Statistical analysis was performed using the Statistical Program for Social Sciences (SPSS) software 17.0 (SPSS Inc., Chicago, IL). The correlations in recovery experiment and calculation of PCR efficiency were analyzed by Spearman correlation analysis. The level of significance was set at p < 0.05.
ROC curves were constructed by calculating the sensitivities and specificities of a biomarker or the diagnostic score of a logistic regression model at different cutoff points for differentiating gastric cancer cases from healthy volunteers. The area under the ROC curves (AUC) can be statistically interpreted as the probability to correctly distinguish patients with gastric cancer from normal subjects. The p value is the probability that the sample AUC is found when, in fact, the true (population) AUC is 0.5 (null hypothesis: Area = 0.5). If p is low (p < 0.05), then it can be concluded that the AUC is significantly different from 0.5 and that the laboratory test is able to distinguish between the two groups [20]. The cutoff value corresponds to the optimal diagnostic accuracy (the highest sum of the respective values for sensitivity and specificity) [20]. To observe the diagnostic value of the combinative use of miR-106a and miR-17, the logistic regression analysis was used. The AUCs of miR-106a, miR-17, and combination were compared through Student’s t test.
Results
Recovery experiments
To establish a reliable method for detecting circulating tumor cells, recovery experiments were performed. We found a significant correlation between the number of cancer cells spiked and the values of both miR-106a (r = −0.906, p = 0.037; Fig. 1a) and miR-17 (r = −0.912, p = 0.031; Fig. 1b).

The relative expression of miR-106a (a) and miR-17 (b) in healthy blood spiked with gastric cancer SGC-7901 cells. Values (ΔCt) are relative to those of U6 small RNA in the same samples. r = −0.906, p = 0.037 (a); r = −0.912, p = 0.031 (b). Spearman correlation analysis
Levels of miR-106a and miR-17 in peripheral blood from patients with gastric cancer were higher than those from healthy volunteers
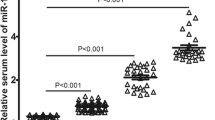
Levels of miR-106a and miR-17 in peripheral blood from preoperative (n = 41) and postoperative (n = 49) patients with gastric cancer were compared to those from healthy volunteers (n = 27). We found that miR-106a levels in preoperative patients (p = 0.006, Fig. 2a) and postoperative patients (p = 0.016, Fig. 2b) were higher than those in control; miR-17 levels in preoperative patients (p = 0.001, Fig. 3a) and postoperative patients (p = 0.019, Fig. 3b) were also higher than those in control. The average increase of miR-106a and miR-17 in preoperative patients was 37.324-fold and 36.950-fold, respectively, and those in postoperative patients were 9.341- and 13.698-fold, respectively. If samples having a 2−ΔΔCt value >2.00 were considered as positive [18], the positive detection rates of miR-106a and miR-17 in preoperative patients were 56.10% and 58.54%, respectively.

Levels of miR-106a in mononuclear cells from preoperative (n = 41) (a) and postoperative (n = 49) (b) patients with gastric cancer were higher than those from healthy volunteers (n = 27). Patients vs control, p = 0.006 (a); p = 0.016 (b)

Level of miR-17 expression in mononuclear cells from preoperative (n = 41) (a) and postoperative (n = 49) (b) patients with gastric cancer were higher than those from healthy volunteers (n = 27). Patients vs control, p = 0.001 (a); p = 0.019 (b)
PCR efficiency
To calculate the efficiency of PCR, serially diluted RNA from SGC-7901 was used. Significant correlations between the RNA used and Ct values of both miR-106a (r = −0.930, p = 0.022; Fig. 4a) and miR-17 (r = −0.956, p = 0.011; Fig. 4b) were found.

The correlation between the RNA from SGC-7901 and Ct values of both miR-106a (a) and miR-17 (b). r = −0.930, p = 0.022 (a); r = −0.956, p = 0.011 (b). Spearman correlation analysis
PCR specificity
To make sure the PCR products were correct, the PCR amplicons were tested by agarose gel electrophoresis. The results showed that the sizes of the miR-106a and miR-17 PCR products were 85 bp each and that of the U6 PCR products was 100 bp (Fig. 5), which are in accord with the manufacturer’s protocol. The dissociation curve analysis showed that there was only one peak at the highest T m in each dissociation curve (Fig. 6a–c). These results indicate that there were no primer–dimers or nonspecific products.

Agarose gel electrophoresis analysis of PCR products. The sizes of miR-106a and miR-17 PCR products were 85 bp each and that of U6 PCR products was 100 bp. 1–3 different patient samples; 4 no RNA template control

Dissociation curves analysis of miR-106a (a), miR-17 (b), and U6 (c) RT-PCR products. 1–3 three blood samples from patients with gastric cancer
Immunohistochemistry experiment
To evaluate whether the fraction of blood used to prepare the sample for PCR analysis contained circulating tumor cells and spiked SGC-7901 cells, immunohistochemistry was performed used CK18 and CK20 as tumor markers. The results show that the cytoplasm of cancer cells had immunohistochemical reaction product (Fig. 7a–f) in both the recovery experiment and patient samples.

A representative result of immunohistochemistry for detecting gastric cancer cells. a–d CK20 was used as a tumor marker to detect MNCs from healthy volunteers’ peripheral blood (a), SGC-7901 cells (b), healthy volunteers’ peripheral blood spiked with SGC-7901 cells (c), and peripheral blood from patients (d). e, f CK18 was used as a tumor marker to detect MNCs from SGC-7901 cells (e) and healthy volunteers’ peripheral blood spiked with SGC-7901 cells (f). Arrows indicate cancer cells (×400)
The diagnostic efficacy of miR-106a or miR-17 in the detecting CTCs in patients with gastric cancer
To evaluate the diagnostic value of miR-106a or miR-17 in the diagnosis of patients with gastric cancer, the AUC value from ROC curve analysis was determined (Fig. 8). The AUC of miR-106a was 0.684 ± 0.068 (p = 0.0066), the 95% confidence interval was 0.560 to 0.791, the criterion value (cutoff value) was 6.535 with a sensitivity of 48.15%, and the specificity was 90.24%. The AUC of miR-17 was 0.743 ± 0.064 (p = 0.0001), the 95% confidence interval was 0.622 to 0.841, the criterion value (cutoff value) was 6.190 with a sensitivity of 51.85%, and the specificity was 92.68%.

Receiver operation characteristics (ROC) curve of the miR-106a, miR-17, and combination in peripheral blood mononuclear cells (MNCs). The clinical values were assessed by differentiating 41 preoperative gastric cancer patients from 27 healthy volunteers. The AUC of miR-106a, miR-17 and combination are \( 0.{684}\pm 0.0{68}\,\,\left( {p = 0.00{66}} \right) \), \( 0.{743}\pm 0.0{64}\,\,\left( {p = 0.000{1}} \right) \), and \( 0.{741}\pm 0.0{64}\,\,\left( {p = 0.000{2}} \right) \), respectively
The AUC of the combinative use of miR-106a and miR-17 was 0.741 ± 0.064 (p = 0.0002), the 95% confidence interval was 0.620 to 0.839, the criterion value (cutoff value) was 0.4916 with a sensitivity of 62.96%, and the specificity was 80.49%.
The pairwise comparisons of ROC curves showed that there were no significant difference between AUCs of miR-106a and miR-17 (p = 0.114), miR-106a and combination (p = 0.278), miR-17 and combination (p = 0.087), respectively.
Discussion
Human cancers commonly exhibit an altered expression profile of miRNAs with oncogenic (miR-21, miR-106a, and miR-155) or tumor-suppressive (let-7, miR-15a/16, miR-34a, and miR-143/145) activity [9]. In the present study, we focused on the miR-106a and miR-17 expression patterns in peripheral blood from patients with gastric cancer. The levels in the cancer groups were found to be significantly higher than those in the healthy-volunteer group (Figs. 2 and 3). The mean expression levels of miR-106a and miR-17 in preoperative patients were higher than those in postoperative patients. These results show that surgery and other treatment may have an effect on the levels of miRNAs in peripheral blood.
Many studies have shown that miR-106a and miR-17 are upregulated in various tumors. In colon adenocarcinoma, Schetter et al. showed that the expression of miR-106a and four other miRNAs were increased [21]. In comparison with the vehicle-treated cells (16HBE-N), human bronchial epithelial cells (16HBE-T) exhibited differential expression of 54 miRNAs, in which miR-106a and miR-17 were highly expressed [22]. Hayashita et al. showed for the first time that the miR-17-92 cluster is markedly and frequently overexpressed in lung cancers, with occasional gene amplification, especially in cases with small-cell lung cancer histology [10]. The expression of miR-106a and miR-17 was found to associate with the occurrence and development of tumors. Busacca et al. investigated the expression of miR-106a between mesothelioma and mesothelial cells and found that its expression was associated significantly with the histopathological subtype [23]. Diaz et al. found that deregulated expression of miR-106a predicts survival in human colon cancer patients [24]. Northcott et al. reported that miR-17-92 is a positive effector of sonic hedgehog (Shh)-mediated proliferation and that aberrant expression or amplification of this miRNA confers a growth advantage to medulloblastomas [25].
Noninvasive tests are a trend for disease diagnosis. Recently, serum and plasma miRNAs were identified as stable blood-based markers for cancer detection. Chim et al. first detected placental miRNAs in maternal plasma and found that the expression levels of 17 miRNAs were higher in placentas than those in maternal blood cells [26]. Using high-density microarray, Lodes et al. discovered that miRNA expression patterns in serum were not identical to those seen from miRNAs taken directly from cancer cell lines [27]. They suggested that tumor cell lysis may be the most obvious source of serum or plasma miRNAs. However, the product of a form of active transport involving the formation of exosomes also may be the source of miRNAs [27].
In the present study, we focused on detecting the miRNAs from CTCs. The difference between an investigation of miRNAs in serum or plasma and in peripheral blood MNCs is that the source of the latter is only from living cells. From a clinical point of view, the detection of CTCs may aid the prognosis and decisions regarding therapeutic decisions for cancer patients. The presence of tumor cells in circulation may be a prognostic indicator of recurrence and metastatic disease [28]. The main cause of tumor recurrence is thought to be the presence of micrometastases, which are currently undetectable by conventional methods [29, 30]. Tumor-specific mRNAs, such as CK19, CK20, carcinoembryonic antigen, and α fetoprotein mRNAs, have been used as biomarkers for the detecting CTCs [15, 31, 32]. However, some markers are not only poorly expressed in some kinds of CTCs but are also expressed in hematopoietic cells [33, 34]. miRNA expression profiling may hold more promise than mRNA profiling for discriminating between tumor types [35]. The detection of miRNAs in CTCs may be a better choice. The results of our recovery experiments, which show a significant correlation between the number of cancer cells and the level of miR-106a (Fig. 1a) and miR-17 (Fig. 1b), and the significant ROC curves (Fig. 8) confirm this speculation.
In all of the data, it seems that miR-17 outperformed miR-106a (Figs. 1, 2, 3, 4). Among miR-106a, miR-17, and the combination, the largest AUC was observed when miR-17 was used alone (Fig. 8). However, there was no significant difference among the AUCs of miR-106a, miR-17, and the combination (p > 0.05). The results did not complement each other across the patient base. These results indicated that miR-106a and miR-17 had the similar diagnostic value. The combination was superior to miR-106a and miR-17 alone regarding the sensitivity, but not the specificity values. As miR-106a and miR-17 show high homology in their gene structures [11–13], they may play some similar roles in the carcinogenesis of gastric cancer. As a result, AUC of the ROC is not significantly improved by using both of miR-106a and miR-17.
In summary, the levels of miR-106a and miR-17 in peripheral blood MNCs from patients with gastric cancer were significantly higher than those from healthy volunteers. The higher levels of miR-106a and miR-17 indicate that there are tumor cells in the peripheral blood from patents with gastric cancer.
References
Ambros V (2003) MicroRNA pathways in flies and worms: growth, death, fat, stress, and timing. Cell 113:673–676
He L, Hannon GJ (2004) MicroRNAs: small RNAs with a big role in gene regulation. Nat Rev Genet 5:522–531
Kloosterman WP, Plasterk RH (2006) The diverse functions of microRNAs in animal development and disease. Dev Cell 11:441–450
Perera RJ, Ray A (2007) MicroRNAs in the search for understanding human diseases. BioDrugs 21:97–104
Calin GA, Dumitru CD, Shimizu M, Bichi R, Zupo S, Noch E, Aldler H, Rattan S, Keating M, Rai K et al (2002) Frequent deletions and down-regulation of micro- RNA genes miR15 and miR16 at 13q14 in chronic lymphocytic leukemia. Proc Natl Acad Sci U S A 99:15524–15529
Murray CJ, Lopez AD (1997) Alternative projections of mortality and disability by cause 1990-2020: global burden of disease study. Lancet 349:1498–1504
Bandres E, Bitarte N, Arias F, Agorreta J, Fortes P, Agirre X, Zarate R, Diaz-Gonzalez JA, Ramirez N, Sola JJ et al (2009) microRNA-451 regulates macrophage migration inhibitory factor production and proliferation of gastrointestinal cancer cells. Clin Cancer Res 15:2281–2290
Jiang Z, Guo J, Xiao B, Miao Y, Huang R, Li D, Zhang Y (2010) Increased expression of miR-421 in human gastric carcinoma and its clinical association. J Gastroenterol 45:17–23
Tong AW, Nemunaitis J (2008) Modulation of miRNA activity in human cancer: a new paradigm for cancer gene therapy? Cancer Gene Ther 15:341–355
Hayashita Y, Osada H, Tatematsu Y, Yamada H, Yanagisawa K, Tomida S, Yatabe Y, Kawahara K, Sekido Y, Takahashi T (2005) A polycistronic microRNA cluster, miR-17-92, is overexpressed in human lung cancers and enhances cell proliferation. Cancer Res 65:9628–9632
Xiao B, Guo J, Miao Y, Jiang Z, Huan R, Zhang Y, Li D, Zhong J (2009) Detection of miR-106a in gastric carcinoma and its clinical significance. Clin Chim Acta 400:97–102
Petrocca F, Visone R, Onelli MR, Shah MH, Nicoloso MS, de Martino I, Iliopoulos D, Pilozzi E, Liu CG, Negrini M et al (2008) E2F1-regulated microRNAs impair TGFbeta-dependent cell-cycle arrest and apoptosis in gastric cancer. Cancer Cell 13:272–286
Landais S, Landry S, Legault P, Rassart E (2007) Oncogenic potential of the miR-106-363 cluster and its implication in human T-cell leukemia. Cancer Res 67:5699–5707
Guo J, Miao Y, Xiao B, Huan R, Jiang Z, Meng D, Wang Y (2009) Differential expression of microRNA species in human gastric cancer versus non-tumorous tissues. J Gastroenterol Hepatol 24:652–657
Koga T, Tokunaga E, Sumiyoshi Y, Oki E, Oda S, Takahashi I, Kakeji Y, Baba H, Maehara Y (2008) Detection of circulating gastric cancer cells in peripheral blood using real time quantitative RT-PCR. Hepatogastroenterology 55:1131–1135
Sobin LH, Wittekind C (1997) International Union against Cancer. TNM classification of malignant tumours, 5th edn. Wiley, New York, pp 59–62
Solcia E, Klöppel G, Sobin L, Williams E (2000) Endocrine tumours of the gastrointestinal tract. In: Solcia E (ed) Histological typing of endocrine tumours. Springer, Heidelberg, pp 61–68
Markou A, Tsaroucha EG, Kaklamanis L, Fotinou M, Georgoulias V, Lianidou ES (2008) Prognostic value of mature microRNA-21 and microRNA-205 overexpression in non-small cell lung cancer by quantitative real-time RT-PCR. Clin Chem 54:1696–1704
Kim MA, Lee HS, Yang HK, Kim WH (2004) Cytokeratin expression profile in gastric carcinomas. Hum Pathol 35:576–581
Bachtiar I, Santoso JM, Atmanegara B, Gani RA, Hasan I, Lesmana LA, Sulaiman A, Gu J, Tai S (2009) Combination of alpha-1-acid glycoprotein and alpha-fetoprotein as an improved diagnostic tool for hepatocellular carcinoma. Clin Chim Acta 399:97–101
Schetter AJ, Leung SY, Sohn JJ, Zanetti KA, Bowman ED, Yanaihara N, Yuen ST, Chan TL, Kwong DL, Au GK et al (2008) MicroRNA expression profiles associated with prognosis and therapeutic outcome in colon adenocarcinoma. JAMA 299:425–436
Shen YL, Jiang YG, Greenlee AR, Zhou LL, Liu LH (2009) MicroRNA expression profiles and miR-10a target in anti-benzo[a] pyrene-7, 8-diol-9, 10-epoxide-transformed human 16HBE cells. Biomed Environ Sci 22:14–21
Busacca S, Germano S, De Cecco L, Rinaldi M, Comoglio F, Favero F, Murer B, Mutti L, Pierotti M, Gaudino G (2009) MicroRNA Signature of Malignant Mesothelioma with Potential Diagnostic and Prognostic Implications. Am J Respir Cell Mol Biol. doi:10.1165/rcmb.2009-0060OC
Diaz R, Silva J, Garcia JM, Lorenzo Y, Garcia V, Pena C, Rodriguez R, Munoz C, Garcia F, Bonilla F et al (2008) Deregulated expression of miR-106a predicts survival in human colon cancer patients. Genes Chromosomes Cancer 47:794–802
Northcott PA, Fernandez LA, Hagan JP, Ellison DW, Grajkowska W, Gillespie Y, Grundy R, Van Meter T, Rutka JT, Croce CM et al (2009) The miR-17/92 polycistron is up-regulated in sonic hedgehog-driven medulloblastomas and induced by N-myc in sonic hedgehog-treated cerebellar neural precursors. Cancer Res 69:3249–3255
Chim SS, Shing TK, Hung EC, Leung TY, Lau TK, Chiu RW, Lo YM (2008) Detection and characterization of placental microRNAs in maternal plasma. Clin Chem 54:482–490
Lodes MJ, Caraballo M, Suciu D, Munro S, Kumar A, Anderson B (2009) Detection of cancer with serum miRNAs on an oligonucleotide microarray. PLoS ONE 4:e6229
White H, Griffiths JD (1976) Circulating malignant cells and fibrinolysis during resection of colorectal cancer. Proc R Soc Med 69:467–469
Ghossein RA, Rosai J (1996) Polymerase chain reaction in the detection of micrometastases and circulating tumor cells. Cancer 78:10–16
Pelkey TJ, Frierson HF Jr, Bruns DE (1996) Molecular and immunological detection of circulating tumor cells and micrometastases from solid tumors. Clin Chem 42:1369–1381
Guo J, Xiao B, Zhang X, Jin Z, Chen J, Qin L, Mao X, Shen G, Chen H, Liu Z (2004) Combined use of positive and negative immunomagnetic isolation followed by real-time RT-PCR for detection of the circulating tumor cells in patients with colorectal cancers. J Mol Med 82:768–774
Guo J, Yao F, Lou Y, Xu C, Xiao B, Zhou W, Chen J, Hu Y, Liu Z (2007) Detecting carcinoma cells in peripheral blood of patients with hepatocellular carcinoma by immunomagnetic beads and rt-PCR. J Clin Gastroenterol 41:783–788
Lambrechts AC, van 't Veer LJ, Rodenhuis S (1998) The detection of minimal numbers of contaminating epithelial tumor cells in blood or bone marrow: use, limitations and future of RNA-based methods. Ann Oncol 9:1269–1276
Vlems FA, Diepstra JH, Cornelissen IM, Ruers TJ, Ligtenberg MJ, Punt CJ, van Krieken JH, Wobbes T, van Muijen GN (2002) Limitations of cytokeratin 20 RT-PCR to detect disseminated tumour cells in blood and bone marrow of patients with colorectal cancer: expression in controls and downregulation in tumour tissue. Mol Pathol 55:156–163
Nelson KM, Weiss GJ (2008) MicroRNAs and cancer: past, present, and potential future. Mol Cancer Ther 7:3655–3660
Acknowledgments
This work was supported by the Ningbo Natural Science Foundation (Nos. 2009A610134, 201001A6010002, 201001A6010003), Zhejiang Province Research Project (Nos. 2008C33020 and 2008F70052), Natural Science Foundation of Zhejiang Province (Nos. Y207240 and Y207244), National Natural Science Foundation of China (No. 30872420), Post-graduate Innovative Research Project in Zhejiang Province (No. YK2008046), and K. C. Wong Magna Fund in Ningbo University.
Disclosure of potential conflict of interests
The authors declare that they have no conflicting interests related to this study.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Zhou, H., Guo, JM., Lou, YR. et al. Detection of circulating tumor cells in peripheral blood from patients with gastric cancer using microRNA as a marker. J Mol Med 88, 709–717 (2010). https://doi.org/10.1007/s00109-010-0617-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00109-010-0617-2