
Abstract
Immunologic tolerance is a state of unresponsiveness that is specific for a particular antigen. The immune system has an extraordinary potential for making T cell and B cell that recognize and neutralize any chemical entity and microbe entering the body. Certainly, some of these T cells and B cells recognize self-components; therefore, cellular mechanisms have evolved to control the activity of these self-reactive cells and achieve immunological self-tolerance. The most important in vivo biological significance of mechanisms regulating self-tolerance is to prevent the immune system from mounting an attack against the host’s own tissues resulting in autoimmunity. This review summarizes recent developments in our understanding of T-helper cell tolerance and discusses how the new findings can be exploited to prevent and treat autoimmune diseases, allergy, cancer, and chronic infection, or establish donor-specific transplantation tolerance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Central tolerance
One of the most remarkable properties of the immune system is its ability to recognize, respond to, and eliminate foreign (nonself) antigens while not reacting harmfully to that individual’s own (self) antigenic substances. This state of immunologic unresponsiveness to antigens is also called tolerance. Self-tolerance is maintained by various mechanisms that prevent the maturation and activation of potentially self-reactive lymphocytes. The primary mechanism of immunological self-tolerance is central deletion in which self-reactive T cells are deleted in the thymus during T cell maturation by negative selection [1]. Many recent studies suggest that T cell receptor (TCR) editing may play a role in controlling the development of self-reactive T cells in thymus [2] as well. TCRs are selected to recognize a composite ligand comprising peptide fragments of antigen bound to major histocompatibility complex (MHC) molecules. Composites of self-peptides and MHC are displayed on the surface of cortical thymic epithelial cells, and CD4+CD8+ thymocyte expression of TCRs that weakly bind these ligands trigger maturation signals that inhibit RAG gene expression, thereby closing off the option of editing [3]. As a result, thymocytes are stimulated to survive. During this process, a minority of self-reactive TCRs triggers an editing process; in this case, TCRs are downregulated, RAG expression continues and the offending TCR α-chain is replaced or diluted with a second α-chain that is less self-reactive [2]. The majority of thymocytes whose receptors do not recognize self-MHC molecules are permitted to die. As positive selected thymocytes move from the cortex toward the medulla, they continue the maturation process and further test their TCRs for self-reactivity. TCRs that bind strongly to self-peptide/MHC combinations trigger the death (negative selection) of thymocytes. These medullary cells express T cell costimulatory molecules, such as CD80 and CD86, the ligands for CD28, and these costimulatory molecules play a crucial role in ensuring self-tolerance [4] (Fig. 1).

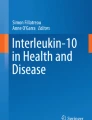
Pathways of central and peripheral tolerance. Hematopoietic precursors migrate to the thymus where they undergo positive and negative selection based on the nature of their TCR interactions with peptide/MHC. Self-reactive T cells with high affinity TCR are deleted at this stage, but others with low-affinity TCR escape in the periphery where they are controlled by mechanisms of peripheral tolerance acting either directly on the self-reactive T cell (T cell intrinsic) or indirectly via other cells (T cell extrinsic)
Recent studies on intrathymic expression of peripheral autoantigens, termed promiscuous gene expression, extends the scope of central T cell tolerance to peripheral organs and proves essential for the induction and maintenance of self-tolerance [3]. The finding of a causal relationship between the function of the transcriptional regulator autoimmune regulator (Aire) and the promiscuous expression of many peripheral antigens in murine medullary thymic epithelial cell (mTECs) was an important advancement. Anderson et al. [5, 6] showed that expression of many tissue-specific genes in mTECs is highly reduced in Aire knockout mice. Aire-deficient mice develop tissue-specific autoantibodies and lymphoid infiltration of several peripheral organs. Mutations of the Aire gene are associated with a multiorgan autoimmune syndrome known as autoimmune polyglandular syndrome type 1 [5, 6]. Partially deregulating promiscuous gene expression could lead to a breakdown of central tolerance, which also explain the pathophysiology of the human disease [3].
The molecular basis of thymocyte negative selection is still unclear. It was proposed that the serine–threonine kinase MINK (misshapen-Nck-interacting kinase-related kinase) selectively connects the TCR to a signaling pathway that mediates negative but not positive selection. MINK transcription is relatively low in CD4−CD8− thymocytes but is markedly higher in CD4+CD8+ thymocytes. Once thymocytes are positively selected, MINK expression declines. Knockdown MINK expression results in a double number of single positive thymocytes, which is consistent with a reduction in negative selection. However, decreasing MINK expression has no effect on positive selection. Essential function of MINK in the elimination of self-reactive thymocytes may be associated with downstream activation of Jun kinase and enhancement of expression of the proapoptotic molecule BIM, a member of the BH3-only proapoptotic subfamily of the BCL-2 family protein [7].
BIM is required for apoptosis of thymocytes in response to negative selection signals. Regulation of the apoptotic activity of BIM during negative selection is not understood. Initially it was observed that BIM expression at the messenger RNA and protein level was required at the negative selection pathway [4]. Recent studies by Bunin et al. suggest that strong TCR signals regulate the apoptotic activity of BIM by phosphorylation and subsequent changes in binding to Bcl-x (L) in immature thymocytes [8]. The tyrosine kinase ZAP70 (ζ-chain-associated protein kinase of 70 kDa) is required for thymocyte deletion because partial deficiency of ZAP70 in mice allows cells with forbidden TCRs to escape death and cause a systemic inflammatory disorder resembling rheumatoid arthritis [9]. Deletion also involves the induction of members of the Nur77 family of orphan nuclear receptors, and TCR-induced thymocytes death is blocked by a dominant negative Nur77 mutant [10]. It is interesting to note that recent studies suggest that HDAC7 (histone deacetylase 7), a key transcriptional regulator in several major developmental programs, regulates negative selection by repressing expression of Nur77 [11].
Peripheral tolerance
Although central tolerance is the major mechanism to eliminate self-reactive T cells, such deletion is incomplete. Indeed, healthy individuals were shown to harbor self-reactive T cells in the periphery. Therefore, the immune system has developed the mechanisms that deal with tolerance in the peripheral lymphoid organs, providing the necessary safety net to prevent autoimmunity. The mechanisms responsible for peripheral tolerance can be divided into those that regulate the responding state of T cell intrinsically, such as biochemical and gene-expression changes, and those that provide extrinsic controls, including limiting the supply of essential growth factors, costimuli, and proinflammatory mediators, and active suppression by regulatory T cells (Treg) (Fig. 1).
Mechanisms leading to intrinsic regulation of T cell tolerance
Inhibitory receptors
T cells that have exited the thymus remain capable of mounting responses to self-antigen; therefore, biochemical and genetic feedback loops are extremely important for fine tuning of autoreactive T cell responses. Inhibitory molecules expressed on T cells are essential for the maintenance of T cell homeostasis and self-tolerance. Expression levels of CD5, an inhibitory receptor able to recruit SHP1 [Src homology 2 (SH2)-domain-containing inositol-5-phosphatase] are dynamically adjusted on individual thymic and peripheral T cells in proportion to the strength of TCR self-reactivity, downregulating the response of TCRs to self-peptides to avoid T cell activation or deletion [12, 13].
CTLA-4 (cytotoxic T lymphocyte antigen 4) and PD-1 (programmed death-1) were recognized as two major coinhibitory receptors of the B7-CD28 family (Fig. 2). CTLA-4 is a well-characterized coinhibitory receptor. The strong inhibitory role of CTLA-4 is underscored by the phenotype of CTLA-4−/− mice, that is, the development of a massive accumulation of self-reactive T cells in peripheral lymphoid and nonlymphoid tissues [14, 15]. Major emphasis was recently placed on the evaluation of dynamic changes in CTLA-4 expression, uptake, trafficking, and degradation during T cell activation [16–19]. These careful analyses suggest that CTLA-4 has the potential to influence the activating threshold needed for a T cell to progress to full activation to mediate the attenuation of ongoing proliferative responses and to regulate the development of T-helper subset differentiation. Although the precise mechanism of CTLA-4 function is not clear, competition with CD28 for B7 molecules may have a critical role in mediating this outcome [1, 20, 21]. CTLA-4 polymorphisms appear to differentially influence its inhibitory activity. It is interesting to note that susceptibility to a variety of human autoimmune disorders was mapped to a noncoding 6.1-kb 3′ region of CTLA-4. Allelic variation in this region influenced mRNA levels and soluble alternative splice forms of human CTLA-4 [22]. This information, together with genetic data from diabetes and thyroiditis disease models, suggests that genetic difference in the context of CTLA-4 deficiency may contribute to the development of autoimmune disorders [23].

B7-1/B7-2:CD28/CTLA-4 superfamily members. CD28 family members are immunoglobulin superfamily members with a single immunoglobulin V-like domain. B7 family members are immunoglobulin superfamily members with immunoglobulin-V-like and immunoglobulin-C-like domains. CD28 and CTLA-4 have a MYPPPY motif that is essential for binding B7-1 and B7-2, whereas ICOS has a FDPPPF motif and binds ICOSL but not B7-1 and B7-2. PD-1 is a receptor for both PD-L1 and PD-L2 (which might also bind to other, and yet unidentified receptors on T cells)
PD-1 is expressed on activated T cells, B cells, and macrophages. In the presence of a TCR ligation by antigen, PD-1 recognition of its ligands B7-H1 results in the phosphorylation of the cytoplasmic ITIM (immunoreceptor tyrosine-based inhibition motif) and the subsequent generation of SHP-2-dependent negative signals [24–26]. The genetic loss of PD-1 leads to the development of autoimmune diseases with the genetic background influencing the severity and type of disease [27, 28]. It is important to note that polymorphisms in PD-1 have also recently been associated with susceptibility to systemic lupus erythematosus [29] type 1 diabetes [30].
In addition, a third member of coinhibitory receptors, B- and T-lymphocyte-attenuator (BTLA/CD272), which belongs to the CD28 immunoglobulin superfamily, was identified [31]. The cytoplasmic region of both human and murine BTLA, similar to that of PD-1 contains an ITIM. Indeed, T cell activation is enhanced in BTLA-deficient mice [31, 32]. BTLA-mediated inhibition of human T cell activation occurred during both primary CD4+ T cell responses and secondary CD4+ and CD8+ T cell responses, suggesting that BTLA ligation sends a constitutive “off” signal to T cells and thus might play an important role in the maintenance of T cell tolerance [33].
T cell anergy
T cell activation requires recognition of specific antigenic peptides by the TCR, as signal 1, and additional costimulatory signals provided by accessory surface molecules on T cells, as signal 2. When costimulatory signals are absent, T-helper cells become anergic. Anergy is the state in which T-helper lymphocytes are alive but are incapable of proliferating and transcribing the interleukin (IL)-2 gene in response to optimal antigenic stimulation provided by professional antigen-presenting cells (APCs) [34]. Recent advances in the understanding of these pathways show the complexity of such networks and are challenging some of our preconceptions on T cell activation requirements [35]. Although detailed description of these signaling networks is beyond the scope of the present review, a basic outline of the major pathways, which are potential targets of novel immunomodulating therapeutic approaches, will be discussed.
Ligation of the TCR by antigenic peptides presented in the context of MHC proteins induces tyrosine phosphorylation of γ, δ, ε, and ζ polypeptides of the TCR-associated CD3 complex. This event is mediated by Src family tyrosine kinase such as Fyn and Lck, and leads to the recruitment of zeta-associated protein of 70 kDa (ZAP-70) to the TCR complex. ZAP-70 is then activated by phosphorylation of a tyrosine residue within the activation loop of the kinase domain by Lck and ZAP-70 itself. Activated ZAP-70 induces tyrosine phosphorylation of various downstream effector molecules, such as the adapter molecule linker for activation of T cells (LAT) and SH2 domain-containing leukocyte phosphoprotein of 76 kDa (SLP-76). These scaffold proteins can associate with distinct molecules, and this association regulates activation cascades further downstream. Signaling enzymes such as phosphatidylinositol 3-OH kinase (PI3K), phospholipase C, and a variety of nonenzymatic adapter proteins link these receptor-associated events to downstream pathways. Consequences of these proximal events include activation of mitogen-activated protein kinases (MAP kinases) through the Ras pathway, activation of IL-2 transcription through calcineurin phosphatase and nuclear factor of activated T cell (NFAT), and activation of protein kinase C [36].
In anergic cells many of these critical signaling events initiated by T cell activation do not occur, whereas other signaling events predominate [35]. Specifically, anergic cells are incapable of activating Lck and ZAP-70, phosphorylating the ε and ζ chain of the TCR and activating Ras, ERK, and JNK MAP kinases [37–42]. However, these cells have increased Fyn kinase activity, increased levels of free intracellular Ca++, phosphorylation of pLC-γ1, and increased levels of phosphatidylinositol 1, 4, 5 triphosphate [39]. Although Ras is not activated, anergizing stimulation results in the activation of Rap1, another small GTP-binding protein of the Ras family, which functions as an inhibitor of IL-2 gene transcription [43]. The mechanism by which Rap1-GTP inhibits IL-2 production is a subject at extensive ongoing studies. Our most recent study using transgenic mice that express the GTP-bound mutant Rap1E63 in T cells suggest that negative regulation of T-helper cell function by Rap-GTP is not due to the inhibition of Ras signaling pathway as previously reported in other systems [44]. These altered TCR proximal events and the selective predominance of unique or distinct downstream signaling pathways result in a selective profile of gene transcription in anergic cells. Using techniques for comparison of gene expression, it was determined that a distinct gene transcription program is activated in anergic cells compared to T cells stimulated via their TCR in the presence of costimulation [45–47]. Anergic cells also display a distinct protein expression profile, for instance, anergic cells exhibit increased expression of p27kip1, which is an essential regulator responsible for the blockade of clonal expansion of anergic T cells in vitro and in vivo [48, 49].
Extensive studies from many laboratories showed that CD28 provides the dominant costimulatory signal that cooperates with the TCR/CD3 complex to induce T cell activation, cytokine production, and clonal expansion and prevent the induction of anergy [34, 35]. Appleman et al. [50] observed that ligation of TCR/CD3, but not CD28 alone, resulted in the activation of MEK targets extracellular signal-related kinase 1/2, whereas ligation of CD28 alone was sufficient for the activation of PI3K target protein kinase B (PKB; c-Akt). Simultaneous activation of PI3K- and MEK1/2-dependent pathways was required to decrease the abundance of cyclin-dependent kinase inhibitor p27kip1 and induce cell cycle progression. These results show that the PI3K–PKB pathway links CD28 to cell cycle progression and suggest that p27kip1 integrates mitogenic MEK- and PI3K-dependent signals from TCR and CD28 in primary T lymphocytes [50].
It was suggested that calcium signaling is clearly critical for the first step of anergy induction [39, 51]. Calcium-induced anergy is mediated primarily by NFAT, a transcription factor regulated by the protein phosphatase calcineurin. During a productive activation, NFAT proteins are dephosphorylated and translocate to the nucleus where they cooperate with numbers of the AP-1 family of transcription factors to induce the expression of T-cell-associated genes [52]. Induction of calcium-induced unresponsiveness correlates with expression of a new set of NFAT-dependent genes that are independent of NFAT-AP-1 cooperation and do not overlay with genes activated during productive stimulation. These anergy-associated genes encode several classes of proteins that could function as negative regulators of TCR signaling and TCR-induced transcription, thus defining a genetic program associated with reduced responsiveness [53, 54].
Among the calcium-induced anergy-associated genes are genes encoding at least three E3 ubiquitin ligases, Itch, Cbl-b, and GRAIL [53]. Increased expression of these molecules may accompany chronic TCR signaling in vitro [55]. These proteins may interfere with TCR, CD28, and cytokine receptor signaling by tagging the TCR, CD28, and cytokine receptor signaling molecules with ubiquitin. Ubiquitination may trigger endocytosis, alter intracellular trafficking, promote proteolytic degradation of receptors or signaling subunits, or allosterically interfere with signaling [56–58]. It is not known whether these ubiquitin ligases are induced to higher levels in strongly self-reactive T cells in vivo. However, their importance for preventing autoimmunity in rodents is clear. Deletion or mutation of Itch and Cbl-b in mice are associated with disseminated autoimmune disease [59, 60]. Taken together, these extensive studies provide compelling evidence that the balance between stimulatory and inhibitory signals that are initiated via surface receptors and transmitted via specific signaling pathways is crucial to maximize protective immune responses while maintaining immunological tolerance and preventing autoimmunity [1].
Mechanisms of extrinsic regulation of T cell tolerance
Regulatory T cells
A significant development in the field of tolerance was the reemergence of the concept that T cell reactivity might be controlled by a distinct subset of T cells with a “regulatory function,” named Treg. The majority of these in vivo existing Treg constitutively express CD25 (IL-2 receptor alpha chain) and constitute 5–10% of CD4+ T cells in rodents and 1–2% of CD4+ T cells in humans. Many extensive excellent reviews on the development and function of CD4+CD25+ Treg are available [61, 62]. The present review does not directly address these issues. Instead, we will focus briefly on the relationship between the Treg function and the expression of the forkhead transcription factor Foxp3.
The X-chromosome-encoded transcription factor Foxp3 belongs to large family of functionally diverse transcription factors based on its winged helix forkhead DNA-binding domain. Homology among full-length human, mouse, rat Foxp3 is very high, suggesting a highly conserved function. At present, there is very little understanding of the function of Foxp3 at the molecular level. Foxp3 binds DNA, localizes to the nucleus and can act as a transcriptional repressor. Identification of consensus forkhead-binding domains adjacent to NFAT transcription factor binding sites in the promoters of several cytokine genes, including those encoding IL-2, IL-4, and tumor necrosis factor, led to the proposal of a model of Foxp3-mediated transcriptional inhibition or repression in which Foxp3 antagonizes NFAT function by competition for DNA-binding sites [63]. Based on those and other studies, it was also proposed that Foxp3 is induced in a variety of cell types as a general mechanism of negative immune regulation by repressing production of inflammatory cytokines. However, so far there has been no characterization of Foxp3 target genes or the transcriptional program regulated by Foxp3.
Foxp3 was recently identified as a key player in CD4+CD25+ Treg biology [64–66]. Recently, an unexpected observation related to the pathobiology of the Scurfy mice and the immune dysregulation, polyadenopathy, enteropathy, and X-linked inheritance (IPEX) syndrome in humans has shed some light to the characterization of naturally occurring Treg [67, 68]. The Scurfy mouse strain was generated about 50 years ago in a program to study the effects of ionizing radiation in mammals. The Scurfy mice developed an X-linked lymphoproliferative disease and died by 3 weeks of age [69]. Initial studies in these mice indicated that their CD4+ T cells were hyperresponsive to stimulation by a variety of cytokines. In addition, the adoptive transfer of these cells into SCID or nu/nu mice induced a rapid wasting disease. Overall, the phenotype of these mice resembles that of mice deficient for CTLA-4 or for transforming growth factor-beta (TGF-β) [70, 71]. It was recently determined that the disease is caused by loss of function of Scurfin, the product of a novel member of the Forkhead family of transcription factors that was termed Foxp3 [72]. Foxp3 functions as transcriptional repressor of various genes, including IL-2 [63].
Foxp3 is expressed in CD4+CD25+ Treg in the thymus and the periphery [73]. Forced expression of Foxp3 gene can convert murine naïve T cells to Treg both phenotypically and functionally. T cells overexpressing Foxp3 respond poorly to stimulation compared to Foxp3− cells and display reduced proliferation and cytokine production [64]. It is important to note that the amount of Foxp3 mRNA in transgenic mice directly correlates with the number of peripheral T cells [74]. This could represent the limited homeostatic expansion capacity of Foxp3+ transgenic Treg or a direct effect of Foxp3+ transgenic Treg on the overall T cell expansion. It is interesting to note that expression of Foxp3 during thymic development alone is not sufficient to protect Foxp3−/− animals [64, 65]. This observation indicates that Foxp3 expression within the peripheral tissues is necessary either for the maintenance and/or function of thymic-generated Treg, for the generation of Treg in the periphery, or for another function of Scurfin that has not yet been determined (Fig. 3).

Generation of Treg. CD4+CD25+ Treg are produced in the normal thymus. Some of the naïve CD4+CD25− T cells may also differentiate into Treg that express Foxp3 in the periphery. Treg suppress the activation and expansion of self-reactive T cells that may cause autoimmune diseases. In patients with IPEX syndrome, mutations in Foxp3 result in severe X-linked autoimmunity. In scurfy mice, loss of function of Scurfin, the product of Foxp3, results in X-linked lymphoproliferative disease and death by 3 weeks of age
Foxp3 is highly conserved in humans and appears to have a similar function in regulating immune quiescence. Mutations within Foxp3 result in a severe X-liked autoimmune syndrome known as IPEX [68, 75]. This is a rare disease in male children, characterized by autoimmune diabetes (type 1), severe allergy, and inflammatory bowel disease, similar to those induced in mice by depletion of CD4+CD25+ T cells. As mentioned above, it was reported that in rodents, Foxp3 is expressed only in CD4+CD25+ T cells occurring in vivo and is not induced by in vitro activation of CD4+CD25− naïve T cells [64]. In contrast, in human T cells Foxp3 is constitutively expressed in CD4+CD25+ T cells occurring in vivo, but can also be induced in a subset of CD4+CD25− T cells after stimulation in vitro [76]. These in vitro-induced Foxp3+ cells have regulatory functions and suppress immune responses of immune-competent T cells. This observation suggests two possibilities: One possibility is that naïve CD4+CD25− T cells can differentiate to CD4+CD25+ Treg upon TCR stimulation. A second possibility is that some of the Treg produced by the thymus are CD4+CD25− or loose their CD25 expression during circulation in the periphery. These cells can reacquire CD25 expression upon ligation of their TCR by antigen in a microenvironment of high IL-2 concentration, which also triggers their expansion. These observations indicate that there could be distinct mechanisms that control the generation and function of Treg in rodents and humans.
Reconciling the relationship between the antigen specificity of the Treg and that of the T cell being regulated will be essential for effective therapeutic exploitation of this phenomenon.
Antigen-presenting cells
Dendritic cells (DCs), the most potent professional APCs, were shown to contribute to immune tolerance. This function that is apparently incompatible with the conventional view that DCs are primarily involved in innate and adaptive immunity to infections and other antigens in vivo [77, 78]. The question not fully answered is whether DCs at distinct maturation stages perform a tolerogenic, or a distinct lineage of DCs has this important role. Evidence accumulating from both animal and human experiments indicates that immature DCs (iDCs) can suppress peripheral T cell responses or induce antigen-specific tolerance. In contrast, specific factors can induce DC maturation and promote a proinflammatory phenotype. For example, pathogen-associated molecular patterns containing components of bacteria, viruses, and parasites, such as lipopolysaccharides, peptidoglycans, CpG motifs, flagella, and viral nucleic acids induce Toll-like receptor signaling, which results in full activation of DCs, indicated by the expression of costimulatory ligands, adhesion molecules, chemokine receptors, and T-cell-activating cytokines. Such DCs mediate full stimulatory function during antigen presentation [78].
Local cytokine environment, e.g., presence of IL-10 and TFG-β, is another important contributor to the establishment of DC phenotype [79]. A recently emerged concept is that the dialog between Treg and DCs are crucial for regulation of alloimmune responses (Fig. 4). Using a human in vitro model system, it was shown that iDCs exposed to Treg can increase the expression of inhibitory molecules needed for the tolerogenic activity of DCs, and that tolerogenic DCs, in turn, can induce anergy in alloreactive CD4+ anergy T cells, thus establishing an inhibitory feedback loop [80]. Alternatively, the tolerance-inducing antigen presentation might even be the function of a dedicated DC subset, as indicated for the CD11c+CD4−OX41− DC subset in the rat [81]. Efforts to unravel the defining characteristics of a tolerogenic vs a stimulatory DC have led to pioneering studies in humans using antigen-pulsed iDCs to successfully induce T cell tolerance [77].

The properties of APC determine whether the presentation of antigen to T cells will result to the initiation of immune response or T cell suppression. DCs and monocytes are the most competent APCs and can be programmed to undergo a classical or alternative activation pattern. Alternatively, activated APC have immunosuppressive properties
Therapeutic relevance of T cell tolerance in hematopoietic cell transplantation
Bone marrow transplantation (BMT) is extensively used to correct hereditary defects (such as primary immunodeficiencies, metabolic diseases, or hemoglobinopathies), hematologic malignancies (such as acute or chronic myeloid leukemia), aplastic anemia, and medullary aplasia. Because a totally histocompatible graft is rarely available, two types of alloreactivity have to be dealt with. The most life-threatening type is the graft-versus-host disease (GvHD) caused mainly by T lymphocytes contained within the bone marrow graft. In contrast, in other cases the graft may suffer from rejection by the host’s immune system, leading to failure of the therapy. Induction of immunological tolerance to alloantigens would be the treatment of choice to prevent GvHD and allograft rejection in transplantation medicine. Based on elucidation of the mechanisms for self-tolerance, new and promising therapeutic interventions were developed in transplantation.
Induction of T cell tolerance by blockade of costimulation
Experimental studies showed that both CD28/B7 and CD40L/CD40 costimulatory pathways are critical for allograft rejection and their blockade during transplantation induced decreased proliferation of alloreactive T cells and increased apoptotic cell death and resulted in acceptance of allogeneic grafts [82]. Based on these results a pilot clinical trial was conducted that enable successful haploidentical BMT after ex vivo blockade of the B7-CD28/CTLA-4 pathway. Recipient peripheral blood mononuclear cells were collected, irradiated, and cocultured with donor bone marrow ex vivo in the presence of CTLA-4/Ig to block B7-mediated ligation, washed and infused to the patient. Ten out of 11 treated patients engrafted and developed full donor chimerism, and no clinically detectable GvHD [83]. These results support that ex vivo blockade of B7-mediated signals results in acceptance of human histoincompatible allograft in vivo without GvHD.
The role of the newly discovered pathway PD-1/PD-LI in the regulation of T cell response in transplantation tolerance is currently becoming apparent. In an animal islet transplantation model, recipient mice were treated with anti-CD40L mAb, along with PD-L1Ig, which stimulates the coinhibitory receptor PD-1. This combined approach induced long-term survival of pancreatic islet allografts, whereas treatment with each reagent alone failed to prevent islet allograft rejection [84]. In a model of GvHD, lethality was markedly accelerated by blockade of PD-1 pathway. It is interesting to note that coblockade of CTLA-4 and PD-1 was additive in augmenting GvHD, indicating that these pathways are not fully redundant [85].
Therapeutic applications of regulatory T cells
Accumulated evidence indicates that Treg play a critical role in transplantation tolerance. However, a major limitation for the use of Treg is the difficulty to obtain sufficient amounts of these relatively rare cells from a single donor. Most studies showed that prevention of GvHD requires the use of equivalent proportions of total donor cells and Treg. Treg can be expanded by ex vivo culture with allogeneic splenocytes and IL-2, and the administration of such Treg at the time of grafting delays or prevents GvHD [86]. The addition of TGF-β to the ex vivo Treg cultures strongly enhances the protective effect [87]. This effect may be probably due to its later established role in enhancing the functionality of Treg [88].
What are the effector mechanisms involved in the protection from GvHD by Treg? The observation that Treg expressing high levels of CD62L efficiently inhibit GvHD lethality indicates that initially they primarily act in secondary lymphoid tissues [87, 89]. Treg also appear to act in GvHD target tissues such as skin, liver, lung, and the gastrointestinal tract. In this regard, expression of the chemokine receptor CCR5 by Treg was shown to play a critical role in homing Treg to target tissues and to significantly improve survival after donor lymphocyte infusion [90]. In GvHD models, a role for Treg-generated IL-10 was reported [91]. IL-10 plays a critical but not exclusive role in Treg-mediated protection from GvHD. TGF-β and CTLA-4 may mediate the partial protection from GvHD observed with IL-10-deficient Treg [92].
GvHD and graft-versus-leukemia (GvL) are both due to alloreactivity, and if these two targets could not be discriminated by Treg, inhibition of GvHD by Treg would have similar effects as T cell depleted from bone marrow grafts. Edinger et al. [93] and Trenado et al. [94] showed that Treg significantly delayed GvHD in irradiated BALB/c mice injected with C57BL/6 bone marrow and T cells. When the mice were simultaneously injected with (host-type) A20 leukemia cells, the leukemic cells were cleared by the injected C57BL/6 T cells while suppression of GvHD remained unaffected. Therefore, Treg cells specific for recipient-type alloantigens could maintain a GvL activity. How Treg discriminate GvHD from GvL remains an open question. One potential mechanism may be due to the fact that Treg are more potent inhibitors of CD4+ than of CD8+ effector T lymphocytes [92]. However, in contrast to the reported discrimination of GvHD from GvL, Treg do not appear to be able to distinguish GvHD from graft-versus-tumor reaction [86]. Another advantage of using Treg along with bone marrow grafts is that Treg improve immune reconstitution [94]. This might be happening because Treg silence host T and natural killer cells, thereby allowing for efficient stem cell engraftment.
BMT is not only complicated by GvHD but also by rejection of the allograft. Preconditioning regimens and immunosuppressive drugs limit this complication and generally, graft rejection is not a clinical issue. However, these treatments have severe toxicity and are associated with severe side effects. A recent study has evaluated the capacity of ex vivo cultured Treg to inhibit bone marrow allograft rejection in sublethally irradiated hosts and concluded that Treg stimulated with donor-type APCs ex vivo can efficiently induce tolerance to bone marrow allografts. The induced tolerant state is durable and alloantigen-specific [92].
The role of antigen-presenting cells
As we discussed above, DCs are uniquely well-equipped APCs, which induce and regulate T cell reactivity. They play a critical role in central tolerance and maintenance peripheral tolerance in the normal steady state. After stem cell or organ transplantation, DCs present antigen to T cells via the direct or indirect pathways of allorecognition. These functions of DCs set in train the rejection response, but they also serve as potential targets for suppression of alloimmune reactivity and promotion of tolerance induction. Presently, the enhancement of the tolerogenicity of DCs was achieved by the use of iDCs or the pharmacological inhibition of DC maturation, or by the use of genetically engineered DCs expressing immunosuppressive molecules [95].
A novel strategy involving the use of DCs for the regulation of T cell responses consists of the generation of cytokine-modified regulatory DCs. In particular, DCs differentiated in the presence of exogenously added TGF-β, IL-10, granulocyte/macrophage colony-stimulating factor (GM-CSF), and IL-4 possess the immunophenotyic and functional features of iDCs and induce CD4+CD25+ Treg cells that suppress the response of Ag-primed CD4+ T cells to allogeneic normal mature DCs. Notably, the incidence of xenogenic GvHD was significantly reduced in SCID mice receiving transplants of human T cells primed with murine cytokine-modified DCs, indicating that these regulatory DCs induced anergy in human xenoreactive T cells, e.g., human T cells that recognized murine H-2d MHC molecules. A single injection of murine regulatory DCs after xenogenic transplantation prolonged the life span of hu-PBL-SCID mice, and this therapeutic effect could be abrogated by sequential injections of IL-2 [96].
The role of immunosuppressive drugs in the induction of regulatory DCs was extensively reviewed elsewhere [95]. Corticosteroids do not affect DC viability but downregulate the expression of costimulatory molecules on iDCs, prevent DC maturation, and impair their immunostimulatory activities by inhibiting the nuclear factor-kappa B pathway. The two calcineurin inhibitors cyclosporine A and tacrolimus have no effect on the expression of phenotypic markers during DC generation, but reduce the expression of costimulatory molecules on Langerhans cell and inhibit their differentiation in the epidermis. The capacity of DCs and Langerhans cells to stimulate allogeneic T cells is reduced in the presence of either drug [97].
The currently developing observations about the significance of the distinct differentiation programs of APC in the regulation of the immune response may have important implications in the field of transplantation. Clinical data showed that allografts of G-CSF-mobilized peripheral blood stem cells (PBSC) have an unexpected immunological behavior [98]. Transplantation of allogeneic G-CSF mobilized PBSC, which contain tenfold higher numbers of T cells compared with bone marrow grafts, did not result in higher incidence of GvHD. Moreover, such grafts achieved better engraftment across the HLA barrier. Potentially, CD14+ cells contained in the G-CSF-mobilized peripheral blood mononuclear cells have an active role in the reduced responsiveness of the CD4+ cells contained in this population. These CD14+ cells are involved in the impaired transactivation of the CD28 response element of G-CSF-mobilized CD4+ cells. It was shown that such CD14+ cells produce high levels of IL-10 and mediate their effect in an IL-10-dependent manner [99, 100].
G-CSF was initially used as a lineage-specific growth factor for neutrophils. It was also shown that G-CSF-mobilized PBSC from healthy donors contain high numbers of type 2 DCs (DC2), which prime T cells to produce IL-4 and IL-10 [101]. It is interesting to note that umbilical cord blood, another source of allogeneic stem cells for transplantation associated with low incidence of acute GvHD, contains DC2 and not DC1 type cells [102, 103]. These studies suggest that donor APC regulate both GvHD induction and engraftment and have a critical role in the clinical outcome of allogeneic transplantation. Taken together these observations suggest that APCs are potential regulators of the development and severity of GvHD. Moreover, they provide evidence that intervention in the regulation of APC maturation, differentiation, and surveillance, the complexity of which is only being unraveled now, provides great promise for therapeutic potential.
Conclusions and future directions
Lymphocyte quiescence has begun to gain recognition as an actively maintained state. Transcription factors appear to inhibit lymphocyte activation, metabolism, cell size, and cytokine transcription. In addition to intrinsic, powerful extrinsic mechanisms also control quiescence of T lymphocytes. CD4+CD25+ Treg have an essential role in controlling autoimmunity and allergy both in rodents and in humans. Despite the large number of studies examining Treg biology, many questions still remain unanswered. What is their antigen specificity and affinity? Are there specific markers for their identification? How are these cells generated in the thymus and how are they maintained and expanded in the periphery? What are the mechanisms by which they prevent autoimmunity in vivo? What is the mechanism via which Foxp3 mediates its effects? Clearly, more molecular understanding is required for the characterization of participating cell populations, identification of mechanisms responsible for their function, and exploitation of their properties for clinical applications.
Understanding the biochemical and molecular events that characterize intrinsic mechanisms of immune quiescence and regulate induction and maintenance of T cell tolerance/anergy will allow the development of new assays to evaluate the immune status of patients in a variety of clinical settings, including cancer, autoimmune diseases, and bone marrow or solid organ transplantation. It will also identify targets for the antigen-specific modulation of a variety of detrimental immune responses. This will involve the development of small molecules that activate anergy-specific signaling events or the development of RNA interference approaches for genes that need to be targeted to modify the antigen-specific response. Generation and expansion of antigen-specific T cells and Treg for use in adoptive immunotherapy protocols will greatly facilitate transplantation across the MHC. Such treatment approaches will minimize or prevent graft rejection and GvHD, allowing transplantation between individuals with increasing HLA disparity, thereby expanding the donor pool, enabling reduction of the need for nonspecific immunosuppression, and eliminating the risk of opportunistic infections.
References
Walker LS, Abbas AK (2002) The enemy within: keeping self-reactive T cells at bay in the periphery. Nat Rev Immunol 2:11–19
Nemazee D, Hogquist KA (2003) Antigen receptor selection by editing or downregulation of V(D)J recombination. Curr Opin Immunol 15:182–189
Gotter J, Kyewski B (2004) Regulating self-tolerance by deregulating gene expression. Curr Opin Immunol 16:741–745
Goodnow CC, Sprent J, Fazekas de St Groth B, Vinuesa CG (2005) Cellular and genetic mechanisms of self tolerance and autoimmunity. Nature 435:590–597
Anderson MS, Venanzi ES, Klein L, Chen Z, Berzins SP, Turley SJ, von Boehmer H, Bronson R, Dierich A, Benoist C, Mathis D (2002) Projection of an immunological self shadow within the thymus by the aire protein. Science 298:1395–1401
Su MA, Anderson MS (2004) Aire: an update. Curr Opin Immunol 16:746–752
McCarty N, Paust S, Ikizawa K, Dan I, Li X, Cantor H (2005) Signaling by the kinase MINK is essential in the negative selection of autoreactive thymocytes. Nat Immunol 6:65–72
Bunin A, Khwaja FW, Kersh GJ (2005) Regulation of Bim by TCR signals in CD4/CD8 double-positive thymocytes. J Immunol 175:1532–1539
Sakaguchi N, Takahashi T, Hata H, Nomura T, Tagami T, Yamazaki S, Sakihama T, Matsutani T, Negishi I, Nakatsuru S, Sakaguchi S (2003) Altered thymic T-cell selection due to a mutation of the ZAP-70 gene causes autoimmune arthritis in mice. Nature 426:454–460
Zhou T, Cheng J, Yang P, Wang Z, Liu C, Su X, Bluethmann H, Mountz JD (1996) Inhibition of Nur77/Nurr1 leads to inefficient clonal deletion of self-reactive T cells. J Exp Med 183:1879–1892
Dequiedt F, Van Lint J, Lecomte E, Van Duppen V, Seufferlein T, Vandenheede JR, Wattiez R, Kettmann R (2005) Phosphorylation of histone deacetylase 7 by protein kinase D mediates T cell receptor-induced Nur77 expression and apoptosis. J Exp Med 201:793–804
Wong P, Barton GM, Forbush KA, Rudensky AY (2001) Dynamic tuning of T cell reactivity by self-peptide-major histocompatibility complex ligands. J Exp Med 193:1179–1187
Smith K, Seddon B, Purbhoo MA, Zamoyska R, Fisher AG, Merkenschlager M (2001) Sensory adaptation in naive peripheral CD4 T cells. J Exp Med 194:1253–1261
Waterhouse P, Penninger JM, Timms E, Wakeham A, Shahinian A, Lee, KP, Thompson CB, Griesser H, Mak TW (1995) Lymphoproliferative disorders with early lethality in mice deficient in Ctla-4. Science 270:985–988
Tivol EA, Borriello F, Schweitzer AN, Lynch WP, Bluestone JA, Sharpe AH (1995) Loss of CTLA-4 leads to massive lymphoproliferation and fatal multiorgan tissue destruction, revealing a critical negative regulatory role of CTLA-4. Immunity 3:541–547
Egen JG, Allison JP (2002) Cytotoxic T lymphocyte antigen-4 accumulation in the immunological synapse is regulated by TCR signal strength. Immunity 16:23–35
Darlington PJ, Baroja ML, Chau TA, Siu E, Ling V, Carreno BM, Madrenas J (2002) Surface cytotoxic T lymphocyte-associated antigen 4 partitions within lipid rafts and relocates to the immunological synapse under conditions of inhibition of T cell activation. J Exp Med 195:1337–1347
Chikuma S, Imboden JB, Bluestone JA (2003) Negative regulation of T cell receptor-lipid raft interaction by cytotoxic T lymphocyte-associated antigen 4. J Exp Med 197:129–135
Egen JG, Kuhns MS, Allison JP (2002) CTLA-4: new insights into its biological function and use in tumor immunotherapy. Nat Immunol 3:611–618
Tivol EA, Boyd SD, McKeon S, Borriello F, Nickerson P, Strom TB, Sharpe AH (1997) CTLA4Ig prevents lymphoproliferation and fatal multiorgan tissue destruction in CTLA-4-deficient mice. J Immunol 158:5091–5094
Sharpe AH, Freeman GJ (2002) The B7-CD28 superfamily. Nat Rev Immunol 2:116–126
Ueda H, Howson JM, Esposito L, Heward J, Snook H, Chamberlain G, Rainbow DB, Hunter KM, Smith AN, Di Genova G, Herr MH, Dahlman I, Payne F, Smyth D, Lowe C, Twells RC, Howlett S, Healy B, Nutland S, Rance HE, Everett V, Smink LJ, Lam AC, Cordell HJ, Walker NM, Bordin C, Hulme J, Motzo C, Cucca F, Hess JF, Metzker ML, Rogers J, Gregory S, Allahabadia A, Nithiyananthan R, Tuomilehto-Wolf E, Tuomilehto J, Bingley P, Gillespie KM, Undlien DE, Ronningen KS, Guja C, Ionescu-Tirgoviste C, Savage DA, Maxwell AP, Carson DJ, Patterson CC, Franklyn JA, Clayton DG, Peterson LB, Wicker LS, Todd JA, Gough SC (2003) Association of the T-cell regulatory gene CTLA4 with susceptibility to autoimmune disease. Nature 423:506–511
Levin L, Tomer Y (2003) The etiology of autoimmune diabetes and thyroiditis: evidence for common genetic susceptibility. Autoimmun Rev 2:377–386
Agata Y, Kawasaki A, Nishimura H, Ishida Y, Tsubata T, Yagita H, Honjo T (1996) Expression of the PD-1 antigen on the surface of stimulated mouse T and B lymphocytes. Int Immunol 8:765–772
Freeman GJ, Long AJ, Iwai Y, Bourque K, Chernova T, Nishimura H, Fitz LJ, Malenkovich N, Okazaki T, Byrne MC, Horton HF, Fouser L, Carter L, Ling V Bowman MR, Carreno BM, Collins M, Wood CR, Honjo T (2000) Engagement of the PD-1 immunoinhibitory receptor by a novel B7 family member leads to negative regulation of lymphocyte activation. J Exp Med 192:1027–1034
Latchman Y, Wood CR, Chernova T, Chaudhary D, Borde M, Chernova I, Iwai Y, Long AJ, Brown JA, Nunes R, Greenfield EA, Bourque K, Boussiotis VA, Carter LL, Carreno BM, Malenkovich N, Nishimura H, Okazaki T, Honjo T, Sharpe AH, Freeman GJ (2001) PD-L2 is a second ligand for PD-1 and inhibits T cell activation. Nat Immunol 2:261–268
Nishimura H, Nose M, Hiai H, Minato N, Honjo T (1999) Development of lupus-like autoimmune diseases by disruption of the PD-1 gene encoding an ITIM motif-carrying immunoreceptor. Immunity 11:141–151
Nishimura H, Okazaki T, Tanaka Y, Nakatani K, Hara M, Matsumori A, Sasayama S, Mizoguchi A, Hiai H, Minato N, Honjo T (2001) Autoimmune dilated cardiomyopathy in PD-1 receptor-deficient mice. Science 291:319–322
Prokunina L, Castillejo-Lopez C, Oberg F, Gunnarsson I, Berg L, Magnusson V, Brookes AJ, Tentler D, Kristjansdottir H, Grondal G, Bolstad AI, Svenungsson, Lundberg EI, Sturfelt G, Jonssen A, Truedsson L, Lima G, Alcocer-Varela J, Jonsson R, Gyllensten UB, Harley JB, Alarcon-Segovia D, Steinsson K, Alarcon-Riquelme ME (2002) A regulatory polymorphism in PDCD1 is associated with susceptibility to systemic lupus erythematosus in humans. Nat Genet 32:666–669
Nielsen C, Laustrup H, Voss A, Junker P, Husby S, Lillevang ST (2004) A putative regulatory polymorphism in PD-1 is associated with nephropathy in a population-based cohort of systemic lupus erythematosus patients. Lupus 13:510–516
Watanabe N, Gavrieli M, Sedy JR, Yang J, Fallarino F, Loftin SK, Hurchla MA, Zimmerman N, Sim J, Zang X, Murphy TL, Russell JH, Allison JP, Murphy KM (2003) BTLA is a lymphocyte inhibitory receptor with similarities to CTLA-4 and PD-1. Nat Immunol 4:670–679
Krieg C, Han P, Stone R, Goularte OD, Kaye J (2005) Functional analysis of B and T lymphocyte attenuator engagement on CD4+ and CD8+ T cells. J Immunol 175:6420–6427
Otsuki N, Kamimura Y, Hashiguchi M, Azuma M (2006) Expression and function of the B and T lymphocyte attenuator (BTLA/CD272) on human T cells. Biochem Biophys Res Commun 344:1121–1127
Schwartz RH (1997) T cell clonal anergy. Curr Opin Immunol 9:351–357
Appleman LJ, Boussiotis VA (2003) T cell anergy and costimulation. Immunol Rev 191:1–20
Saito T, Yamasaki S (2003) Negative feedback of T cell activation through inhibitory adapters and costimulatory receptors. Immunol Rev 192:143–160
Sloan-Lancaster J, Shaw AS, Rothbard JB, Allen PM (1994) Partial T cell signaling: Altered phospho-ζ and lack of Zap70 recruitment in APL-induced T cell anergy. Cell 79:913–922
Madrenas J, Wange RL, Wange JR, Isakov N, Samelson LE, Germain RN (1995) ζ phosphorylation without ZAP-70 activation induced by TCR antagonists or partial agonists. Science 267:515–518
Gajewski TF, Qian D, Fields P, Fitch FW (1994) Anergic T-lymphocyte clones have altered inositol phosphate, calcium and tyrosine kinase signaling pathways. Proc Natl Acad Sci USA 91:38–42
Boussiotis VA, Barber DL, Lee BJ, Freeman GJ, Gribben JG, Nadler LM (1996) Differential association of protein tyrosine kinases with T cell receptor is linked to the induction of anergy and its prevention by B7 family-mediated costimulation. J Exp Med 184:365–376
Fields PE, Gajewski TF, Fitch FW (1996) Blocked Ras activation in anergic CD4+ T cells. Science 271:1276–1278
Li W, Whaley CD, Mondino A, Mueller DL (1996) Blocked signal transduction to the ERK and JNK protein kinases in anergic CD4+ T cells. Science 271:1272–1276
Boussiotis VA, Freeman GJ, Berezovskaya A, Barber DL, Nadler LM (1997) Maintenance of human T cell anergy: blocking of IL-2 gene transcription by activated Rap1. Science 278:124–128
Li L, Greenwald RJ, Lafuente EM, Tzachanis D, Berezovskaya A, Freeman, GJ, Sharpe AH, Boussiotis VA (2005) Rap1-GTP is a negative regulator of Th cell function and promotes the generation of CD4+CD103+ regulatory T cells in vivo. J Immunol 175:3133–3139
Tzachanis D, Freeman GJ, Hirano N, van Puijenbroek AA, Delfs MW, Berezovskaya A, Nadler LM, Boussiotis VA (2001) Tob is a negative regulator of activation that is expressed in anergic and quiescent T cells. Nat Immunol 2:1174–1182
Tzachanis D, Appleman LJ, Van Puijenbroek AA, Berezovskaya A, Nadler LM, Boussiotis VA (2003) Differential localization and function of ADP-ribosylation factor-6 in anergic human T cells: a potential marker for their identification. J Immunol 171:1691–1696
Safford M, Collins S, Lutz MA, Allen A, Huang CT, Kowalski J, Blackford A, Horton MR, Drake C, Schwartz RH, Powell JD (2005) Egr-2 and Egr-3 are negative regulators of T cell activation. Nat Immunol 6:472–480
Boussiotis VA, Freeman GF, Taylor PA, Berezovskaya A, Grass I, Blazar BR, Nadler LM et al (2000) p27kip1 functions as an anergy factor inhibiting IL-2 transcription and clonal expansion of alloreactive human and murine helper T lymphocytes. Nat Med 6:290–297
Greenwald RJ, Boussiotis VA, Lorsbach RB, Abbas AK, Sharpe AH (2001) CTLA4 regulates peripheral T cell tolerance in vivo. Immunity 14:145–155
Appleman LJ, van Puijenbroek AA, Shu KM, Nadler LM, Boussiotis VA (2002) CD28 costimulation mediates down-regulation of p27(kip1) and cell cycle progression by activation of the PI3K/PKB signaling pathway in primary human T cells. J Immunol 168:2729–2736
Sloan-Lancaster J, Steinberg TH, Allen PM (1996) Selective activation of the calcium signaling pathway by altered peptide ligands. J Exp Med 184:1525–1530
Clipstone NA, Crabtree GR (1992) Identification of calcineurin as a key signalling enzyme in T-lymphocyte activation. Nature 357:695–697
Feske S, Giltnane J, Dolmetsch R, Staudt LM, Rao A (2001) Gene regulation mediated by calcium signals in T lymphocytes. Nat Immunol 2:316–324
Macian F, Garcia-Cozar F, Im SH, Horton HF, Byrne MC, Rao A (2002) Transcriptional mechanisms underlying lymphocyte tolerance. Cell 109:719–731
Anandasabapathy N, Ford GS, Bloom D, Holness C, Paragas V, Seroogy C, Skrenta H, Hollenhorst M, Fathman CG, Soares L (2003) GRAIL: an E3 ubiquitin ligase that inhibits cytokine gene transcription is expressed in anergic CD4+ T cells. Immunity 18:535–547
Heissmeyer V, Macian F, Im SH, Varma R, Feske S, Venuprasad K, Gu H, Liu YC, Dustin ML, Rao A (2004) Calcineurin imposes T cell unresponsiveness through targeted proteolysis of signaling proteins. Nat Immunol 5:255–265
Liu YC (2004) Ubiquitin ligases and the immune response. Annu Rev Immunol 22:81–127
Naramura M, Jang IK, Kole H, Huang F, Haines D, Gu H (2002) c-Cbl and Cbl-b regulate T cell responsiveness by promoting ligand-induced TCR down-modulation. Nat Immunol 3:1192–1199
Jeon MS, Atfield A, Venuprasad K, Krawczyk C, Sarao R, Elly C, Yang C, Arya S, Bachmaier K, Su L, Bouchard D, Jones R, Gronski M, Ohashi P, Wada T, Bloom D, Fathman CG, Liu YC, Penninger JM (2004) Essential role of the E3 ubiquitin ligase Cbl-b in T cell anergy induction. Immunity 21:167–177
Fang D, Elly C, Gao B, Fang N, Altman Y, Joazeiro C, Hunter T, Copeland N, Jenkins N, Liu YC (2002) Dysregulation of T lymphocyte function in itchy mice: a role for Itch in TH2 differentiation. Nat Immunol 3:281–287
Sakaguchi S (2005) Naturally arising Foxp3-expressing CD25+CD4+ regulatory T cells in immunological tolerance to self and non-self. Nat Immunol 6:345–352
von Boehmer H (2005) Mechanisms of suppression by suppressor T cells. Nat Immunol 6:338–344
Schubert LA, Jeffery E, Zhang Y, Ramsdell F, Ziegler SF (2001) Scurfin (FOXP3) acts as a repressor of transcription and regulates T cell activation. J Biol Chem 276:37672–37679
Fontenot JD, Gavin MA, Rudensky AY (2003) Foxp3 programs the development and function of CD4+CD25+ regulatory T cells. Nat Immunol 4:330–336
Fontenot JD, Rudensky AY (2005) A well adapted regulatory contrivance: regulatory T cell development and the forkhead family transcription factor Foxp3. Nat Immunol 6:331–337
Fontenot JD, Rasmussen JP, Gavin MA, Rudensky AY (2005) A function for interleukin 2 in Foxp3-expressing regulatory T cells. Nat Immunol 6:1142–1151
Brunkow ME, Jeffery EW, Hjerrild KA, Paeper B, Clark LB, Yasayko SA, Wilkinson JE, Galas D, Ziegler SF, Ramsdell F (2001) Disruption of a new forkhead/winged-helix protein, scurfin, results in the fatal lymphoproliferative disorder of the scurfy mouse. Nat Genet 27:68–73
Bennett CL, Christie J, Ramsdell F, Brunkow ME, Ferguson PJ, Whitesell L, Kelly TE, Saulsbury FT, Chance PF, Ochs HD (2001) The immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX) is caused by mutations of FOXP3. Nat Genet 27:20–21
Blair PJ, Bultman SJ, Haas JC, Rouse BT, Wilkinson JE, Godfrey VL (1994) CD4+CD8− T cells are the effector cells in disease pathogenesis in the scurfy (sf) mouse. J Immunol 153:3764–3774
Shull MM, Ormsby I, Kier AB, Pawlowski S, Diebold RJ, Yin M, Allen R, Sidman C, Proetzel G, Calvin DA, Annunziata N, Doetschman T (1992) Targeted disruption of the mouse transforming growth factor-beta 1 gene results in multifocal inflammatory disease. Nature 359:693–699
Gorelik L, Flavell RA (2000) Abrogation of TGFb signaling in T cells leads to spontaneous T cell differentiation and autoimmune disease. Immunity 12:171–181
Hori S, Nomura T, Sakaguchi S (2003) Control of regulatory T cell development by the transcription factor Foxp3. Science 299:1057–1061
Sakaguchi S (2003) The origin of FOXP3-expressing CD4+ regulatory T cells: thymus or periphery. J Clin Invest 112:1310–1312
Khattri R, Kasprowicz D, Cox T, Mortrud M, Appleby MW, Brunkow ME, Ziegler SF, Ramsdell F (2001) The amount of scurfin protein determines peripheral T cell number and responsiveness. J Immunol 167:6312–6320
Wildin RS, Ramsdell F, Peake J, Faravelli F, Casanova JL, Buist N, Levy-Lahad E, Mazzella M, Goulet O, Perroni L, Bricarelli FD, Byrne G, McEuen M, Proll S, Appleby M, Brunkow ME (2001) X-linked neonatal diabetes mellitus, enteropathy and endocrinopathy syndrome is the human equivalent of mouse scurfy. Nat Genet 27:18–20
Walker MR, Kasprowicz DJ, Gersuk VH, Benard A, Van Landeghen M, Buckner JH, Ziegler SF (2003) Induction of FoxP3 and acquisition of T regulatory activity by stimulated human CD4+CD25− T cells. J Clin Invest 112:1437–1443
Steinman RM, Hawiger D, Nussenzweig MC (2003) Tolerogenic dendritic cells. Annu Rev Immunol 21:685–711
Wallet MA, Sen P, Tisch R (2005) Immunoregulation of dendritic cells. Clin Med Res 3:166–175
Allavena P, Piemonti L, Longoni D, Bernasconi S, Stoppacciaro A, Ruco L, Mantovani A (1998) IL-10 prevents the differentiation of monocytes to dendritic cells but promotes their maturation to macrophages. Eur J Immunol 28:359–369
Goerdt S, Orfanos CE (1999) Other functions, other genes: alternative activation of antigen-presenting cells. Immunity 10:137–142
Powell TJ, Jenkins CD, Hattori R, MacPherson GG (2003) Rat bone marrow-derived dendritic cells, but not ex vivo dendritic cells, secrete nitric oxide and can inhibit T-cell proliferation. Immunology 109:197–208
Blazar BR, Taylor PA, Panoskaltsis-Mortari A, Buhlman J, Xu J, Flavell RA, Korngofd R, Noelle R, Vallera DA (1997) Blockade of CD40 ligand-CD40 interaction impairs CD4+ T cell-mediated alloreactivity by inhibiting mature donor T cell expansion and function after bone marrow transplantation. J Immunol 158:29–39
Guinan EC, Boussiotis VA, Neuberg D, LaVita Brennan L, Hirano N, Nadler LM, Gribben JG (1999) Transplantation of anergic histoincompatible bone marrow allografts. N Engl J Med 340:1704–1714
Gao W, Demirci G, Strom TB, Li XC (2003) Stimulating PD-1-negative signals concurrent with blocking CD154 co-stimulation induces long-term islet allograft survival. Transplantation 76:994–999
Blazar BR, Carreno BM, Panoskaltsis-Mortari A, Carter L, Iwai Y, Yagita H, Nishimura H, Taylor PA (2003) Blockade of programmed death-1 engagement accelerates graft-versus-host disease lethality by an IFN-gamma-dependent mechanism. J Immunol 171:1272–1277
Cohen JL, Trenado A, Vasey D, Klatzmann D, Salomon BL (2002) CD4(+)CD25(+) immunoregulatory T cells: new therapeutics for graft-versus-host disease. J Exp Med 196:401–406
Taylor PA, Lees CJ, Blazar BR (2002) The infusion of ex vivo activated and expanded CD4(+)CD25(+) immune regulatory cells inhibits graft-versus-host disease lethality. Blood 99:3493–3499
Marie JC, Letterio JJ, Gavin M, Rudensky AY (2005) TGF-beta1 maintains suppressor function and Foxp3 expression in CD4+CD25+ regulatory T cells. J Exp Med 201:1061–1067
Ermann J, Hoffmann P, Edinger M, Dutt S, Blankenberg FG, Higgins JP, Negrin RS, Fathman CG, Strober S (2005) Only the CD62L+ subpopulation of CD4+CD25+ regulatory T cells protects from lethal acute GVHD. Blood 105:2220–2226
Wysocki CA, Jiang Q, Panoskaltsis-Mortari A, Taylor PA, McKinnon KP, Su L, Blazar BR, Serody JS (2005) Critical role for CCR5 in the function of donor CD4+CD25+ regulatory T cells during acute graft-versus-host disease. Blood 106:3300–3307
Hoffmann P, Ermann J, Edinger M, Fathman CG, Strober S (2002) Donor-type CD4(+)CD25(+) regulatory T cells suppress lethal acute graft-versus-host disease after allogeneic bone marrow transplantation. J Exp Med 196:389–399
Joffre O, van Meerwijk JP (2006) CD4(+)CD25(+) regulatory T lymphocytes in bone marrow transplantation. Semin Immunol 18:128–135
Edinger M, Hoffmann P, Ermann J, Drago K, Fathman CG, Strober S, Negrin RS (2003) CD4+CD25+ regulatory T cells preserve graft-versus-tumor activity while inhibiting graft-versus-host disease after bone marrow transplantation. Nat Med 9:1144–1150
Trenado A, Charlotte F, Fisson S, Yagello M, Klatzmann D, Salomon BL, Cohen JL (2003) Recipient-type specific CD4+CD25+ regulatory T cells favor immune reconstitution and control graft-versus-host disease while maintaining graft-versus-leukemia. J Clin Invest 112:1688–1696
Hackstein H, Thomson AW (2004) Dendritic cells: emerging pharmacological targets of immunosuppressive drugs. Nat Rev Immunol 4:24–34
Sato K, Yamashita N, Baba M, Matsuyama T (2003) Modified myeloid dendritic cells act as regulatory dendritic cells to induce anergic and regulatory T cells. Blood 101:3581–3589
Nachbaur D, Kircher B (2005) Dendritic cells in allogeneic hematopoietic stem cell transplantation. Leuk Lymphoma 46:1387–1396
Bensinger WI, Martin PJ, Storer B, Clift R, Forman SJ, Negrin R, Kashyap A, Flowers ME, Lilleby K, Chauncey TR, Storb R, Appelbaum FR (2001) Transplantation of bone marrow as compared with peripheral-blood cells from HLA-identical relatives in patients with hematologic cancers. N Engl J Med 344:175–181
Mielcarek M, Martin PJ, Torok-Storb B (1997) Suppression of alloantigen-induced T-cell proliferation by CD14+ cells derived from granulocyte colony-stimulating factor-mobilized peripheral blood mononuclear cells. Blood 89:1629–1634
Mielcarek M, Graf L, Johnson G, Torok-Storb B (1998) Production of interleukin-10 by granulocyte colony-stimulating factor-mobilized blood products: a mechanism for monocyte-mediated suppression of T-cell proliferation. Blood 92:215–222
Arpinati M, Green CL, Heimfeld S, Heuser JE, Anasetti C (2000) Granulocyte-colony stimulating factor mobilizes T helper 2-inducing dendritic cells. Blood 95:2484–2490
Blom B, Ligthart SJ, Schotte R, Spits H (2002) Developmental origin of pre-DC2. Hum Immunol 63:1072–1080
Hagendorens MM, Ebo DG, Schuerwegh AJ, Huybrechs A, Van Bever HP, Bridts CH, De Clerck LS, Stevens WJ (2003) Differences in circulating dendritic cell subtypes in cord blood and peripheral blood of healthy and allergic children. Clin Exp Allergy 33:633–639
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Li, L., Boussiotis, V.A. Physiologic regulation of central and peripheral T cell tolerance: lessons for therapeutic applications. J Mol Med 84, 887–899 (2006). https://doi.org/10.1007/s00109-006-0098-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00109-006-0098-5