
Abstract
Purpose
Study objectives are to determine whether quality of life is recovered completely after major injury and to identify determinants associated with a worse quality of life.
Methods
Prospective 12-month follow-up of injured patients admitted to the intensive care unit in a Spanish level 1 trauma centre. The main outcome (quality of life) was measured using the EQ-5D-5L. The relationships between sociodemographic factors, injury severity and location, and quality of life scores were evaluated. Mean comparison analysis (95% confidence interval) was performed with the student “t” test for quantitative variables and with chi-squared for proportion comparison (qualitative variables). A multivariate logistic regression (odds ratio and 95% confidence interval) was performed to identify determinants of each dimension, and a multivariate linear regression (regression coefficient and 95% confidence interval) to identify the determinants of EQus and EQvas.
Results
Over a 2-year period, 304 patients who met the inclusion criteria were identified, and 200 patients (65.8%) were finally included. Most of patients suffered blunt trauma (91.5%), 72.5% were men, mean age was 47.8, mean ISS was 15.2. The overall health index (EQvas) improved slightly, but its mean value at 12 months was below the Spanish population norm (P < 0.001). In the multivariate analysis, age ≥ 55, female gender and unskilled employment were risk factors for a lower EQvas. Also in the multivariate analysis, having a severe extremity injury was associated with a lower score on the mobility dimension (OR 6.56 95% CI 2.00, 21.55) while age ≥ 55 years was associated with a lower score on the usual activities dimension (OR 3.52 95% CI 1.17, 10.57). Female gender was the most important factor associated with suffering pain (OR 4.54, 95% CI 2.01, 10.27) and depression/anxiety (OR 4.04, 95% CI 1.88, 8.65). In the univariate and multivariate analyses, female gender, age ≥ 55 years, ISS ≥ 25 and severe extremity injury were associated with a lower EQ utility score (EQus).
Conclusions
The quality of life score improves during the first year after major trauma. However, it does not return to the reference levels for the normal population. Female gender and age ≥ 55 years are statistically significant determinants of poorer EQvas and EQus.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Today, in Spain, major trauma remains the first cause of death in the young population; it is the first in the 15–34 year age group, and the second, after tumour-related deaths, in the 35–44 year group. However, mortality represents only a minor proportion of the health impact of major trauma. According to data from the Spanish directorate general of traffic (DGT) [1], for every road traffic accident-related death there are six major injuries and 68 minor injuries, which may cause life-long disabilities and generate high economic, health care and social costs. Several cohort studies have found that the functional results in injured patients are notably worse than those in reference populations [2,3,4], that at least half of patients with major injuries have residual disabilities, and that a quarter do not return to work [5]. Thus, a complete evaluation of trauma care also requires the assessment of quality of life (QoL). Quality of life is measured with standardized scales that measure the impact of injuries on overall health status. Due to the huge variety in functional outcomes, there are multiple QoL scales and questionnaires and it is difficult to find a single, uniform disability measure.
Spain does not have a national trauma registry and functional long-term outcomes are not systematically evaluated or recorded. To our knowledge, this study is the largest follow-up registry of QoL after major trauma carried out so far in this country. Our main objective is to determine whether patients experience a complete recovery of QoL after a trauma injury. The secondary objectives are to identify determinants of worse QoL and to determine the worst rated dimension, to be able to design and implement measures that can improve outcomes. Our hypothesis is that there is a significant deterioration in the QoL after a major trauma and its recovery is slow and limited.
Methods
A prospective follow-up observational study was performed at a level 1 trauma centre [Hospital Universitari Parc Taulí, Sabadell (Barcelona)]. All trauma patients aged 16 and older admitted to intensive (or semi-intensive) care units (ICU) from April 2012 to March 2014 were included. Exclusion criteria were patient death before hospital discharge and patients unable to answer questionnaires (or without family members able to do so).
Data were recorded prospectively after hospital admission in a computerized database (Microsoft® Access 2003) with protected format. All patients included in the study (or their relatives) provided sociodemographic data through personal interviews at admission, and answered the EQ-5D-5L questionnaire at hospital discharge, 3, 6 and 12 months post-injury through a telephone interview. The EQ-5D-5L is a QoL measure scale [6] available and validated in Spanish and used previously in other traumatic cohorts. The scale evaluates five dimensions: mobility, self-care, usual activities, pain and depression/anxiety on a scale from 1-no problems at all to 5-incapacity. The EQ-5D-5L user guide [7] recommends summarizing dimension scores in two categories: (a) no problems or slight problems (equal to scores 1 or 2), and (b) moderate, severe or incapacitating problems (equal to scores 3, 4, and 5). From the scores of the five dimensions, an overall score is obtained: the EQ utility score, or EQus. The EQus expresses the overall score of all the dimensions and summarizes the functional incapacity of the patient. Every country has a standardized EQus for every combination of the five dimension scores [6]. In Spain, the EQus oscillates between 1.000 (best score) and − 0.654 (worst score). The second part of the EQ-5D-5L questionnaire consists of a visual analogue scale from 1 to 100 reflecting overall health, generating a score known as EQvas. EQvas reflects the patient’s degree of acceptance of his/her limitations, while EQus reflects the functional limitation that disability induces.
The study was approved by our centre’s Ethics Committee and the information was collected anonymously and confidentially. All patients (or relatives acting in their name) signed an informed consent form. All patients were contacted four times for each follow-up examination (discharge, 3, 6 and 12 months).
The main outcome (QoL) was measured by the EQvas and EQus scores. The relationships between sociodemographic factors, injury severity and location, and QoL scores were evaluated. Mean comparison analysis (95% confidence interval) was performed with the student “t” test for quantitative variables and with chi-squared for proportion comparison (qualitative variables). A multivariate logistic regression (odds ratio and 95% confidence interval) was performed to identify determinants of each dimension, and a multivariate linear regression (regression coefficient and 95% confidence interval) to identify the determinants of EQus and EQvas. Statistical analysis was performed with Stata12®.
Results
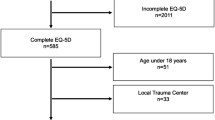
From April 2012 to March 2014, 348 patients with major injury aged over 16 and admitted to our ICU (or who died in the hospital before admission to ICU) were prospectively recorded. From those, 200 patients (see Fig. 1) were finally included and interviewed on admission to the ICU. There were no differences between the patients included in the study and those who met the inclusion criteria but were not included (see Table 1).

Patients included
Dimensions
Figure 2 shows the proportion of patients in each category (from 1-no problems at all to 5-total incapacity), for each dimension, and for each interview (at discharge, 3, 6 and 12 months). For ease of interpretation a colour code has been added: white = 1, green = 2, yellow = 3, red = 4, black = 5.

Evolution of dimensions during follow-up
Initially (at hospital discharge), the best rated dimension was anxiety/depression, followed by mobility and self-care. Mobility improved progressively during follow-up, and at 12 months after the trauma 80% of the patients had no or only slight mobility difficulties. At 12 months, self-care was the best rated dimension, with 85% of the patients having no or only slight difficulties on that dimension.
Initially, the worst rated dimension was resumption of usual activities (fewer than 40% of the trauma population had no or only slight difficulties), but this score improved steadily to 62% at 12 months. In contrast, pain (the second worst rated dimension at discharge), did not improve during follow-up; at 12 months 52% had no or only slight pain, the same proportion as at discharge. Over the first year, anxiety/depression scores rose (78.7% reported no or only slight anxiety at discharge, but only 70.2% at 12 months). In women, anxiety was the second worst rated dimension after pain.
Table 2 shows the comparison of the proportion of patients in category B (moderate, severe or incapacitating problems) with those in the Spanish population as a whole [6]. Our patients’ scores at 12 months were significantly higher for all dimensions, and none had returned to normal values.
Table 3 shows the multivariate logistic regression analysis [with odds ratios (OR) and 95% confidence intervals (CI)] for the different factors associated with problems in the different dimensions at 12 months after the injury. Severe extremity injury was associated with worse mobility, while age ≥ 55 years was associated with worse outcomes on the self-care dimension. Female gender was associated with problems on the pain and anxiety/depression dimensions.
Eq-5d-5l utility score (Equs)
In our study the EQus improved during follow-up (Fig. 3). The univariate analysis found female gender, age ≥ 55, Injury severity score (ISS) ≥ 25 and severe extremity injury to be determinants of a worse EQus at 12 months. In the multivariate analysis (see Table 4) female gender, age ≥ 55 and severe extremity injury were negatively associated with EQus throughout the follow-up.

EQus evolution
EQvas
The evolution of this parameter during follow-up is shown in Fig. 4. Median EQvas score at discharge was 60, improving slightly during follow-up to 65 at 3 months, 70 at 6 months, and 75 at 12 months. However, compared to the standardized data on the Spanish population [6], at 12 months, the scores of both men and women were lower than those of the reference population (see Table 5).

Evolution of EQvas
Female gender, age ≥ 55 years and unskilled employment were associated with a lower EQvas score (worse overall health) in both the univariate analysis and the multivariate analysis (Table 6) at 12 months.
Discussion
A total of 304 patients met the study’s inclusion criteria, but only 200 patients were finally included (66%). This low participation is common in studies of this type; other authors have reported figures ranging from 32 to 93% [2, 4, 9,10,11,12]. It is due to factors such as the data collection method, patients’ age and injury severity. In any case, in our study there were no differences between the characteristics of patients included and patients who met the inclusion criteria but did not take part.
As the EQ-5D-5L questionnaire could not be administered at ICU admission, we assumed that prior to the injury the cohort would have presented similar QoL values to those of the normal Spanish population [6]. Therefore, at 12 months, our cohort’s EQvas and scores on dimensions were compared with these normative values. Our results showed that, 1 year after the injury, EQvas had improved but had not returned to its pre-trauma values. These findings corroborate those of many previous studies [2,3,4, 13,14,15,16,17,18,19].
There are multiple determinants of quality of life: demographics, social and injury-related. According to our study, female gender is the main determinant of a worse QoL (lower EQvas, EQus and worse dimension scores). These results are supported by other studies in which female gender was the risk factor most closely associated with poor QoL [2, 4, 17, 20]. However, in the study by Holtslag et al. [12] in 2007, women scored slightly higher, although the difference was not statistically significant. The low scores of women for pain and anxiety dimensions corroborate those of previous studies [4, 5, 9, 21]. In the general population, women have a poorer quality of life than men [6], but these differences are accentuated after the injury. The finding that there are gender differences in pain and anxiety dimensions but not in mobility or usual activities is significant. Women in our society have the role of main family carers, and after an injury, their ability to carry out this role is limited. This incapacity accentuates the pain due to its high psychological component and increases the anxiety and depression. These results are unlikely to improve without profound changes in the organization of gender roles in our society. Given the evidence of low scores of women for anxiety and other psychological disorders [21], we would suggest a gender-specific intervention with psychological support for female injured patients.
In our study, age ≥ 55 years was associated with a lower EQvas at 12 months, a lower EQus and a poorer assessment of the usual activities dimension. Old age has been associated with poorer QoL in multiple studies [10, 14, 17, 20, 22]; according to Rainer et al. [2] age > 65 years was the strongest determinant of poor QoL (OR 4.77). Although previous authors have associated the absence of morbidity with better QoL [2, 4, 12], this was not reflected in our study. We did not find a strong association between low education level and poor QoL (low level of schooling was only associated with a worse EQus at 6 months).
Regarding severity of injury, and in accordance with previous studies [2, 4, 12], we found an ISS ≥ 25 to be a factor of worse prognosis. In our cohort only 12.5% patients had an ISS ≥ 25; this score was associated with a lower EQus but not with a lower EQvas or a lower score in any dimension. As in previous studies [10, 23], hospital length of stay was not associated with long-term QoL.
As for the site of the injury, several studies [4, 10, 12, 21, 24] have shown injuries to the extremities to be determinants of poor QoL. Severe spine and spinal cord injuries have also associated with a worse QoL [12]; however, in our study, we had only one patient with spinal cord injury and this association was not found. The relationship between severe intracranial injuries and quality of life is controversial, probably due to differences in the definition of the injury. We found no association between QoL and severe intracranial injury when the latter was defined in accordance with the AIS [8] as intracranial AIS ≥ 3, or as Glasgow score ≤ 8, or as both Glasgow ≤ 8 and AIS ≥ 3. Several authors [5, 9, 10] have stressed that the consequences of cranial injuries are not well captured by the EQ-5D-5L questionnaire. In fact, some have decided to add GOS [25] or GOSE [26] questionnaires to improve this deficit [12, 22], and have thus found an association between severe intracranial injury and a worse quality of life.
In our study the worst rated dimension after 12 months was pain. This finding corroborates those of Ulvik et al. [23], who found that most patients suffered pain more than 2 years after injury, and those of Gabbe et al. [27] who reported that pain was worse at 18 months after the injury than at 12 months (OR 1.8, 95% CI: 1.2, 2.8).
This study has the limitations of observational follow-up studies (loss of follow-up, response bias), but its results are similar to those of other European, US or Australian studies. EQ-5D-5L questionnaire is validated for telephonic use. However, telephonic use entails loss of follow-up due to change of telephonic numbers or absence of answer. The only type of follow-up that could improve results would be a personal interview at home (or rehabilitation centre) but it would increase costs too. A specific limitation of our study is its single-centre design; however, since the sociodemographic data of our trauma population are similar to the normative data for Catalonia, we think that our results may be generally applicable in our country. Another important limitation of our study is the impossibility to obtain a previous score of quality of life before the trauma injury. Since it is impossible to predict who and when will suffer a traumatism, it is practically impossible to get a reliable score of quality of life just before it.
Conclusion
The factors identified as determinants of a worse quality of life are not modifiable (female gender, age > 55 years, extremities injury). However, this study identified pain as the dimension that was rated lowest by our trauma population. In the future, we would like to carry out a long-term follow-up from pain clinics of all our major trauma patients, identifying the ones with risk factors that will need support and treatment.
Finally, we stress that accurate recording and follow-up of these patients is essential and that quality of life is at least as important as mortality in the evaluation of the quality of trauma care. Thus, the authors call once more for a Spanish national trauma database. Such database might be of a great value to improve our knowledge about trauma epidemiology and outcomes in Spain and to evaluate the quality of our trauma care.
References
Dirección General de Tráfico. Anuario estadístico de accidentes 2013, Dirección General de Tráfico, Madrid; 2015. pp. 5–7.
Rainer TH, Yeung JH, Cheung SK, et al. Assessment of quality of life and functional outcome in patients sustaining moderate and major trauma: a multicentre, prospective cohort study. Injury. 2014;45(5):902–9.
Fitzharris M, Fildes B, Charlton J, et al. General health status and functional disability following injury in traffic crashes. Traffic Inj Prev. 2007;8(3):309–20.
Ringburg AN, Polinder S, van Ierland MC, et al. Prevalence and prognostic factors of disability after major trauma. J Trauma. 2011;70(4):916–22.
Vles WJ, Steyerberg EW, Essink-Bot ML, et al. Prevalence and determinants of disabilities and return to work after major trauma. J Trauma. 2005;58(1):126 – 35.
Szende A, Williams A. Measuring self-reported population health: an international perspective based on EQ-5D, EuroQol Group; 2004.
Rabin R, Oemar M, Oppe M, et al. EQ-5D-5L User Guide. Basic information on how to use the EQ-5D-5L instrument, EuroQol Group; 2011.
Gennarelli T, Wodzin E. The Abbreviated Injury Scale 2005. Update 2008. Des Plaines, IL; 2008.
Meerding WJ, Looman CW, Essink-Bot ML, et al. Distribution and determinants of health and work status in a comprehensive population of injury patients. J Trauma. 2004;56(1):150–61.
Serviá Goixart L, Badia Castelló M, Montserrat Ortiz N, et al. Risk factors for the deterioration of quality of life in critical trauma patients. Assessment at 6 and 12 months after discharge from the intensive care unit. Med Intensiva. 2013;38(1):1–10.
Gabbe BJ, Cameron PA, Hannaford AP, et al. Routine follow up of major trauma patients from trauma registries: What are the outcomes? J Trauma. 2006;61(6):1393–9.
Holtslag HR, van Beeck EF, Lindeman E, et al. Determinants of long-term functional consequences after major trauma. J Trauma. 2007;62(4):919–27.
Aitken LM, Chaboyer W, Kendall E, et al. Health status after traumatic injury. J Trauma Acute Care Surg. 2012;72(6):1702–8.
Kenardy J, Heron-Delaney M, Warren J, et al. The effect of mental health on long-term health-related quality of life following a road traffic crash: results from the UQ SuPPORT study. Injury. 2015;46(5):883–90.
Overgaard M, Høyer CB, Christensen EF. Long-term survival and health-related quality of life 6 to 9 years after trauma. J Trauma. 2011;71(2):435–41.
Soberg HL, Bautz-Holter E, Roise O, et al. Long-term multidimensional functional consequences of severe multiple injuries two years after trauma: a prospective longitudinal cohort study. J Trauma. 2007;62(2):461–70.
Gabbe BJ, Simpson PM, Sutherland AM, et al. Improved functional outcomes for major trauma patients in a regionalized, inclusive trauma system. Ann Surg. 2012;255(6):1009–15.
Marasco S, Lee G, Summerhayes R, Fitzgerald M, et al. Quality of life after major trauma with multiple rib fractures. Injury. 2015;46(1):61–5.
Gabbe BJ, Simpson PM, Harrison JE, et al. Return to work and functional outcomes after major trauma: who recovers, when, and how Well? Ann Surg. 2016;263(4):623–32.
Innocenti F, Del Taglia B, Coppa A, et al. Quality of life after mild to moderate trauma. Injury. 2015;46(5):902–8.
Holbrook TL, Hoyt DB. The impact of major trauma: quality-of-life outcomes are worse in women than in men, independent of mechanism and injury severity. J Trauma. 2004;56(2):284–90.
Dimopoulou I, Anthi A, Mastora Z, et al. Health-related quality of life and disability in survivors of multiple trauma one year after intensive care unit discharge. Am J Phys Med Rehabil. 2004;83(3):171–6.
Ulvik A, Kvåle R, Wentzel-Larsen T, et al. Quality of life 2–7 years after major trauma. Acta Anaesthesiol Scand. 2008;52(2):195–201.
MacKenzie EJ, Shapiro S, Smith RT, et al. Factors influencing return to work following hospitalization for traumatic injury. Am J Public Health. 1987;77(3):329–34.
Isaac L. The glasgow outcome scale, the center for outcome measurement in brain injury. 2000. http://www.tbims.org/combi/gos.
Sander A. The extended glasgow outcome scale, the center for outcome measurement in brain injury. 2002. http://www.tbims.org/combi/gose.
Gabbe BJ, Simpson PM, Sutherland AM, et al. Evaluating time points for measuring recovery after major trauma in adults. Ann Surg. 2013;257(1):166–72.
Acknowledgements
Thank you to Mireia Figueroa, JavieraHernández and Georgina Vila for all the efforts. Without your constant dedication, this study had not been possible.
Funding
IX Convocatoria de Becas y Ayudas a la Investigación Médica de la Fundación Mutua Madrileña.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Research involving human participants and/or animals
The study was approved by our centre’s Ethics Committee and the information was collected anonymously and confidentially.
Informed consent
All patients (or relatives acting in their name) signed an informed consent form.
Rights and permissions
About this article

Cite this article
Llaquet Bayo, H., Montmany, S., Rebasa, P. et al. Analysis of quality of life after major trauma: a spanish follow-up cohort study. Eur J Trauma Emerg Surg 45, 289–297 (2019). https://doi.org/10.1007/s00068-018-0920-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-018-0920-0