
Abstract
Introduction
Most patients with penetrating chest injuries benefit from early treatment with chest tube drainage or surgery. Although penetrating chest injury is not uncommon, few descriptive studies are published, especially in Europe. The aim of this study was to review our experience and further improve our management of penetrating chest injuries in a level I trauma center in the Netherlands.
Methods
All patients with penetrating chest injury between August 2004 and December 2012 were included. Demographics, mechanism of injury, physiological parameters, Injury Severity Scores (ISS), surgical and non-surgical treatment, length of intensive care unit (ICU) stay, length of hospital stay (LOS), complications and rate of mortality were collected.
Results
A total of 159 patients were analyzed. Patients included 116 (73 %) stab wounds and 34 (21 %) gunshot wounds. In 27 patients (17 %), cardiac injury was seen. The mean ISS was 12. Almost half of all patients (49 %) were treated with only chest tube drainage. Alternatively, surgical treatment was performed in 24 % of all cases. Anterolateral incision was most frequently used to gain access to the thoracic cavity. The mean LOS was 9 days. Among all patients, 17 % were admitted to the ICU with a mean stay of 3 days. In 18 (11 %) patients, one or more complications occurred. The 30-day mortality was 7.5 %.
Conclusion
Patients presenting with penetrating chest injury are not uncommon in the Netherlands and can mostly be treated conservatively. In one-fourth of the patients, surgical treatment is performed. A structural and vigorous approach is needed for good clinical outcome.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In civilian practice, penetrating chest injuries are most likely due to stabbings and gunshots [1]. The incidence depends on regional circumstances like crime rates, therefore medical centers in urban areas deal in general more frequently with penetrating thoracic injury [2]. Early treatment of stab and gunshot wounds of the chest improves prognosis and outcome. Most patients are treated with chest tube drainage; however, in some patients surgical exploration is needed. In general, surgical treatment depends on clinical presentation and radiographic findings. Several indications for thoracotomy are formulated; these include a large initial and continued chest tube output, deterioration of hemodynamic condition, hemodynamic shock, signs of pericardial tamponade, massive air leakage and radiographic evidence of large hemothorax [3]. In chest stabbing and gunshot wounds, mortality is associated with the Injury Severity Scores (ISS), total blood loss, blood transfusion volume, systolic blood pressure (SBP) on arrival and associated injury of the diaphragm, abdomen and mediastinum [3, 4]. Although penetrating chest injuries are common, few descriptive studies have been published about this subject in the last decade, especially in Europe, despite surgical and imaging technological developments during this time. In this article, we reviewed our experience with penetrating chest injuries to evaluate the outcome of surgical and non-surgical treatment, and identify opportunities for improving our outcome in a level I trauma center in the Netherlands.
Materials and methods
All patients with penetrating chest injury during the period August 2004 till December 2012, who were presented at our hospital, were included.
All data were retrospectively collected using our Trauma Registry Database, Patient Information System and medical records. Data collected include demographics, mechanism of injury, physiological parameters during hospital admission, ISS, surgical and non-surgical treatment, length of intensive care unit (ICU) stay, length of hospital stay, complications and rate of mortality.
For statistical analyses, SPSS 20.0 was used. Continuous data are presented as mean and standard deviation. Discrete data are presented as median and range. The χ2 and Fisher exact-test was assessed for discrete data and for continuous data the t test was employed. Differences were considered to be statistically significant when the p value was <0.05.
According to Dutch regulation, retrospective medical data analysis does not require consent by the medical ethical review board.
Results
Over a 9 year period, a total of 159 patients with penetrating chest injury were analyzed. In total, 89 % (n = 141) were male and 11 % (n = 18) female. The mean age was 35 years (range 14–75). Most penetrating chest injuries were caused by stabbings or gunshots, 73 % (n = 116) and 21 % (n = 34), respectively (Table 1). Other causes included mostly work-related injuries.
All patients presented in the trauma resuscitating room were assessed according to the Advanced Trauma Life Support (ATLS) guidelines. During primary survey, heart rate (HR), SBP and Glasgow Coma Scale (GCS) were registered. Prehospital resuscitation was performed using crystalloid fluids. Twenty-one patients (13 %) were intubated before admission. The mean heart rate was 94 (±22) beats per minute. In 15.8 % of all patients, the SBP was below 90 mmHg. The median GCS was 14 (range 3–15). Only six patients had a GCS of 3. In 6.2 % of the cases the GCS was below nine. In the non intubated patients, the mean GCS at admission was 14. The mean GCS in the intubated patients was 13.
Laboratory findings were obtained by using the emergency laboratory services. In patients with penetrating chest injury, hematological and biochemical analyses were made immediately after presentation. The mean number of platelets in patients was 246 × 10e9/L (±94) and the mean number of white blood cells was 11.2 × 9e10/L (±5.1). In male patients, the mean hemoglobin level (Hb) was 8.2 mmol/L (±1.2) and in 49 % of the cases below 8.5 mmol/L, the inferior level of normal for males. In female patients, the mean Hb was 7.0 mmol/L (±1.0) and 78 % of all women presented had a mean Hb below 7.5 mmol/L, the inferior level of normal for females.
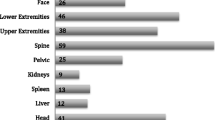
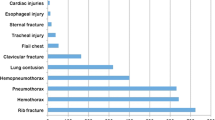
Using physical examination, diagnostic imaging and exploratory operation, types and locations of injury were determined. Ten patients (6.3 %) had cardiac injury. The most common injury was pneumothorax, this occurred in 24.5 % (n = 39) of all patients. Hemo-pneumothorax and hemothorax occurred less often, 13.2 % (n = 21) and 14.5 % (n = 23), respectively. Two of the patients suffered from a bilateral pneumothorax. Diaphragmatic injuries were seen in 13 (8.2 %) patients. Rib fractures were seen in 11 patients (7 %) with a mean number of 1.3 fractures. Other types of injuries include pneumomediastinum. The median ISS of all patients was 12 (range 1–50).
Most patients could be managed conservatively. Almost half (n = 78) were treated using chest tube drainage. Alternatively, surgical treatment was performed in 24 % (n = 38) of all patients. In the thoracic surgical treated group, the anterolateral incision was used in 63.3 % (n = 19) to gain access to the thoracic cavity. In 30 % (n = 9), a midsternotomy was used and in 6.6 % (n = 2) a combination of both approaches. Only in two patients, video-assisted thoracoscopic surgery (VATS) was performed as primary intervention. In 22 (14 %) patients, a laparotomy was performed due to severe abdominal injuries.
Surgically and non-surgically treated groups were compared. We found significant differences in clinical presentation, laboratory findings, mortality rate and length of hospital stay. Patients treated surgically had a significant lower SBP, GCS and hemoglobin levels. Also the ISS, mortality and length of hospital stay differed as these were significantly higher in the surgical treated group (Table 2).
Among all patients, 16.9 % were admitted to the ICU with a mean stay of 2.9 days.
In 18 patients (11 %), complications occurred. Half of these complications were infectious. Five patients developed sepsis. Seven of these complications were respiratory, mostly based on atelectasis. Obstructive shock was described in one patient, due to pulmonary embolism. Other type of complications include consistent bleeding. The overall 30-day mortality was 7.5 % (n = 12). Eight (67 %) of the diseased patients suffered from gunshot wounds.
When only including patients with an ISS of 16 or above, no statistical differences were seen in length of hospital stay, length of ICU stay and mortality (Table 3).
Discussion
Our study displays the management and outcome of patients with penetrating chest injury in an urban level I trauma center in the Netherlands for a period of 9 years. In penetrating chest injury, maintenance of the airway, intravascular volume resuscitation, assessment of pneumothorax, hemothorax, hemo-pneumothorax, or tension pneumothorax and evaluation of open chest wounds are the objectives during primary survey [5]. Conservative or surgical treatment is based upon abnormalities during physical examination and radiographic findings.
Most patients in our study were conservatively treated. Almost half of the patients were treated with chest tube drainage. These findings are comparable with the current literature [6]. Indications for conservative treatment using chest tube drainage were mainly pneumothorax and pleural fluid collections [7].
In total, 24 % of our patients were treated surgically by explorative thoracotomy. This percentage is higher in comparison to findings in comparable studies. This is most likely due to the severity of the injury [8, 9]. In areas such as war zones or areas with civil disorder, explorative thoracotomy rates can reach 80 % of the cases [8, 10]. Another reason might be due to the direct access to OR facilities for HD instable patients at our facility. This may blur the difference between a strict explorative thoracotomy and a resuscitative thoracotomy, since resuscitation is a continuous process. As expected, the rate of thoracotomy in patients sustaining gunshot wounds was 50 % higher compared to thoracotomy rates in patients with stab wounds. This is because gunshot wounds are associated with more tissue destruction due to the high kinetic energy transfer. Tissue with lower specific gravity absorbs less kinetic energy, therefore the destruction and devitalisation in lung tissue is less than in other solids organs [2].
In our series, indication for thoracotomy included initial chest tube output of over 1500 cc, continuous loss of blood during drainage, hemodynamic deterioration, radiographic evidence of retained hemothorax and/or clinical evidence of pericardial tamponade. However, worldwide there is no clear consensus on indications for thoracotomy in penetrating chest injury. Some studies conclude that initial chest tube outcome is not a determining factor for the level of total blood loss and therefore surgical intervention in cases of lower volume loss, such as more than 800 cc is necessary [11, 12].
Using the indications mentioned above, we found differences between the surgical- and non-surgical group in clinical presentation, laboratory findings, mortality rate and length of hospital stay. These differences may be explained by the lower ISS score in the non-surgical group. When comparing high ISS groups, these differences do not occur.
Different approaches have been described in performing thoracotomy. In our study, the anterolateral approach was mostly used (63 %). In 30 % of the cases, a midsternotomy was performed. The midsternotomy was mainly used in patients with cardiac injury. Cardiac injury can be treated surgically by using both anterolateral and midsternal approaches. However, the midsternotomy gives better access to all major structures, especially the right side of the heart and the hilus of the right lung, compared to the anterolateral approach. In addition, by using a midsternotomy, a cardiopulmonary bypass can be achieved [13]. In 6.6 % of the patients, both anterolateral and midsternal approach was used. VATS was performed in only 1.3 % of the patients, as thoracotomy is still seen as the standard procedure in treating penetrating chest injury [14]. Most trauma surgeons in the Netherlands do not perform a VATS procedure on a regular basis.
The overall 30-day mortality rate in our study was 7.5 %. In comparable studies the mortality ranges from 2.1 to 10.8 % [3, 15].
We collected our data retrospectively using Trauma Registry Database, Patient Information System and medical records. The retrospective nature of this study and the use of medical records give this study some limitations. The results were accordingly presented. The information in the medical records of blood transfusion was limited. Therefore, those data are not presented.
According to the results of our evaluation, patients with penetrating chest injury are not uncommon anymore in the Netherlands and most can safely be treated with chest tube drainage only. Although a smaller, hemodynamic severe compromised, group of patients may benefit from early surgical treatment. Management in selected hemodynamic stable patients for diagnostic and therapeutic purposes could probably be improved by training Dutch trauma surgeons in VATS techniques instead of using ‘open’ thoracotomy. Overall, a stepwise and consistent approach in the management of these patients is needed for a good outcome.
References
Robinson PD, Harman PK, Trinkle JK, Grover LG. Management of penetrating lung injuries in civilian practice. J Thorac Cardiovasc Surg. 1988;95:184–90.
Mandal AK, Sanusi M. Penetrating chest wounds: 24 years experience. World J Surg. 2001;25:1145–9.
Onat S, Ulku R, Avci A, Ates G, Ozcelik C. Urgent thoracotomy for penetrating chest trauma: analysis of 158 patients. Injury. 2011;42:900–4.
Hirshberg A, Or J, Stein M, Walden R. Transaxial gunshot injuries. J Trauma. 1996;41:460–1.
American College of Surgeons. Trauma Life Support Instructor Manual. Chicago 1993; pp. 113–125.
Tariq UM, Faruque A, Ansari H, Ahmad M, Rashid U, Perveen S. Changes in the patterns, presentation and management of penetrating chest trauma patients at a level II trauma centre in Southern Pakistan over the last two decades. Interact CardioVasc Thorac Surg. 2011;12:24–7.
Gambazzi F, Schirren J. Thoracic drainage. What is evidence based? Chirurg. 2003;74:99–107.
Zakhari AT. Thoracic battle injuries in Lebanon war: review of the early operative approach in 1,992 patients. Ann Thorac Surg. 1985;40:209–13.
van Waes OJF, van Riet PA, van Lieshout EMM, Hartog DD. Immediate thoracotomy for penetrating injuries: ten years’ experience at a Dutch level I trauma center. Eur J Trauma Emerg Surg. 2012;38:543–51.
Suleman ND, Rasoul HA. War injuries of the chest. Injury. 1985;16:382–4.
Siemens R, Polk HC Jr, Gray LA Jr, Fulton RL. Indications for thoracotomy following penetrating thoracic injury. J Trauma. 1977;17:493–500.
Kish G, Kozloff L, Joseph WL, Adkins PC. Indications for early thoracotomy in the management of chest trauma. Ann Thorac Surg. 1976;22:23–8.
Kupferschmid JP, Stein D, Aldea GS. Rupture of the right atrium secondary to blunt cardiac injury. J Card Surg. 1995;10:285–7.
Dutta R, Kumar A, Das CJ, Jindal T. Emergency video-assisted thoracoscopic foreign body removal and decortication of lung after chest trauma. Gen Thorac Cardiovasc Surg. 2010;58:155–8.
Sukul DM, de Zeeuw GR, Brummelkamp WH. Sharp thoracic injury. Injury. 1989;20:22–6.
Conflict of interest
C. Heus, J. J. Mellema, G. F. Giannakopoulos and W. P. Zuidema declare that they have no conflict of interest.
Compliance with ethical requirements
According to Dutch regulation, retrospective medical data analysis does not require consent by the medical ethical review board.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Heus, C., Mellema, J.J., Giannakopoulos, G.F. et al. Outcome of penetrating chest injuries in an urban level I trauma center in the Netherlands. Eur J Trauma Emerg Surg 45, 461–465 (2019). https://doi.org/10.1007/s00068-015-0533-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-015-0533-9