
Objective:
To verify whether the treatment of brain oligometastases with whole-brain radiotherapy (WBRT) plus stereotactic radiotherapy (SRT) or surgical resection results in different outcomes.
Methods:
Files of patients affected by brain metastases submitted to surgical resection followed by WBRT (group A) or WBRT + SRT (group B) were retrospectively selected for this study. The two treatment groups were matched for the following potential prognostic factors: WBRT schedule, age, gender, performance status, tumor type, number of brain metastases, extra-cerebral metastases, and recursive partitioning analysis class (RPA). The outcomes of patients in both groups were evaluated in terms of toxicity, local control, and overall survival.
Results:
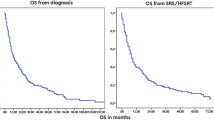
Total of 97 patients were selected (56 male; 42 female) who were respectively submitted to surgical resection followed by WBRT (group A, n = 50 patients) or WBRT + SRT (Group B, n = 47 patients). Median follow-up was 95 months (range, 8–171 months). The 1-year local control rates were 46.0% and 69.0% respectively. No significant difference in local tumor control was observed between group A and B (p = 0.10). Median overall survival was 15 and 19 months in group A and B, respectively. One-year survival was 56.0% and 62%, respectively. No difference was observed in the two groups (p = 0.40).
Conclusion:
Surgery remains the main therapeutic approach in symptomatic patients; nevertheless, our data support the use of WBRT plus SRT in one or two brain metastases smaller than 3 cm.
Zielsetzung:
Zu untersuchen, ob die Behandlung von Oligohirnmetastasen mit Ganzhirnbestrahlung (whole-brain radiotherapy, WBRT) plus stereotaktischer Radiotherapie (SRT) oder chirurgischer Resektion unterschiedliche Ergebnisse bringt.
Methoden:
Krankenakten von Patienten mit operativ entfernten Hirnmetastasen und anschließender WBRT (Gruppe A) oder WBRT + SRT (Gruppe B) wurden retrospektiv für diese Studie ausgewählt. Die zwei Beghandlungsarme wurden für folgende prognostische Parameter gematcht: WBRT-Schema. Alter, Geschlecht, Allgemeinzustand, Art des Primärtumors, Anzahl der Hirnmetastasen, extrazerebrale Metastasen, Recursive-Partioning-Analysis-(RPA-)Klasse. Das Behandlungsergebnis für beide Patientengruppen wurde im Hinblick auf Toxizität, lokale Tumorkontrolle und Gesamtüberleben bewertet.
Ergebnisse:
Insgesamt wurden 97 Patienten ausgewählt (56 m; 42 w), die entweder mit operativer Entfernung und anschließender WBRT (Gruppe A, n = 50 Pat.) oder mit WBRT + SRT (Gruppe B, n = 47 Pat.) behandelt wurden. Die mediane Beobachtungszeit betrug 95 Monate (Spanne 8–171). Die lokale Tumorkontrolle nach 1 Jahr betrug 46,0% (Gruppe A) und 69,0% (Gruppe B), ohne dass dieser Unterschied statistisch signifikant wäre (p = 0,10). Das mediane Gesamtüberleben betrug jeweils 15 und 19 Monate in Gruppe A and B. Die 1-Jahres-Überlebensrate betrug jeweils 56,0% and 62%. Es wurde kein Unterschied zwischen den beiden Gruppen gefunden (p = 0,40).
Schlussfolgerung:
Die chirurgische Entfernung bleibt die Behandlungsoption bei symptomatischen Patienten. Unsere Daten sprechen für eine Behandlung mit WBRT plus SRT bei Vorliegen von ein oder zwei Hirnmetastasen, die kleiner als 3 cm sind.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Buhmann Kirchhoff S, Becker C, Duerr HR et al. Detection of osseous metastases of the spine: comparison of high resolution multi-detector-CT with MRI. Eur J Radiol 2009;69:567–573.
Catton C, O’sullivan B, Bell R et al. Chordoma: long-term follow-up after radical photon irradiation. Radiother Oncol 1996;41:67–72.
Cummings BJ, Hodson DI, Bush RS. Chordoma: the results of megavoltage radiation therapy. Int J Radiat Oncol Biol Phys 1983;9:633–642.
Emami B, Lyman J, Brown A et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys 1991;21:109–122.
Freundt K, Meyners T, Bajrovic A et al. Radiotherapy for oligometastatic disease in patients with spinal cord compression (MSCC) from relatively radioresistant tumors. Strahlenther Onkol 2010;186:218–223.
Gabriele P, Macias V, Stasi M et al. Feasibility of intensity-modulated radiation therapy in the treatment of advanced cervical chordoma. Tumori 2003;89:298–304.
Kim B, Soisson ET, Duma C et al. Image-guided helical tomotherapy for treatment of spine tumors. Clin Neurol Neurosurg 2008;110:357–362.
Mahan SL, Ramsey CR, Scaperoth DD et al. Evaluation of image-guided helical tomotherapy for the retreatment of spinal metastasis. Int J Radiat Oncol Biol Phys 2005;63:1576–1583.
Mamitz S, Stromberger C, Kawgan-Kagan M et al. Helical tomotherapy in cervical cancer patients: simultaneous integrated boost concept: technique and acute toxicity. Strahlenther Onkol 2010;186:572–579.
Marcus RB, Jr., Million RR. The incidence of myelitis after irradiation of the cervical spinal cord. Int J Radiat Oncol Biol Phys 1990;19:3–8.
Pirzkall A, Carol M, Lohr F et al. Comparison of intensity-modulated radiotherapy with conventional conformal radiotherapy for complex-shaped tumors. Int J Radiat Oncol Biol Phys 2000;48:1371–1380.
Rochet N, Sterzing F, Jensen A et al. Helical tomotherapy as a new treatment technique for whole abdominal irradiation. Strahlenther Onkol 2008;184:145–149.
Scarabino T, Perfetto F, Giannatempo GM et al. [Imaging with magnetic resonance imaging of the operated cervical spine]. Radiol Med 1996;92:671–676.
Schultheiss TE, Kun LE, Ang KK et al. Radiation response of the central nervous system. Int J Radiat Oncol Biol Phys 1995;31:1093–1112.
Schulz-Ertner D, Karger CP, Feuerhake A et al. Effectiveness of carbon ion radiotherapy in the treatment of skull-base chordomas. Int J Radiat Oncol Biol Phys 2007;68:449–457.
Sterzing F, Herfarth K, Debus J. IGRT with helical tomotherapy-effort and benefit in clinical routine. Strahlenther Onkol 2007;183(Spec No 2):35–37.
Sterzing F, Sroka-Perez G, Schubert K et al. Evaluating target coverage and normal tissue sparing in the adjuvant radiotherapy of malignant pleural mesothelioma: helical tomotherapy compared with step-and-shoot IMRT. Radiother Oncol 2008;86:251–257.
Sterzing F, Welzel T, Sroka-Perez G et al. Reirradiation of multiple brain metastases with helical tomotherapy. A multifocal simultaneous integrated boost for eight or more lesions. Strahlenther Onkol 2009;185:89–93.
Sterzing F, Hauswald H, Uhl M et al. Spinal cord sparing reirradiation with helical tomotherapy. Cancer 2010;116:3961–3968.
Stoiber EM, Lechsel G, Giske K et al. Quantitative assessment of image-guided radiotherapy for paraspinal tumors. Int J Radiat oncol Biol Phys 2009:45:933–940.
Terezakis SA, Lovelock DM, Bilsky MH et al. Image-guided intensity-modulated photon radiotherapy using multifractionated regimen to paraspinal chordomas and rare sarcomas. Int J Radiat Oncol Biol Phys 2007;69:1502–1508.
Thariat J, Castelli J, Chanalet S, et al. CyberKnife stereotactic radiotherapy for spinal tumors: value of computed tomographic myelography in spinal cord delineation. Neurosurgery 2009;64:A60–A66.
Verhey LJ. Comparison of three-dimensional conformal radiation therapy and intensity-modulated radiation therapy systems. Semin Radiat Oncol 1999;9:78–98.
Yamada Y, Lovelock DM, Bilsky MH. A review of image-guided intensity-modulated radiotherapy for spinal tumors. Neurosurgery 2007;61:226–235; discussion 235.
Zibold F, Sterzing F, Sroka-Perez G et al. Surface dose in the treatment of breast cancer with helical tomotherapy. Strahlenther Onkol 2009;185:574–581.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
D’Agostino, G.R., Autorino, R., Pompucci, A. et al. Whole-Brain Radiotherapy Combined with Surgery or Stereotactic Radiotherapy in Patients with Brain Oligometastases. Strahlenther Onkol 187, 421–425 (2011). https://doi.org/10.1007/s00066-011-2228-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-011-2228-4