
Abstract
Purpose
Despite improved techniques and sophisticated postinterventional care, symptomatic intracranial hemorrhage (sICH) remains the most feared complication of mechanical thrombectomy (MT). Based on peri-interventional parameters, we aimed to discover which patients have a higher risk of sICH.
Methods
From March 2017 until March 2020 consecutive patients with acute ischemic stroke (AIS) and confirmed large-vessel occlusion who underwent MT were analyzed retrospectively. Demographic, clinical, and radiological variables and parameters specific to thrombectomy were reviewed. A univariate analysis was performed and statistically significant variables were included in a logistic regression model to identify independent factors predictive of sICH.
Results
A total of 236 patients with confirmed large-vessel occlusion were included and 22 (9.3%) had sICH. Univariate predictors of sICH included diabetes mellitus, glucose > 11.1 mmol/L, creatinine clearance (CrCl) ≤ 30 ml/min/1.73, ASPECTS indicating pretreatment infarct size, acute internal carotid artery (ICA) occlusion, stent implantation, tirofiban use, time from symptom onset to groin puncture > 4.5 h and high contrast medium consumption. In the adjusted analysis, ASPECTS < 6 (OR 3.673, p = 0.041), and amount of contrast injected ≥ 140 ml (OR 5.412, p = 0.003) were independent predictors of sICH, but not any more baseline glucose > 11.1 mmol/L (OR 1.467, p = 0.584), CrCl ≤ 30 ml/min/1.73 (OR 4.177, p = 0.069), acute ICA occlusion (OR 2.079, p = 0.181), stent implantation (OR 0.465, p = 0.512), tirofiban use (OR 5.164, p = 0.167), and time from onset-to-groin puncture (OR 1.453, p = 0.514).
Conclusion
The amount of contrast medium used is a modifiable factor associated with sICH. This association is novel and may be related to the neurotoxicity of the contrast medium disrupting the blood-brain barrier.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In real-world practice, the rate of symptomatic intracranial hemorrhage (sICH) after mechanical thrombectomy (MT) varies from 4% to 16% [1,2,3,4]. Several factors have been associated with sICH, such as older age [5, 6], high glucose levels [7, 8], low Alberta Stroke Program Early CT Score (ASPECTS) [5, 7, 8], high National Institutes of Health Stroke Scale (NIHSS) on admission [6], grade of recanalization [6, 7], angiographic poor collaterals [5, 8], treatment with intra-arterial thrombolytics (GPIIb/IIIa inhibitor) [9], and renal impairment [10]. Given the severe short-term and long-term consequences of sICH, including higher mortality [2], it is essential to identify modifiable factors associated with the risk of sICH to optimize current procedures.
The administration of iodine-containing contrast media (CM) in radiological interventions is related to adverse reactions, such as transient cortical blindness (most common), transient focal neurological deficits, seizures [11], and in some instances, cerebral edema [12] and death [13]. These manifestations are also known as contrast-induced encephalopathy (CIE), which has primarily been studied in patients undergoing coronary angiography [11], and it can radiologically mimic subarachnoid hemorrhage [11, 14, 15]. CIE is a rare condition during neuroradiological interventions with an incidence as low as 0.38% [16]. CIE was also observed after MT: out of 421 patients who underwent this procedure, CIE was seen in 7 patients (1.7%) [17]. Contrast extravasation (CE) indicates blood-brain barrier damage [18] and has been reported as an independent risk factor of hemorrhagic transformation and poor outcome after MT [19]. Prior to the MT era, a study in acute ischemic stroke (AIS) and intra-arterial thrombolysis with recombinant tissue plasminogen activator (rtPA) showed that contrast injection through the microcatheter was associated with intracranial hemorrhage. The higher the number of injections via the microcatheter, the higher the intracranial bleeding rate, suggesting a dose-dependent effect [20]. The elimination of contrast medium by renal excretion is delayed in patients with renal failure. Delayed excretion causes a greater exposure of the BBB to CM, contributing again to a vicious circle with greater BBB permeability and increased risk of sICH.
However, the role of CM dosage during MT and its impact on the risk of sICH has not been well established.
Material and Methods
Data collection and retrospective analysis was approved by the ethic committee of the Heinrich-Heine-University Düsseldorf (2020-1131). We used the STROBE case-control checklist [21]. We retrospectively analyzed all patient files with AIS and proximal large vessel occlusion (LVO) on the computed tomography (CT) or magnetic resonance (MR) angiogram who underwent MT in our institution (Kliniken Maria Hilf) between March 2017 and March 2020. Patients with symptom onset within 24 h from the last known normal time and follow-up imaging within 36 h after thrombectomy were included. Patients with symptom onset within 4.5 h before admission and without any contraindications to thrombolysis were primarily treated with intravenous alteplase according to national [22] and international guidelines [23].
For diagnostic CT-Angiography (CT-A), all patients received a 60 ml bolus of the non-ionized contrast medium Iomeprol. For CT-Perfusion (CT-P) imaging, a dose of 40 ml of the same contrast medium was given.
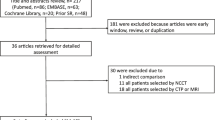
During the study period 263 acute ischemic stroke patients with LVO were diagnosed, out of which 236 patients were included in this study. Reasons for exclusion were lack of follow-up CT imaging or MRI within 36 h after thrombectomy, spontaneous recanalization, recanalization due to thrombolysis before thrombectomy, or early death before control imaging (Fig. 1).

Flow chart of patients who were eligible for mechanical thrombectomy between March 2017 and March 2020. CT computed tomography, LVO large-vessel occlusion, MRI magnetic resonance imaging
Mechanical Thrombectomy
The MT was performed by an experienced neuroradiologist (AR) or by a neuroradiologist in training under the experienced neuroradiologists’ supervision. The MT was performed with the direct aspiration first pass technique (ADAPT), rarely with a stent retriever alone, or mainly with the stent retriever-assisted, vacuum-locked extraction (SAVE) technique. If the ipsilateral internal carotid artery (ICA) was occluded, the decision of carotid stent implantation and the use of an intra-arterial antiplatelet agent (tirofiban) was left to the judgment of the treating neuroradiologist. For the MT the contrast medium Iomeprol with 350 mg iodine/ml (Imeron 350®, Bracco Imaging Deutschland GmbH, Konstanz, Germany) was used. Iomeprol is a non-ionic iodinated and low-osmolar (618 mosmol/kg) contrast agent. The contrast medium was administered via the guide catheter. During thrombectomy with a stent retriever, a super-selective angiogram was additionally performed with the help of a microcatheter.
Data Collection and Variables
We analyzed age and sex as demographic variables, and history of diabetes mellitus, arterial hypertension, atrial fibrillation, and stroke severity according to the National Institutes of Health Stroke Scale (NIHSS) as clinical variables. The laboratory variables considered were blood glucose, hemoglobin, white blood cell count, platelet count, creatinine, creatinine clearance, and international normalized ratio (INR). We also considered the medication prior to admission, particularly the use of antiplatelet agents (yes or no; and if yes, monotherapy or dual therapy) and oral anticoagulants. The radiological variables were the size of the pretreatment infarction core measured with ASPECTS [24] for anterior circulation stroke and pc-ASPECTS [25] for posterior circulation infarcts, the site of occlusion (internal carotid artery, anterior cerebral artery, M1 or M2 segment of the middle cerebral artery, posterior cerebral artery or basilar artery) and time from symptom onset to groin puncture. After the procedure, the reperfusion rate was evaluated with the modified thrombolysis in cerebral infarction (mTICI) score [26]. In addition, the door to groin time and the amount (ml) of contrast agent administered during MT and for diagnostic CTA and CT perfusion were evaluated.
Symptomatic Intracranial Hemorrhage
A sICH was defined according to the European Cooperative Acute Stroke Study (ECASS) III as “apparently extravascular blood in the brain or within the cranium that was associated with clinical deterioration, as defined by an increase of ≥ 4 points of the NIHSS score or that lead to death and that was identified as the predominant cause of the neurological deterioration” [27]. The clinical diagnosis of sICH was made by the treating physician and confirmed by a stroke neurologist.
Statistical Analysis
The statistical analysis was performed with SPSS software Version 27 (IBM Corp, Armonk, NY, USA). Shapiro-Wilk test was used to check for normal distribution. Differences between the groups were analyzed with the Mann-Whitney U‑test for continuous variables without normal distribution, and t‑test was used for continuous variables with normal distribution. For categorical variables, x2 test or Fisherʼs exact test was used. P values < 0.05 were considered statistically significant. For statistically significant variables, binary logistic regression models were applied.
Results
A total of 236 patients were included in the final study analysis. The mean age at AIS was 73 ± 13 years (range 23–99 years), and 134 (56.8%) were women. 22 patients (9.3%) had post-MT sICH. 189 patients (80.1%) underwent CT-A as a diagnostic tool; 87 (36.9%) received a CT‑P additionally. In 47 patients (19.9%), an MRI was performed before MT. The median dose of contrast used during MT was 42 ml in the non-sICH group and 73.5 ml in the sICH group, p = < 0.001. The total median contrast applied for diagnostic (CT‑A with or without CT-P) plus contrast amount used in the MT was 118 ml in the non-sICH group and 160 ml in the sICH group, p = 0.001.
The mean number of passes, which refers to the number of attempts to recanalize the occluded vessel, with available data of 134 (57%) patients, was 2.04 (standard deviation, SD ± 1.35). Subgroup analyses revealed that the non-sICH group had a mean of 1.95 passes (SD ± 1.29), and the sICH group of 2.80 passes (SD ± 1.61, p = 0.018). The difference between the two groups was statistically significant and is worth considering for further considerations; however, since the available data only corresponded to 57% of the total cohort, we decided not to include them in the final statistical analyses.
In univariate analysis, variables associated with sICH included history of diabetes mellitus (36.4% vs. 17.8%, p = 0.036), blood glucose > 11.1 mmol/L on admission (22.7% vs. 7.5%, p = 0.033), CrCl ≤ 30 (18.2% vs. 5.6%, p = 0.025), ASPECTS (median 7 vs. 9, p = 0.008), ASPECTS dichotomized ≤ 6 (45.5% vs. 17.3%, p = 0.002), acute ICA occlusion (50% vs. 25.2%, p = 0.013), carotid stent implantation (31.8% vs. 14%, p = 0.029), tirofiban use (27.3% vs. 8.4%, p = 0.005), time from onset-to-groin > 4.5 h (36.4% vs. 16.2%, p = 0.021) and total volume of contrast medium administered for diagnostic imaging and during MT (median 160 ml vs. 118 ml, p = 0.001), as well as total volume of contrast medium administered only during the MT procedure (median 73.5 ml vs. 42 ml, p = < 0.001) (Table 1).
Because of the wide overlap between baseline glucose > 11.1 mmol/L and diabetes mellitus, we arbitrarily decided to include only baseline glucose > 11.1 mmol/L for the subsequent regression analysis. We could not document the number of maneuvers to achieve reperfusion in all patients, but the median time of the duration of MT in the non sICH group was 34 min vs. 48.5 min in the sICH group, p = 0.003.
Variables with a P value of < 0.05 in the univariate analysis were included in the multivariable logistic regression model (Table 2). Model 1 included ASPECTS and CM amount as continuous variables: baseline glucose > 11.1 mmol/L (OR 1.401, 95% CI 0.354–5.540, p = 0.630), CrCl ≤ 30 ml/min/1.73 (OR 4.445, 95% CI 0.969–20.391, p = 0.055), ASPECTS (OR 0.749, 95% CI 0.625–0.899, p = 0.002), acute ICA occlusion (OR 1.529, 95% CI 0.511–4.578, p = 0.448), stent implantation (OR 0.475, 95% CI 0.045–4.964, p = 0.534), tirofiban use (OR 6.750, 95% CI 0.615–74.134, p = 0.118), time from onset-to-groin > 4.5 h (OR 1.121, 95% CI 0.317–3.964, p = 0.859), and amount of CM used (OR 1.129, 95% CI 1.019–1.250, p = 0.020).
In model 2, ASPECTS score and contrast media amount were dichotomized (ASPECTS < 6 or ≥ 6 and contrast media with a predefined cut-off of ≥ 140 ml) with the following results:
baseline glucose > 11.1 mmol/L (OR 1.467, 95% CI 0.373–5.775, p = 0.584), CrCl ≤ 30 ml/min/1.73 (OR 4.177, 95% CI 0.894–19.528, p = 0.069), acute ICA occlusion (OR 2.079, 95% CI 0.711–6. 079, p = 0.181), stent implantation (OR 0.465, 95% CI 0.047–5.576, p = 0.512), and tirofiban use (OR 5.164, 95% CI 0.505–52.863, p = 0.167) were no longer significant, whereas ASPECTS < 6 (OR 3.673, 95% CI 1.055–12.792, p = 0.041), CM amount ≥ 140 ml (5.412, 95% CI 1.770–16.551, p = 0.003) were still significantly associated with sICH.
In a model where only the contrast medium used during MT (per 10 ml) is taken into account, its association with the risk of sICH remained significant (OR 1.445 95% CI 1.028–1.275, p = 0.014).
In summary, according to the logistic regression, ASPECTS ≤ 6 and procedural contrast media dose ≥ 140 ml were independent predictors of sICH in our cohort.
Discussion
Following acute ischemic stroke, hemorrhagic transformation of the brain parenchyma is multifactorial and, in some cases, represents part of the natural history of reperfusion and the ischemic process per se [18]. Disruption of the BBB after reperfusion treatment is associated with hemorrhagic transformation [28] but may even lead to pronounced intracerebral bleeding. Which modifiable factors play a role in sICH is not entirely clear but identifying these factors could reduce the risk of sICH and its associated morbidity and mortality. In particular, the abrupt increase in perfusion pressure following MT may lead to a reperfusion injury enhancing tissue damage [18, 29]. Another intriguing risk factor appears to be the amount of CM given during the MT procedure. This study reports an independent association between CM amounts ≥ 140 ml and sICH. In addition, we replicated the impact of several known predictors of sICH.
Contrast media are considered neurotoxic since they increase the BBB permeability due to their toxic effect on the basal lamina [18]. Contrast media neurotoxicity is thought to be due to their hyperosmolarity compared to blood. Non-ionized CM have less osmolarity than ionized ones. Due to their safer profile, non-ionized CM are preferred for most radiological interventions. Intra-arterial hyperosmolar solutions cause the exit of water from the endothelial cells, thus opening the tight junctions and allowing BBB damage [30]; however, a study in rabbits demonstrated greater BBB permeability with non-ionized CM than with mannitol, the osmolarity of which is twice that of the CM, suggesting that BBB damage occurs mainly due to their chemotoxic properties rather than due to hyperosmolarity [31]. Moreover, some evidence suggests that contrast-induced adverse reactions are related to injection dosage and speed. Patients with injection doses ≥ 100 ml and an injection speed of ≥ 5 ml/s were at higher risk of experiencing contrast-induced adverse reactions [32]. Although Kathri et al. demonstrated an association between higher numbers of contrast injections via microcatheter and intracranial hemorrhage, they could not demonstrate an association with the total dose of CM applied [20]. Therefore, our study adds a novel aspect regarding the CM used during MT and its association with sICH.
In animal studies, hyperglycemia has been associated with more extensive cerebral infarction, severe BBB disruption, and greater hemorrhagic transformation than normoglycemia [33]; however, unlike other studies in which baseline glucose was an independent predictor for sICH (such as the ASIAN score [8] or TAG score [7]), we were not able to prove baseline glucose as an independent predictive factor of sICH; however, in the univariate analysis, a subgroup with admission glucose ≥ 11.1 mmol/l showed a statistically significant increase in bleeding complications but statistical significance could not be replicated in the logistic regression.
Lower ASPECTS (≤ 6) is another well-known predictive factor for sICH and our findings are in concordance with previous studies [5, 7, 8].
Amazingly, incomplete reperfusion (TICI score < 2b) was not associated with sICH in the present study. A possible explanation for the lack of association in our study may relate to the low rates of incomplete reperfusion in both groups (13.6% vs. 13.1% in patients with and without sICH, respectively) as compared to the TAG score derivation study, where the incomplete reperfusion rates were much higher (15.3% in the no sICH group vs. 47.4% in the sICH group) [7].
We can deduce that patients with large cerebral infarcts leading to a severe disruption of the BBB, combined with high doses of CM for diagnostic and procedural purposes, are at particular risk of sICH because both these factors potentiate their damaging effect.
Based on our results, we hypothesize that patients with large cerebral infarction (ASPECTS ≤ 6) and high amounts of CM used during MT are at higher risk of sICH.
The group of sICH, as shown in Table 1, had higher glucose levels at presentation, had more frequent renal failure (measured by CrCl ≤ 30 ml/min/1.73), had lower ASPECT scores, and had more ICA occlusions. Those patients with ICA occlusion received an ICA stent and were treated with tirofiban post-procedurally, and the time from onset to groin puncture was > 4.5 h. One explanation why the sICH group received more CM is that these patients underwent significantly more stent implantations than the non-sICH group, and this intervention directly implies more lengthy procedures.
Limitations of our study include its relatively small sample size and retrospective, single-center design. We could not accurately document the time from onset to groin in an ordinal manner, only as categorical variable as (> or < 4.5 h), and the number of passes during MT to achieve reperfusion. The generalizability of our results without these details could be limited, and even though our sICH ranges are consistent with other publications [2, 4, 8], our results should be interpreted carefully. Since there is only evidence that microcatheter injections of CM are associated with intracranial hemorrhage, and no studies compared the CM amount with the incidence of sICH so far, it is impossible to reliably generate a cut-off value beyond the risk of sICH increases. The cut-off value we used (≥ 140 ml) was arbitrarily predefined. It is well-known that not all of the CM used is administered entirely to the patient; for example, some milliliters will be discarded when mixed with blood, and the difficulty of precisely measuring the amount of CM administered is also a limitation to consider. We do not include the number of passes or maneuvers in the statistical analysis because this information was only available in 57% of the cohort population.
Another point to consider is that in patients with more complicated interventions, the procedure takes longer. This is precisely the case in our study, where the procedures in the sICH group were significantly longer (p = 0.003), implying more maneuvers (passes) to achieve reperfusion and a more significant amount of CM complicating the interaction of adverse factors. Logically, the more passes for reperfusion are needed, the greater the amount of CM administered.
The collateral status is another important point that could not be evaluated in this retrospective study but should be considered in future prospective clinical trials since there is evidence that good collaterals are associated with decreased rates of sICH [34].
A crucial question for future clinical trials is whether the number of maneuvers needed for recanalization primarily facilitates intracranial bleeding due to mechanical side effects of the catheter leading to endothelial injury or whether the amount of CM favors intracranial bleeding as the main culprit.
Our study shows a clear association between the amount of CM used during MT with sICH, especially in patients with large infarcts.
Our main findings may also be of scientific relevance in that they could stimulate researchers to investigate the toxic role of CM during MT prospectively.
Summary
Although the scientific value of this study could be limited due to the small sample size, retrospective design, and lack of control of all potentially relevant factors, our study shows some evidence that the administration of CM should be carefully controlled both in the diagnostic and therapeutic part in patients with AIS.
This paper provides evidence that the amount of CM used during MT impacts the risk of sICH after that. Stroke teams should be aware that the dose of CM is an independent risk factor for sICH. More validation studies are necessary to clarify prospectively what amount of CM could be used safely in order to avoid intracranial hemorrhage after MT.
Abbreviations
- AIS:
-
Acute ischemic stroke
- ASIAN:
-
Alberta Stroke Program Early CT Score, Baseline Glucose, Poor Collateral Circulation, Passes with Retriever and Onset-to-Groin Puncture Time
- ASPECTS:
-
Alberta Stroke Program Early CT Score
- CIE:
-
Contrast-induced encephalopathy
- CM:
-
Contrast medium
- CrCl:
-
Creatinine clearance
- ICA:
-
Internal carotid artery
- LVO:
-
Large vessel occlusion
- MT:
-
Mechanical thrombectomy
- NIHSS:
-
National Institutes of Health Stroke Scale
- SAVE:
-
Stent retriever assisted vacuum-locked extraction
- sICH:
-
Symptomatic intracranial hemorrhage
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology
- TAG:
-
Thrombolysis in Cerebral Ischemia Score, Alberta Stroke Program Early CT Score, and Glucose Level.
References
Mokin M, Abou-Chebl A, Castonguay AC, Nogueira RG, English JD, Farid H, Gupta R, Martin C, Holloway WE, Haussen DC, Mueller-Kronast N, Zaidat OO; NASA and TRACK investigators. Real-world stent retriever thrombectomy for acute ischemic stroke beyond 6 hours of onset: analysis of the NASA and TRACK registries. J Neurointerv Surg. 2019;11:334–7.
Hao Y, Yang D, Wang H, Zi W, Zhang M, Geng Y, Zhou Z, Wang W, Xu H, Tian X, Lv P, Liu Y, Xiong Y, Liu X, Xu G; ACTUAL Investigators (Endovascular Treatment for Acute Anterior Circulation Ischemic Stroke Registry). Predictors for Symptomatic Intracranial Hemorrhage After Endovascular Treatment of Acute Ischemic Stroke. Stroke. 2017;48:1203–9.
Ospel JM, Qiu W, Menon BK, Mayank A, Demchuk A, McTaggart R, Nogueira RG, Poppe AY, Jayaraman M, Buck B, Haussen D, Roy D, Joshi M, Zerna C, Almekhlafi M, Tymianski M, Hill MD, Goyal M; ESCAPE-NA1 Investigators. Radiologic Patterns of Intracranial Hemorrhage and Clinical Outcome after Endovascular Treatment in Acute Ischemic Stroke: Results from the ESCAPE-NA1 Trial. Radiology. 2021;300:402–9.
Venditti L, Chassin O, Ancelet C, Legris N, Sarov M, Lapergue B, Mihalea C, Ozanne A, Gallas S, Cortese J, Chalumeau V, Ikka L, Caroff J, Labreuche J, Spelle L, Denier C. Pre-procedural predictive factors of symptomatic intracranial hemorrhage after thrombectomy in stroke. J Neurol. 2021;268:1867–75.
Boisseau W, Fahed R, Lapergue B, Desilles JP, Zuber K, Khoury N, Garcia J, Maïer B, Redjem H, Ciccio G, Smajda S, Escalard S, Taylor G, Mazighi M, Michel P, Gory B, Blanc R; ETIS Investigators. Predictors of Parenchymal Hematoma After Mechanical Thrombectomy: A Multicenter Study. Stroke. 2019;50:2364–70.
Cappellari M, Mangiafico S, Saia V, Pracucci G, Nappini S, Nencini P, Konda D, Sallustio F, Vallone S, Zini A, Bracco S, Tassi R, Bergui M, Cerrato P, Pitrone A, Grillo F, Saletti A, De Vito A, Gasparotti R, Magoni M, Puglielli E, Casalena A, Causin F, Baracchini C, Castellan L, Malfatto L, Menozzi R, Scoditti U, Comelli C, Duc E, Comai A, Franchini E, Cosottini M, Mancuso M, Peschillo S, De Michele M, Giorgianni A, Delodovici ML, Lafe E, Denaro MF, Burdi N, Internò S, Cavasin N, Critelli A, Chiumarulo L, Petruzzellis M, Doddi M, Carolei A, Auteri W, Petrone A, Padolecchia R, Tassinari T, Pavia M, Invernizzi P, Turcato G, Forlivesi S, Ciceri EFM, Bonetti B, Inzitari D, Toni D; Listing of IER Collaborators. IER-SICH Nomogram to Predict Symptomatic Intracerebral Hemorrhage After Thrombectomy for Stroke. Stroke. 2019;50:909–16. Erratum in: Stroke. 2019;50:e341.
Montalvo M, Mistry E, Chang AD, Yakhkind A, Dakay K, Azher I, Kaushal A, Mistry A, Chitale R, Cutting S, Burton T, Mac Grory B, Reznik M, Mahta A, Thompson BB, Ishida K, Frontera J, Riina HA, Gordon D, Parella D, Scher E, Farkas J, McTaggart R, Khatri P, Furie KL, Jayaraman M, Yaghi S. Predicting symptomatic intracranial haemorrhage after mechanical thrombectomy: the TAG score. J Neurol Neurosurg Psychiatry. 2019;90:1370–4.
Zhang X, Xie Y, Wang H, Yang D, Jiang T, Yuan K, Gong P, Xu P, Li Y, Chen J, Wu M, Sheng L, Liu D, Liu X, Xu G. Symptomatic Intracranial Hemorrhage After Mechanical Thrombectomy in Chinese Ischemic Stroke Patients: The ASIAN Score. Stroke. 2020;51:2690–6.
Neuberger U, Seker F, Schönenberger S, Nagel S, Ringleb PA, Bendszus M, Pfaff JAR, Möhlenbruch MA. Prediction of intracranial hemorrhages after mechanical thrombectomy of basilar artery occlusion. J Neurointerv Surg. 2019;11:1181–6.
Laible M, Jenetzky E, Möhlenbruch MA, Neuberger U, Bendszus M, Ringleb PA, Rizos T. Renal Impairment Is Associated with Intracerebral Hemorrhage after Mechanical Thrombectomy in Vertebrobasilar Stroke. Cerebrovasc Dis. 2019;47:48–56.
Spina R, Simon N, Markus R, Muller DW, Kathir K. Contrast-induced encephalopathy following cardiac catheterization. Catheter Cardiovasc Interv. 2017;90:257–68.
Junck L, Marshall WH. Fatal brain edema after contrast-agent overdose. AJNR Am J Neuroradiol. 1986;7:522–5.
Zhao W, Zhang J, Song Y, Sun L, Zheng M, Yin H, Zhang J, Wang W, Han J. Irreversible fatal contrast-induced encephalopathy: a case report. BMC Neurol. 2019;19:46.
Harada Y, Kairamkonda SR, Ilyas U, Pothineni NVK, Samant RS, Shah VA, Kapoor N, Onteddu S, Nalleballe K. Pearls & Oy-sters: Contrast-induced encephalopathy following coronary angiography: A rare stroke mimic. Neurology. 2020;94:e2491–4.
Velden J, Milz P, Winkler F, Seelos K, Hamann GF. Nonionic contrast neurotoxicity after coronary angiography mimicking subarachnoid hemorrhage. Eur Neurol. 2003;49:249–51.
Zhang G, Wang H, Zhao L, Li T, Sun M, Zhang Y, Hu H, Teng G, Chen J, Jian Y, Liu J. Contrast-Induced Encephalopathy Resulting From Use of Ioversol and Iopromide. Clin Neuropharmacol. 2020;43:15–9.
Chu YT, Lee KP, Chen CH, Sung PS, Lin YH, Lee CW, Tsai LK, Tang SC, Jeng JS. Contrast-Induced Encephalopathy After Endovascular Thrombectomy for Acute Ischemic Stroke. Stroke. 2020;51:3756–9.
Khatri R, McKinney AM, Swenson B, Janardhan V. Blood-brain barrier, reperfusion injury, and hemorrhagic transformation in acute ischemic stroke. Neurology. 2012;79(13 Suppl 1):S52–7.
Chen Z, Zhang Y, Su Y, Sun Y, He Y, Chen H. Contrast Extravasation is Predictive of Poor Clinical Outcomes in Patients Undergoing Endovascular Therapy for Acute Ischemic Stroke in the Anterior Circulation. J Stroke Cerebrovasc Dis. 2020;29:104494.
Khatri P, Broderick JP, Khoury JC, Carrozzella JA, Tomsick TA; IMS I and II Investigators. Microcatheter contrast injections during intra-arterial thrombolysis may increase intracranial hemorrhage risk. Stroke. 2008;39:3283–7.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344–9.
Ringleb PA, Hametner C, Köhrmann M, Frank B, Jansen O. Akuttherapie des ischämischen Schlaganfalls, S2e-Leitlinie. https://www.awmf.org/uploads/tx_szleitlinien/030-046l_S2e_Akuttherapie-des-ischaemischen-Schlaganfalls_2021-05.pdf. Accessed 10 Mar 2022
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–418. Erratum in: Stroke. 2019;50:e440–1.
Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet. 2000;355:1670–4. Erratum in: Lancet 2000;355:2170.
Puetz V, Sylaja PN, Coutts SB, Hill MD, Dzialowski I, Mueller P, Becker U, Urban G, O’Reilly C, Barber PA, Sharma P, Goyal M, Gahn G, von Kummer R, Demchuk AM. Extent of hypoattenuation on CT angiography source images predicts functional outcome in patients with basilar artery occlusion. Stroke. 2008;39:2485–90.
Almekhlafi MA, Mishra S, Desai JA, Nambiar V, Volny O, Goel A, Eesa M, Demchuk AM, Menon BK, Goyal M. Not all “successful” angiographic reperfusion patients are an equal validation of a modified TICI scoring system. Interv Neuroradiol. 2014;20:21–7.
Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, Larrue V, Lees KR, Medeghri Z, Machnig T, Schneider D, von Kummer R, Wahlgren N, Toni D; ECASS Investigators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–29.
Arba F, Rinaldi C, Caimano D, Vit F, Busto G, Fainardi E. Blood-Brain Barrier Disruption and Hemorrhagic Transformation in Acute Ischemic Stroke: Systematic Review and Meta-Analysis. Front Neurol. 2021;11:594613.
Janardhan V, Qureshi AI. Mechanisms of ischemic brain injury. Curr Cardiol Rep. 2004;6:117–23.
Brightman MW, Hori M, Rapoport SI, Reese TS, Westergaard E. Osmotic opening of tight junctions in cerebral endothelium. J Comp Neurol. 1973;152:317–25.
Wilson AJ, Evill CA, Sage MR. Effects of nonionic contrast media on the blood-brain barrier. Osmolality versus chemotoxicity. Invest Radiol. 1991;26:1091–4.
Li X, Liu H, Zhao L, Liu J, Cai L, Liu L, Zhang W. Clinical observation of adverse drug reactions to non-ionic iodinated contrast media in population with underlying diseases and risk factors. Br J Radiol. 2017;90:20160729.
Desilles JP, Syvannarath V, Ollivier V, Journé C, Delbosc S, Ducroux C, Boisseau W, Louedec L, Di Meglio L, Loyau S, Jandrot-Perrus M, Potier L, Michel JB, Mazighi M, Ho-Tin-Noé B. Exacerbation of Thromboinflammation by Hyperglycemia Precipitates Cerebral Infarct Growth and Hemorrhagic Transformation. Stroke. 2017;48:1932–40.
Qian J, Fan L, Zhang W, Wang J, Qiu J, Wang Y. A meta-analysis of collateral status and outcomes of mechanical thrombectomy. Acta Neurol Scand. 2020;142:191–9.
Acknowledgements
The authors thank Dr. Edna-Clarisse Cieslik-Köchling for her support during the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
E.R. Lopez-Navarro, C. Delfs, A. Jarre, V. Sanio, G. Greif, E.B. Ringelstein, C.-A. Haensch and A. Ringelstein declare that they have no competing interests. J. Gutierrez declares no conflict of interest related to this work but NIH grants unrelated to this work. S.G. Meuth received speaker honoraria and travel reimbursement from Almirall, Amicus Therapeutics Germany, Bayer Health Care, Biogen, Celgene, Diamed, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Novo Nordisk, ONO Pharma, Roche, Sanofi-Aventis, Chugai Pharma, QuintilesIMS and Teva, none related to this study. His research is supported by Bundesministerium für Bildung und Forschung (BMBF), Deutsche Forschungsgesellschaft (DFG), Else-Kröner-Fresenius-Stiftung, Deutscher Akademischer Austauschdienst, Hertie Stiftung, Interdisziplinäres Zentrum für Klinische Forschung (IZKF) Münster, Deutsche Stiftung Neurologie and Almirall, Amicus Therapeutics Germany, Biogen, Diamed, Fresenius Medical Care, Genzyme, Merck Serono, Novartis, ONO Pharma, Roche, und Teva, none related to this study. M. Ringelstein received speaker honoraria from Novartis, Bayer, Roche, Alexion and Ipsen and travel reimbursement from Bayer Schering, Biogen Idec, Merz, Genzyme, Teva, Grifols, Roche and Merck, none related to this study.
Rights and permissions
About this article

Cite this article
Lopez-Navarro, E.R., Delfs, C., Jarre, A. et al. Contrast Neurotoxicity and its Association with Symptomatic Intracranial Hemorrhage After Mechanical Thrombectomy. Clin Neuroradiol 32, 961–969 (2022). https://doi.org/10.1007/s00062-022-01152-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00062-022-01152-3