
Abstract
Purpose
Strategies for treating intracranial aneurysms of collateral vessels in adult onset moyamoya disease (MMD) remain unclear, because overall case numbers are limited and data on long-term outcomes are lacking. The aim of this study was to assess clinical and anatomic outcomes of such aneurysms in adult MMD sufferers who present with hemorrhage.
Methods
Of the 77 adult patients consecutively enrolled between January 2003 and December 2014 in the MMD registry at a single institution, those presenting with hemorrhage and followed for >12 months were studied. Aneurysms involving collateral vessels at sites of hemorrhage were considered culprit lesions.
Results
Aneurysms of collateral vessels in 19 patients (19/77, 24.7%) were confirmed as ruptured by conventional angiography. In five of these patients, obliterative endovascular embolization was successfully performed. The other 14 patients were managed conservatively due to lesion inaccessibility, and follow-up imaging studies (13 available) confirmed later disappearance of aneurysms in 12 patients (92.3%). In the aneurysm group (n = 19), re-bleeding occurred in 8 patients (42.1%) during follow-up (mean 67.4 ± 38.9 months). The re-bleeding involved contralateral hemispheres in 6 patients (75.0%), and all re-bleeding events occurred >6 months after initial hemorrhage. In the other 58 subjects without aneurysms 13 (22.4%) also suffered re-bleeding (mean follow-up 71.9 ± 46.3 months).
Conclusion
Although endovascular interventions are appropriate for ruptured aneurysms of collateral arteries in MMD, conservative treatment can be a viable alternative for technically inaccessible lesions.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In patients with moyamoya disease (MMD), who commonly suffer hemorrhagic or ischemic stroke, any intraparenchymal or intraventricular bleeding detected is typically attributed to the fragility of basal collateral vessels; however, such bleeding occasionally results from aneurysms or pseudoaneurysms arising in deep collateral perforators [1]. Collateral channels, namely perforator and choroidal arteries, are prone to development of aneurysms due to altered hemodynamics and inherent structural weakness [2]. Although not always found in hemorrhagic presentations of MMD, true or pseudoaneurysms may pose treatment challenges, given the considerable technical difficulties entailed in surgical or endovascular access and reports of suggested management are scarce [1]. Unless ruptured lesions are obliterated, a risk of re-bleeding remains. On the other hand, the fate of untreated ruptured aneurysms in MMD is unclear, so mandatory treatment is subject to controversy and weighing up of procedural risks. For this study, ruptured aneurysms of collateral vessels were monitored long-term in adults with hemorrhagic type MMD, analyzing clinical and anatomic outcomes. Our intent was to assess episodic re-bleeding in this setting, comparing rates in patients with and without ruptured aneurysms.
Materials and Methods
Patient Population
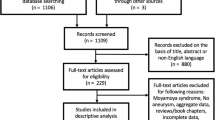
During a 12-year period (January 2003 to December 2014), 103 MMD registry entrants presenting with intracranial hemorrhage, i.e. intraventricular hemorrhage (IVH), intracerebral hemorrhage (ICH), and/or subarachnoid hemorrhage (SAH) were selected for a retrospective review. Aside from 13 instances of childhood onset (<18 years old) hemorrhagic MMD, all patients met the diagnostic criteria for adult MMD established by Kim et al. [3]. The endpoint of this study was change in status of collateral arterial aneurysms and re-bleeding during long-term follow-up of hemorrhagic MMD. One patient with SAH and rupture of a combination saccular aneurysm and 12 patients followed for <12 months were excluded (2 deaths and 1 vegetative state at initial hemorrhage and 9 lost to follow-up). Ultimately, 77 adults (female 57, male 20, mean age 39.7 ± 11.4 years) with hemorrhagic MMD (bilateral 65, unilateral 12) were investigated, collecting various patient variables (gender, age, hypertensive disease, family history, prior bypass surgery, and clinical presentation as ICH, IVH, or SAH) from medical records. Angiographic data were also retrieved, documenting presence/absence of aneurysms (as bleeding focus), their sizes and locations, or assigned Suzuki grades. To gauge the hemodynamic stress exerted on collateral vessels, dilatation and branching of channels (anterior choroidal and posterior communicating arteries) were assessed by angiogram [4].
In patients with confirmed aneurysms of collateral arteries, therapeutic alternatives (e.g. observation, open surgical and endovascular treatment) were discussed, based on a multidisciplinary benefit/risk evaluation. Accessibility of target lesion and volume/location of hematoma, were major considerations. This study was approved by our institutional review boards.
Angiographic Evaluation and Endovascular/Surgical Procedure
Digital subtraction angiography (DSA) was done routinely to diagnose MMD and to locate the origins of the hemorrhage. All lesions were graded by Suzuki system and stratified as aneurysm-related (aneurysm group) or unrelated (non-aneurysm group) hemorrhagic MMD. Rupture was presumed in any aneurysm of collateral arteries located in or adjacent to hematomas. In event of rupture, endovascular procedures were generally preferred. Thus, angioarchitectural explorations were conducted via Integris V (Philips Medical System, Best, The Netherlands) or Innova IGS 630 (GE Healthcare, Wauwatosa, WI) biplane system (including three-dimensional rotational angiography) to assess feeding arteries, determine sizes/locations of aneurysms, and plan access routes via collateral arteries. Patients with incidental aneurysms, unrelated to hemorrhage, were assigned to the non-aneurysm group.
All endovascular procedures entailed general anesthesia. N‑butyl cyanoacrylate (NBCA, Cordis Neurovascular, Miami Lakes, FL) and Berenstein liquid coils (Target Therapeutics, Fremont, CA) were used as embolic materials. Surgical treatments were confined to few patients whose aneurysms were inaccessible via endovascular approach.
Clinical and Image Follow-up
Immediate angiographic results after endovascular procedures were gauged as follows: complete occlusion (no contrast filling), subtotal occlusion (delayed or minimal residual filling of sac by collateral channels), and treatment failure (access failure or embolization failure). Imaging follow-up was customary to assess potential morphological change in all aneurysms of collateral arteries. Depending on clinical conditions, DSA was recommended within 1–3 months for this purpose, but computed tomography angiography (CTA) or magnetic resonance angiography (MRA) was also allowed as needed to match pretreatment testing. Clinical follow-up was advised in all patients every 3–6 months after discharge. Patient outcomes were measured using the modified Rankin scale (mRS).
Statistical Analysis
Continuous data were expressed as mean ± standard deviation (SD). The χ2-test and Fisher’s exact test or unpaired t-test were used to assess categorical or continuous variables, respectively. Average annual risk of re-bleeding was calculated as total re-bleeding patients divided by patient-year total for hemorrhagic MMD during the follow-up period. Statistical significance was set at p < 0.05, employing standard software (SPSS v19; SPSS, Chicago, IL) for all purposes.
Results
Patient Population
In our cohort (N = 77) of adult patients with hemorrhagic MMD, 20 aneurysms of collateral arteries were discovered, 19 of which were associated with hemorrhage. The other was encountered by chance and found contralateral to the hemorrhage. No angiographic basis for intracranial hemorrhage was evident in the remaining patients (n = 57). General characteristics of aneurysm and non-aneurysm patient subsets are summarized in Table 1.
In the aneurysm group, lesions were most often located on collaterals of the lateral posterior choroidal artery (11/19, 57.9%), followed by medial lenticulostriatal artery (3/19, 15.7%) and anterior choroidal artery (2/19, 10.5%). Lateral lenticulostriatal artery, medial posterior choroidal artery, and a collateral of anterior cerebral artery were involved as single occurrences (each 5.2%). Mean aneurysm size was 2.8 ± 0.9 mm and IVH was the most common type of intracranial hemorrhage (n = 15, 78.9%). All patients were Suzuki stage 3 (n = 10) or stage 4 (n = 9) at time of hemorrhage.
In the non-aneurysm (vs aneurysm) group, type of hemorrhage and Suzuki stage were similarly distributed, but bypass surgery after hemorrhage was elected more often; however, dilatation of posterior communicating artery (PcomA) or anterior choroidal artery (AchA) occurred more frequently in patients with aneurysms (see Table 1).
Treatment and Follow-up Outcome in Aneurysm-related Hemorrhagic MMD Group
In the aneurysm group (n = 19), endovascular embolization (attempted in 8 patients) was successful in 5 patients (62.5%) (see Fig. 1), with complete obliteration of aneurysms in 3 patients and subtotal occlusion in the other 2. The latter had both disappeared in 1‑month follow-up DSA imaging. One patient suffered re-bleeding of contralateral hemisphere 25.8 months after initial hemorrhage, despite angiographic evidence of embolic obliteration (Fig. 2). Unfortunately, poor clinical status thereafter precluded further angiographic work-up.

Algorithm for treatment of collateral aneurysms in adult hemorrhagic MMD

a Right-sided IVH in computed tomography (CT). b Ruptured aneurysm of collateral artery (digital subtraction angiography). c Completion angiography immediately after transarterial glue embolization (note disappearance of aneurysm). d Left-sided intracerebral and intraventricular hematoma (2-year follow-up CT)
In the three failed attempts at embolization, lesions were technically inaccessible. Endovascular approach was deemed impossible by pretreatment angiography in 11 other patients, whose aneurysms were subsequently managed through conservative measures (see Fig. 1). Surgical exploration conducted in two patients also failed to localize and obliterate the aneurysms involved. In the 14 patients managed conservatively, 13 available follow-up imaging studies (DSA 9 and MRA 4) confirmed the disappearance of 12 aneurysms (92.3%) (Fig. 3). One lesion persisted, remaining unchanged in size and shape on 5‑year follow-up MRA, without re-bleeding. In this subset, 7 patients (50.0%) suffered re-bleeding (follow-up period: mean 69.5 ± 40.8 months, median 73.4 months). Most of the re-bleeding episodes were unrelated to initial aneurysms, based on location and type of repeat hemorrhage (see Table 2). Re-bleeding involved contralateral hemispheres in five patients (see Fig. 2) and different sites of the same hemispheres in the other two. In addition, time to re-bleeding was never <6 months (6–12 months 2, 24–36 months 3 and >60 months 2). The DSA performed after re-bleeding in five patients excluded both initial and new aneurysms as sources of re-bleeding.

a Intraventricular hemorrhage (computed tomography). b Ruptured aneurysm of collateral artery (arrows), confirmed by angiogram of internal carotid artery. c Absence of ruptured aneurysm (1-month follow-up angiogram)
Follow-up Outcome in Aneurysm-unrelated Hemorrhagic MMD Group
All patients of the non-aneurysm group (n = 58, including 1 incidental aneurysm) were managed conservatively, with mean clinical follow-up of 71.9 ± 46.3 months (median, 68.1 months). Within this group, 13 patients suffered episodes of re-bleeding, but follow-up DSAs in 9 patients failed to implicate aneurysms. Most (n = 11) of the repeat hemorrhages involved sites other than those found initially (see Table 2). In terms of timing, most of re-bleeding events (n = 9) occurred >36 months after initial hemorrhages (see Table 2). One incidental aneurysm (contralateral to initial hemorrhage) disappeared, causing no intracranial bleeding during follow-up (Fig. 4).

a Left-sided intraventricular and intracerebral hemorrhage (computed tomography). b Incidental unruptured aneurysm of collateral artery on contralateral side (arrows). c Disappearance of aneurysm (8-day follow-up angiography)
Overall Outcome
A total of 21 patients with hemorrhagic MMD (27.3%) developed re-bleeding during a follow-up period of 453.9 patient-years. Re-bleeding totals over time were as follows: 4 out of 21 (19.0%) within 12 months, 3/21 (14.3%) within 24 months, 3/21 (14.3%) within 36 months and 11/21 (52.4%) after 36 months. The overall re-bleeding rate of hemorrhagic MMD was 4.6% per patient-year. In the aneurysm (vs non-aneurysm) group, the annual re-bleeding rate was higher (7.5%/year; mean, 5.4 years vs. 3.7%/year; mean, 6.0 years); however, most conservatively managed aneurysms disappeared in follow-up imaging studies, as did aneurysms subjected to endovascular embolization; and most of the re-bleeding in patients with aneurysms was unrelated to initial lesions. The annual re-bleeding rate in patients undergoing bypass surgery was lower by comparison (bypass: 4.4%/year; mean, 5.5 ± 3.9 years vs. non-bypass: 4.8%/year; mean, 6.1 ± 3.6 years) (Supplemental Table 3), but cumulative survival rates without re-bleeding did not reach significance for bypass surgery (Kaplan-Meier estimates, p = 0.326).
Discussion
Compared with ischemic MMD, hemorrhagic MMD characteristically runs a more aggressive clinical course, with higher rates of re-bleeding (28–35%) and mortality (7–10%) [5–7]. Thus, evaluation and treatment of bleeding sites is critical to prevent repetitive hemorrhages. Long-standing hemodynamic loads on abnormally dilated collateral vessels and ruptured aneurysms have been implicated in these hemorrhagic events [8, 9]. Kawaguchi et al. [10] suggested that surgical intervention be considered for aneurysms in the circle of Willis region; however, open surgery was not advocated for aneurysms of the basal ganglia or those involving collateral vessels, given the potential for eventual disappearance. Nevertheless, repetitive bleeding can originate from the same or differing sites. Iwama et al. [11] investigated re-bleeding patterns in 15 patients with MMD and hemorrhagic presentations. In their study, seven subjects experienced same site re-bleeding, four with ruptured aneurysms of collateral or major arteries. Most re-bleeding events (6/7, 85.7%) were manifested within 2 months after initial hemorrhages. Repetitive bleeding at different sites was recorded in the other eight subjects, none of whom displayed abnormal vascular lesions or re-bled at intervals >2 months. They concluded that tiny aneurysms persisting after hemorrhage may rupture within short time frames. By comparison, some aspects of our patient series differed from those mentioned. Most ruptured aneurysms (12/13) of collateral arteries that were managed conservatively (due to inaccessibility) disappeared spontaneously, none were associated with re-bleeding, and locations/types of repeat hemorrhages differed from those of initial episodes (see Table 2). In most patients who re-bled, culprit aneurysms linked to initial bleeding events were actually absent on DSAs done after re-bleeding. In terms of timing, all re-bleeding episodes in patients with aneurysms occurred at >6 months after initial hemorrhages.
Although there have been several reports documenting spontaneously disappearing small aneurysms of collateral arteries [10–13], this does not always happen [6, 7, 11]. In our series, most ruptured aneurysms of collateral arteries (92.3%) disappeared within 3 months, with a single lesion persisting for 5 years unchanged (no related re-bleeding). Kim et al. [14] maintain that endovascular occlusion is an effective treatment option for aneurysms of collateral vessels in patients with MMD, and this is our preference if such lesions appear ruptured on discovery by DSA. The bleeding focus is then obliterated, preventing a repeat episode. Endovascular intervention is less invasive and therefore advantageous [14]. In this series, an endovascular approach was attempted in eight patients but succeeded only in five. All five aneurysms were obliterated or disappeared on follow-up DSA, without additional neurological deficits; however, in the other three patients we were unable to advance microdevices to target lesions. In addition, 12 patients were not candidates for this approach due to tortuosity of collateral arteries and the small calibers. Unavoidably, 15 patients were then conservatively managed and monitored. As anatomic outcomes, most inaccessible ruptured aneurysms of collateral arteries disappeared, and related re-bleeding was relatively low in this series. Hence, we believe that conservative treatment is a viable option for ruptured aneurysms of this nature, particularly those that are technically implausible.
Although surgical revascularization has been effective for prevention of ischemic strokes attributable to MMD [15, 16], its efficacy in preventing hemorrhage in this context remains controversial. Miyamoto et al. [9] investigated the efficacy of extracranial-intracranial bypass surgery for preventing hemorrhages in 80 adults with MMD and hemorrhagic presentations. The incidence of recurrent bleeding was 11.9% and 31.6% for surgical and non-surgical treatment, respectively (p = 0.052). Kaplan-Meier analysis also showed a significant decline in cumulative adverse events such as recurrent bleeding, severe disability, or death in surgically (vs. non-surgically) treated patients (2.7%/year vs. 7.6%/year; p = 0.042), indicating that flow bypass would likely reduce the stress on collateral vessels that promotes hemorrhage. In our series, bypass surgery at hemorrhagic sites was performed in 29 patients (aneurysm: 5/19, 26.3%; non-aneurysm: 24/58, 41.4%). The annual re-bleeding rate in patients undergoing bypass surgery was lower by comparison (Supplemental Table 3), but cumulative survival rates without re-bleeding did not reach significance for bypass surgery. In our series, the higher annual re-bleeding rate of the aneurysm group possibly was impacted by a lower frequency of bypass surgery in these patients. Still, this does not explain why the re-bleeding rate in the aneurysm group exceeded that of non-aneurysm group, because aneurysms were not the primary sites of re-bleeding.
Relative to ischemic presentations of MMD, patients with hemorrhagic MMD show more prominent dilatation of AChA and PcomA, with abnormal arterial branching [4, 17]. Morioka et al. [4] investigated angiographic findings contributing to hemorrhage in adult patients with MMD, focusing on AChA, PcomA, and proliferating basal vessels. Dilated AChA (without clear visualization beyond choroidal fissure) and dilated PcomA (with abnormal branching) yielded specificities of 84.4% and 86.4%, respectively, in predicting hemorrhage, whereas basal vascular proliferations did not correlate in this regard. Liu et al. [17] also assessed the association between changes in AChA or PcomA and cerebrovascular lesions of symptomatic hemispheres in adult patients with MMD. Dilated AChA and PcomA, with abnormal branching, showed a relationship with hemorrhage, especially intraventricular hemorrhage. In our series, these phenomena were more commonly observed in the aneurysm (vs. non-aneurysm) group (see Table 1), possibly reflecting increased blood flow to collateral vessels and greater hemodynamic stress [9], thus promoting aneurysm formation/bleeding. Likewise, repetitive bleeding at the same or other sites may be encouraged. Hence, hemodynamic stress may be excessive in patients with hemorrhagic-type MMD who are prone to development of aneurysms.
This particular investigation was focused on aneurysms of collateral arteries suffered by adult patients with MMD and hemorrhagic presentations, analyzing outcomes of a sizeable sampling (77 qualifying lesions) through strict patient monitoring. Although the pathogenesis of heightened re-bleeding in subjects with aneurysms remains unclear, it appears that aneurysms alone do not account for repeat hemorrhages, and observed outcomes are nevertheless valid. However, the potential for selection bias does exist, due to the nonrandomized, retrospective, and observational nature of this study. Other limitations include MRA or CTA use for follow-up assessments of some patients, and inconsistencies in follow-up periods.
Conclusion
In patients with hemorrhagic MMD, treating the aneurysms of collateral vessels is often technically challenging, given the deep locations and structural vulnerabilities. Although ruptured aneurysms are better treated in this setting by endovascular intervention (to prevent re-bleeding), conservative treatment is a viable alternative if technical access is prohibitive. Our data indicate a higher rate of re-bleeding long-term if aneurysms of collateral arteries are accompaniments of hemorrhagic MMD.
References
Amin-Hanjani S, Goodin S, Charbel FT, Alaraj A. Resolution of bilateral moyamoya associated collateral vessel aneurysms: rationale for endovascular versus surgical intervention. Surg Neurol Int. 2014;5(Suppl 4):S155–60.
Harreld JH, Zomorodi AR. Embolization of an unruptured distal lenticulostriate aneurysm associated with moyamoya disease. AJNR Am J Neuroradiol. 2011;32:E42–3.
Kim JE, Kim KM, Kim JG, Kang HS, Bang JS, Son YJ, Han MH, Oh CW. Clinical features of adult moyamoya disease with special reference to the diagnosis. Neurol Med Chir (Tokyo). 2012;52:311–7.
Morioka M, Hamada J, Kawano T, Todaka T, Yano S, Kai Y, Ushio Y. Angiographic dilatation and branch extension of the anterior choroidal and posterior communicating arteries are predictors of hemorrhage in adult moyamoya patients. Stroke. 2003;34:90–5.
Kobayashi E, Saeki N, Oishi H, Hirai S, Yamaura A. Long-term natural history of hemorrhagic moyamoya disease in 42 patients. J Neurosurg. 2000;93:976–80.
Saeki N, Nakazaki S, Kubota M, Yamaura A, Hoshi S, Sunada S, Sunami K. Hemorrhagic type moyamoya disease. Clin Neurol Neurosurg. 1997;99(Suppl 2):S196–S201.
Yoshida Y, Yoshimoto T, Shirane R, Sakurai Y. Clinical course, surgical management, and long-term outcome of moyamoya patients with rebleeding after an episode of intracerebral hemorrhage: an extensive follow-Up study. Stroke. 1999;30:2272–6.
Kuroda S, Houkin K. Moyamoya disease: current concepts and future perspectives. Lancet Neurol. 2008;7:1056–66.
Miyamoto S, Yoshimoto T, Hashimoto N, Okada Y, Tsuji I, Tominaga T, Nakagawara J, Takahashi JC; JAM Trial Investigators. Effects of extracranial-intracranial bypass for patients with hemorrhagic moyamoya disease: results of the Japan Adult Moyamoya Trial. Stroke. 2014;45:1415–21.
Kawaguchi S, Sakaki T, Morimoto T, Kakizaki T, Kamada K. Characteristics of intracranial aneurysms associated with moyamoya disease. A review of 111 cases. Acta Neurochir (Wien). 1996;138:1287–94.
Iwama T, Morimoto M, Hashimoto N, Goto Y, Todaka T, Sawada M. Mechanism of intracranial rebleeding in moyamoya disease. Clin Neurol Neurosurg. 1997;99(Suppl 2):S187–90.
Hamada J, Hashimoto N, Tsukahara T. Moyamoya disease with repeated intraventricular hemorrhage due to aneurysm rupture. Report of two cases. J Neurosurg. 1994;80:328–31.
Kwak R, Ito S, Yamamoto N, Kadoya S. Significance of intracranial aneurysms associated with moyamoya disease. (Part I). Differences between intracranial aneurysms associated with moyamoya disease and usual saccular aneurysms – review of the literature. Neurol Med Chir (Tokyo). 1984;24:97–103.
Kim SH, Kwon OK, Jung CK, Kang HS, Oh CW, Han MH, Kim YS, Baik SK. Endovascular treatment of ruptured aneurysms or pseudoaneurysms on the collateral vessels in patients with moyamoya disease. Neurosurgery. 2009;65:1000–4.
Takahashi JC, Miyamoto S. Moyamoya disease: recent progress and outlook. Neurol Med Chir (Tokyo). 2010;50:824–32.
Liu X, Zhang D, Shuo W, Zhao Y, Wang R, Zhao J. Long term outcome after conservative and surgical treatment of haemorrhagic moyamoya disease. J Neurol Neurosurg Psychiatry. 2013;84:258–65.
Liu W, Zhu S, Wang X, Yue X, Zhou Z, Wang H, et al. Evaluation of angiographic changes of the anterior choroidal and posterior communicating arteries for predicting cerebrovascular lesions in adult moyamoya disease. J Clin Neurosci. 2011;18:374–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
R. Jong Kook, C. Young Dae, J. Jin Pyeong, Y. Dong Hyun, C. Won-Sang, K. Hyun-Seung, K. Jeong Eun and H. Moon Hee declare that they have no competing interests.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Caption Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
Rhim, J.K., Cho, Y., Jeon, J.P. et al. Ruptured Aneurysms of Collateral Vessels in Adult Onset Moyamoya Disease with Hemorrhagic Presentation. Clin Neuroradiol 28, 191–199 (2018). https://doi.org/10.1007/s00062-016-0554-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00062-016-0554-8