
Abstract
Purpose
This study evaluated morphological features of developmental venous anomalies (DVAs) based on magnetic resonance imaging (MRI) findings. The study also evaluated the factors affecting the visibility of DVAs on MRI.
Methods
We reviewed contrast-enhanced MRIs of 75 patients with DVA. The images were selected from 1,165 consecutive cranial MRIs. The images were examined for the DVA location, the number of collecting veins, the collecting vein diameter, drainage veins and sinuses, any accompanying parenchymal abnormalities or lesions, and the DVA visibility on MRI.
Results
DVAs prevalence was determined as 6.4 %. A total of 88 DVAs were observed. Single DVAs were observed in 65 patients, two were observed in 7 patients and three were observed in 3 patients. The DVA caputs had deep localization most frequently in 54.5 % of patients. A total of 98 collecting veins were identified, with a single vein identified in 80 DVAs. A statistically significant difference (p = 0.000) was found in the diameter of the collecting veins between DVAs that were the visible and nonvisible on noncontrast MRI.
Conclusions
Most frequently, a single DVA was observed in the patients. A DVA caput could be located in the deep, subcortical, juxtacortical or deep + subcortical and juxtacortical + subcortical regions. Increasing collecting vein diameter increased visibility on noncontrast MRI, and small DVAs could be overlooked, even with contrast-enhanced MRI series if the images were not examined carefully.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Cerebral vascular malformations are categorized as arteriovenous malformations, capillary telangiectasias, cavernous malformations (CM), and developmental venous anomalies (DVAs) [1, 2]. The most frequently encountered cerebral vascular malformations are DVAs, with an incidence of 2.58 % in a series of 4,069 brain autopsies [3].
As suggested by Lasjaunias et al. [4], the term developmental venous anomaly is now widely used as a synonym of venous angioma or cerebral venous malformation [2]. DVAs can serve as the normal drainage routes of brain tissue [5]. The typical caput medusae draining into a collecting vein can be observed in both computed tomography (CT) and magnetic resonance imaging (MRI), allowing for the confident diagnosis of DVAs [2]. The diagnosis of a DVA has often generated concern among many physicians who are less familiar with the field of intracranial vascular malformations, although most DVAs have been discovered incidentally and have shown no clinical significance [2, 5].
In this study, we have evaluated the factors that affect the visibility of DVAs in MRI and the morphological features of DVAs based on MRI findings.
Methods
In this study, after obtaining the approval of local ethics committee (number: 13-KAEK-039), we retrospectively analyzed the contrast-enhanced cranial MRIs in the PACS system (GE Healthcare, Milwaukee, WI, USA) of 1,165 patients. The imaging had been conducted for several reasons from September 2009 to January 2013. A total of 75 patients, including 45 females and 30 males, diagnosed with DVAs were included in the study. The MRI examinations were performed on a 1.5 T (Signa excite HD; GE Healthcare, Milwaukee, WI, USA, 2005) machine, using an eight channel neurovascular coil. Contrast-enhanced cranial MRI examinations obtained spin echo T1-weighted or 3D spoiled gradient recalled echo (3D SPGR) sequences. The spin echo T1 sequence parameters were TR/TE, 600/16 ms; matrix 320 × 224; field of view, 25 cm; slice thickness, 5 mm; slice spacing, 1 mm. The 3D SPGR sequence parameters were TR/TE, 6.88/2.48 ms; matrix, 288 × 160; field of view, 22 cm; slice thickness, 4 mm; slice spacing, 2 mm. We performed 3D SPGR examinations in 57 patients, spin echo T1-weighted examinations in 10 patients and both 3D SPGR and spin echo T1 weighted contrast-enhanced brain MRI examinations in 8 patients. We used 0.1 mmol/kg gadopentetate or gadobenatedimeglumine as contrast agents. Images in the PACS system were diagnosed as DVA with consensus after being evaluated by two radiologists (E.G., M.B.).
Vascular structures passing cerebral or cerebellar parenchyma in different lengths and that are characterized by the clustering of venous stems uniting in a collecting vein that causes the typical medusa head appearance have been accepted as DVAs (Fig. 1). There have been studies regarding the prevalence of DVAs, the locations of DVAs (infra-supratentorial, cerebral-cerebellar hemispheres and brain stem formations, and cerebral lobes), the parenchymal areas where DVA caputs are distributed and drained (deep, subcortical, juxtacortical, deep + subcortical, and juxtacortical + subcortical), collecting vein numbers and diameters, drained veins or sinuses, accompanying parenchymal abnormalities (i.e., gliosis) and lesions (i.e., CM, cyst, mass).

A developmental venous anomaly (DVA) accompanied by a small cyst and loco-regional atrophy localized in the left frontal deep + subcortical white matter of a 45-year-old woman with headache complaints. a Thin venous stems and veins in the center, leading to the caput medusae imaging on axial contrast-enhanced 3D spoiled gradient recalled echo (3D SPGR) maximum intensity projection image are visualized. b Loco-regional atrophy in the frontal lobe and a millimetric cyst adjacent to the DVA caput on a coronal contrast-enhanced 3D SPGR image is visualized
The subcortical area has been defined as the area below the juxtacortical region that is not adjacent to the ventricular wall. The deep (or para-periventricular) has been defined as the area adjacent to the lateral, third, or fourth ventricle and the basal ganglia, brachium pontis, dentate nucleus, or the area within the center of the structure, such as the pons (Fig. 2). The location of DVAs has been categorized as deep + subcortical (Fig. 3) and juxtacortical + subcortical (Fig. 4) in cases for which DVA caputs have extended to both deep and subcortical regions or to both juxtacortical and subcortical regions. The collecting vein joined by the caput medusae has been classified as either deep or superficial draining vein. In the supratentorial compartment, superficial collecting veins are identified as those that are joined to the superior sagittal sinus or to other superior sinuses. Deep collecting veins are identified as those that join to the subependymal veins of the lateral ventricles, basal veins of Rosenthal, internal cerebral veins, and the vein of Galen (Fig. 2d). In the infratentorial compartment, superficial collecting veins have been identified as those that join to the transverse or sigmoid sinus and torcula. Deep collecting veins are those that join to the subependymal veins of the fourth ventricle or the deep venous sinuses (petrosal sinus and cavernous sinus) or the internal jugular veins (Fig. 2b). The diameters of the collecting veins have been determined by taking the average of measurements that have been performed in at least two planes from the region where the vein is widest.

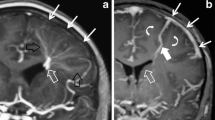
A 37-year-old man with three developmental venous anomalies (DVAs), right-sided hemiparesis, and right central facial paralysis. Only a large infratentorial DVA was in the patient’s radiology report, but supratentorial small DVAs were determined on retrospective evaluation. a A large DVA (white arrows) with double collecting veins distributed to both dentate nuclei, the brachium pontis and the pons. The image is more intense on the right on the axial contrast-enhanced 3D spoiled gradient recalled echo (3D SPGR) MIP image. Left occipital sinus (thin black arrow). b The double collecting veins (white arrows) drained to the superior petrosal sinus (black arrow) at the right cisternal distance on a coronal contrast-enhanced 3D SPGR image. c A second DVA that had one collecting vein (black arrow) caput (white arrow), which was located in the right basal ganglion on an axial contrast-enhanced 3D SPGR image. d A small third DVA located in the parietal deep white matter. The caput (white arrow) has been drained from the collecting vein to the subependymal vein on the axial contrast-enhanced 3D SPGR MIP image

A developmental venous anomaly (DVA) located in the deep + subcortical region in the right frontal lobe of a 40-year-old woman with headache complaints. Collecting veins that have been extended to both caudate nucleus and the periventricular region (white arrows) and the superior frontal and cingulate gyrus subcortical regions (black arrows) in the DVA caput on a and b axial plane, c and d coronal-enhanced spin echo T1-weighted magnetic resonance imaging

A small developmental venous anomaly (DVA) localized in the left parietal lobe juxtacortical + subcortical regions in a 61-year-old woman with a headache. a Juxtacortical extension of the DVA caput on an enhanced axial contrast-enhanced 3D spoiled gradient recalled echo (3D SPGR) sequence (black arrow). b Subcortical extension of the DVA caput on enhanced coronal contrast-enhanced 3D SPGR image (white arrow). c Subcortical extension of the DVA caput on a sagittal-enhanced spin echo T1-weighted image (white arrow). d Juxtacortical extension of a DVA caput on a sagittal contrast-enhanced spin echo T1-weighted image (black arrow)
There have been studies concerning the relationship between accompanying parenchymal abnormalities or lesions and the collecting vein diameters with a prevalence and visibility of DVAs in a noncontrast MRI series. The relationship between the collecting vein diameters and the accompanying parenchymal abnormality or lesion and the localization of the DVA caputs diagnosed with parenchymal abnormality or lesion has also been examined.
Statistical Analysis
The data have been presented as the mean ± standard deviation, median (minimum–maximum), and percentage. Student’s t test has been performed for comparisons in two independent groups. The level of significance has been accepted as p < 0.05.
Results
The age of the participants in the study ranged from 4 to 84 (mean 45.52 ± 17.12). The prevalence of DVAs has been determined to be 6.4 %. In total, 88 DVAs were observed. A single DVA was observed in 65 patients, two DVAs were observed in 7 patients and three DVAs were observed in 3 patients. Sixty-four (72.7 %) of the DVAs were located in the supratentorial region, and 24 (27.3 %) were located in the infratentorial region. Forty-eight (54.5 %) of the DVAs were located in the right cerebellar or cerebral hemisphere, while 37 (42.0 %) were in the left cerebellar or cerebral hemisphere, one (1.1 %) was in both cerebellar hemispheres, and two (2.3 %) were found in the midline of the pons. The most frequent location of the DVAs has been frontal lobes. In Table 1, we have shown intracranial localizations and frequencies of DVAs. In terms of localization of DVA caputs, 54.5 % were deep (Table 2).
While there was one collecting vein in 80 (90.9 %) of 88 DVAs, it was determined that there were 98 total collecting veins, including 2 collecting veins in 6 DVAs (6.8 %), and 3 in 2 DVAs (2.3 %) (Figs. 2 and 5). Collecting vein diameters ranged from a minimum of 1.0 mm to a maximum of 4.3 mm (median 2.0 mm). In DVAs that have multiple collecting veins, the collecting vein diameters ranged between 1.2–4.3 mm (mean 2.39 ± 0.91 mm). Six of the DVAs that have multiple collecting veins were in the supratentorial region, and two were localized in the infratentorial region. Forty-nine of the collecting veins (50.0 %) drained to the deep venous system and the other 49 (50.0 %) drained to the superficial venous system. Six DVAs were shown to have both superficial and deep drainage to the venous system, five of which were located in the supratentorial region and one that was located in the infratentorial region and had more than one collecting vein (Fig. 5). In Table 3, we present the drainage frequencies of DVA caputs to the superficial and deep venous systems, according to the locations of the DVAs. In addition, we present the numbers and frequencies of the veins or dural venous sinuses to which veins are drained in Table 4.

Heterogeneous intensity lesion in the left frontal lobe of a 51-year-old man with epilepsy (Glial mass? + gross gliosis?). The developmental venous anomaly (DVA) could not be visualized on a axial T2 weighted image or b coronal flair image. A deeply localized DVA drained to the internal cerebral vein and superior sagittal sinus, passing through the lesion on c sagittal and d axial contrast-enhanced spin echo T1-weighted images
When parenchymal abnormalities and the number of lesions accompanying DVAs were analyzed, there were abnormalities in the parenchyma adjacent to the DVA and lesions, such as cavernomas in 25 (28.4 %) patients (Figs. 1 and 5). Table 5 presents the parenchymal abnormalities and lesions accompanying DVAs and the frequencies of these lesions. When the locations of the DVA caputs, accompanied by a parenchymal abnormality or a lesion were analyzed, 11 were deep, 7 were deep + subcortical, 3 were subcortical, 3 were juxtacortical, and 1 was juxtacortical + subcortical. There were cavernomas in 13 (17.3 %) of the patients with DVAs, and the number of cavernomas accompanying DVAs was 11 (12.5 %). Those 11 cavernomas were located within or near the DVA caput (the DVA drainage region). DVAs of these cases were located in the infratentorial region while cavernomas in other two patients were intracerebral. There were acute or subacute hemorrhages in eight of the cavernomas accompanying the DVAs. Of the patients diagnosed with hemorrhagic cavernoma, seven had a severe headache, and one had status epilepticus. There was no statistically significant difference (p > 0.05) between parenchymal abnormality or lesion and collecting vein diameters.
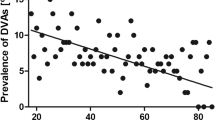
In the noncontrast brain MRI series, 48 (54.5 %) of DVAs were visible and 40 (45.5 %) could not be observed. The average size of the collecting vein diameters for the visible DVAs was 2.37 ± 0.68 mm, and the average size for the nonvisible DVAs was 1.71 ± 0.48 mm. The difference between the two averages was statistically significant (p = 0.000). The number of DVAs on retrospective analysis that were not reported in contrast-enhanced primary MRIs but were reported in subsequent MRIs was 18 (20,4 %), and their collecting vein diameters (the number of collecting veins was 23, including three veins each in two DVAs, two veins in one DVA) were between 1 and 2.3 mm (mean 1.57 ± 0.34). Only four of the DVAs could be visualized on retrospective evaluations in the noncontrast MRI series. The DVAs were not mentioned in reports of spin echo in five of eight patients in whom contrast-enhanced MRI examination were conducted with both 3D SPGR sequence and spin echo, those DVAs were reported in examinations conducted with 3D SPGR. While the DVA could not be observed because of intense pulsation artifacts in the enhanced series obtained with the spin echo sequence on the first MRI of the patient with the infratentorially located DVA, the DVA could be observed on contrast-enhanced MRI conducted with 3D SPGR during follow-up.
No statistically significant difference (p > 0.05) between the visibility of the DVAs in a noncontrast series and the accompanying parenchymal abnormality and lesion has been determined. Of 11, 6 DVAs accompanied by cavernomas could be observed in the noncontrast series (p > 0.05).
Discussion
Lasjaunias et al. [4] proposed that DVAs result from a hemodynamic need that causes the recruitment of transhemispheric anastomotic pathways, and therefore DVAs must be viewed as an anatomical variation [1]. Although there have been different views regarding the development of DVAs, there is a common belief that DVAs develop as result of fetal angiogenesis and deficiencies in regression [1, 2, 4, 6]. DVAs are characterized by a cluster of venous radicles that converge into a collecting vein, resulting in the typical caput medusae or umbrella-like appearance of the DVA [1, 7]. To join either the superficial or deep venous system, the collecting vein crosses a variable length of cerebral or cerebellar parenchyma [1, 7]. DVAs may occasionally drain into both the superficial and deep venous systems, and one of those drainage pathways is predominant [1]. In the study performed by Lee et al. [7], there were 73 DVAs identified in 61 patients. Of these, 5 (6.9 %) DVAs were reported to drain to both the superficial and deep venous systems. In our study only 6.8 % of DVAs were found to drain to both the superficial or deep venous systems.
DVAs have primarily been considered the rarest of the vascular malformations [7]. With the progresses of CT scanning and, more recently MRI, DVAs have been identified as the most common malformations of the cerebral vasculature [7]. In a study by Lee et al. [7], brain MRIs of 4,624 patients obtained with a contrast-enhanced spin echo T1 series found DVAs in 61 (1.3 %) patients. A similar study by Lee and Kim [5] found DVAs in 31 (1.63 %) of 1,899 patients. In our study, the frequency of DVAs found on contrast-enhanced cranial MRI was 6.4 %, which was higher than the frequency determined in the literature. We consider that contrast-enhanced MRI series obtained with 3D SPGR sequence contributes to this higher frequency. There were no reported DVAs on spin echo in five of eight patients in whom MRI examination was conducted with both spin echo and 3D SPGR sequence methods, but the DVAs were reported in examinations obtained with 3D SPGR. In one of those patients, an intense pulsation artifact of the dural venous sinuses formed in the posterior fossa, which prevented the DVA and the cavernoma from being observed in the spin echo series. In our study, nearly half of the DVAs (45.5 %) could not be visualized on routine brain MRI unenhanced series, and we found a statistically significant difference (p = 0.000) between the visibility of DVAs and the collecting vein diameter. While DVAs that have an average 2.3 mm collecting vein diameter could be observed in an unenhanced series, DVAs with an average 1.7 mm diameter were not visible. For this reason, it is necessary to perform contrast-enhanced cranial MRI to visualize DVAs. However, small DVAs that have a small collecting vein diameter can be overlooked, even in a contrast-enhanced series if it is not analyzed carefully. In our study, the frequency of DVAs that are not reported in a contrast-enhanced MRI series was 20.4 %, and those were small DVAs with 2.3 mm or smaller collecting vein diameters. Parenchymal abnormalities or lesions accompanying the DVA have not aided in the visibility of the DVA on a noncontrast imaging series. Similarly, the visibility of the DVAs accompanied by a cavernoma in a noncontrast series was not statistically significant. However, we consider that contrast-enhanced MRI should be conducted to visualize accompanying DVAs in patients diagnosed with cavernoma on imaging methods because of the frequency of the association between DVA and cavernoma.
DVAs are frequently located in the supratentorium, with a clear frontal predominance [1]. Huang et al. [8] noted in his study, including surgical cases and digital subtraction angiography (DSA) data, that DVAs were frequently been found in the frontal and parietal lobe (40 %) and the cerebellum (27 %), and were less often found in the parietal and parieto-occipital lobe (15 %), the basal ganglia and thalamus (11 %), the temporal lobe (3 %), the brain stem (2 %), and in intraventricular locations (2 %). In a study by Garner et al. [9] of 100 patients with DVA determined by DSA, CT, and MRI examinations, DVAs are largest in the frontal (42 %), parietal (24 %), cerebellar (14 %), basal or ventricular (11 %), occipital (4 %), brain stem (3 %), and temporal (2 %) locations. Lee et al. [7] determined the locations of 72 DVAs, and found 6 % of DVAs to be frontal, 22 % cerebellar, 22 % parietal, 10 % temporal, 4 % occipital and basal ganglia, and 2 % pons. In their study of 29 DVAs in 28 patients, Wilms et al. [10] found the locations of DVAs prevalence to be the frontal region (38 %), the cerebellar region, (38 %), the parietal region (10 %), the occipital region (10 %), and the temporal region (7 %). In the study of Lee and Kim [5], DVAs are most frequently localized to the frontal lobes (60 %). Similar to previous articles, our study found DVAs localized most frequently to the frontal lobes (40.9 %), with the dentate nucleus 19.9 % as the second most frequent location.
DVAs can be located superficially, juxtacortically, or subcortically and deeply (or paraventricularly). This categorization was first suggested by Valavanis et al. [11]. In a study by Valavanis et al. [11] of seven patients, DVA caputs were localized in the subcortical region in four patients, the juxtacortical region in two patients and the para-ventricular region in one patient. In study by Ostertun et al. [12], 13 of 21 DVAs found in 20 patients had caputs localized in the subcortical region, and eight caputs were located in the deep regions. In a study by Lee et al. [7] regarding 72 DVAs, the deep location was the most common site (41 caputs), with the juxtacortical (18 caputs) and the subcortical (13 caputs) locations being far less common. In our study, 48 (54.4 %) of DVA caputs were deep, 15 (17 %) were subcortical and 5 (5.7 %) were juxtacortical. In contrast to previous studies, we found 15 (17 %) DVAs in which the caputs were distributed to both deep and subcortical regions, and 5 (5.7 %) DVAs in which the caputs were distributed to both juxtacortical and subcortical regions. For this reason, we added deep + subcortical and juxtacortical + subcortical groups into the categories for the localization of DVA caputs.
Many collectors can be observed in nearly 6–8.3 % of DVAs, although the collecting vein is typically unique, and it has previously been reported in the literature that 5.9–8.3 % of DVAs include multiple collecting veins [7, 13]. In our study, multiple collecting veins were found in 9.1 % of DVAs, which is consistent with previous studies. In a study by Ruiz et al. [13], although multiple collecting veins have been reported in the posterior fossa and in large DVAs, the majority of DVAs with multiple collecting veins in our study were located in the supratentorial region and were of various sizes. Two or more DVAs that existed in separate regions of the brain simultaneously have been observed in 1.2–16.3 % of cases [5, 7, 13, 14]. In our study, the prevalence of more than one DVA was 13.3 %, which is in accordance with the literature. Lee et al. [7] found that 1.6 % of patients had three DVAs, but we found that 4.0 % (three patients) had three DVAs.
Before the advances were made in CT and MRI, DVAs were considered to be rare entities, which often resulted in cerebral hemorrhages and seizures [1]. They were often associated with one or more regional CMs in 3.2–40 % of cases [5, 13, 15–17]. In our study, we found CM in 17.3 % (if the DVA is not localized in the drainage region, it is only 11 %) of patients with DVA. The CMs are now considered responsible for the majority of symptomatic cases were previously attributed to the DVAs [1]. We showed the presence of cavernomas with hemorrhage in an acute or subacute process accompanying DVAs in eight symptomatic patients in our study. Various parenchymal abnormalities and lesions other than cavernomas can accompany DVAs. Santucci et al. [16] found accompanying parenchymal abnormalities or lesions in 28 (16 %) of 174 DVAs. The frequency of parenchymal abnormalities and lesions accompanying 84 DVAs studied by Ruiz et al. [13] in 83 patients was 65.4 %. Ruiz found the most frequently determined abnormality was locoregional atrophy, which occurred in 29.7 %. In our study, we found accompanying parenchymal abnormalities or lesions in 25 DVAs (28.4 %), and the most frequently encountered lesion was a cavernoma, which occurred in 44 % of the cases. Isolated locoregional atrophy was observed in one (4 %) patient, and gliosis or a cyst was accompanied by locoregional atrophy in one patient each. The discrepancy in parenchymal abnormalities and the lesions associated with DVAs is unclear, but it may be related to selection bias and sample size. In a study by Santucci et al. [16], when the relationship between the accompanying parenchymal abnormality or lesions and the localization of the DVA caput, the parenchymal signal intensity changes were generally in deep localized DVAs. Our study also determined that parenchymal abnormalities or lesions correlated frequently with deeply located DVAs (Fig. 4). Similar to the results of Santucci et al. [16], we did not find a statistically significant difference between parenchymal abnormalities and collecting vein diameters.
It has been reported that along with the developments in MRI area, susceptibility-weighted imaging (SWI), an increasingly used imaging system in recent years with a maximized sensitivity effect, can better display vascular deformations such as slow venous flow DVA, CM, and telangiectasia [18]. SWI can demonstrate the whole structure well and has been shown to be more sensitive than conventional T2* imaging in the detection of venous structures [18]. The sensitivity of SWI in assessing the number of CM lesions accurately is significantly higher than that of T2-weighted fast spin echo and gradient echo sequences [18, 19]. In addition, it has also been reported that SWI obtained through high and ultra-high strength (3 and 7 T) imaging can better visualize CMs and accompanying DVAs [20].
It is generally accepted that when DVAs exhibit characteristic CT and MRI findings, angiography is not required for their confirmation. However, in patients exhibiting DVAs associated with atypical hemorrhagic lesions, cerebral angiography is mandatory to determine the true cause of bleeding [21]. DVA with a vascular malformation, arteriovenous shunting, and an arterialized DVA have been described as early appearing vessels with a capillary blush in the arterial phase and early venous filling on DSA [22]. Besides, DSA reveals the typical caput medusae aspect of the draining vein in the territory affected by hemorrhage with signs of venous outflow obstruction such as prolonged transition, venous stasis, and a missing central venous collector as a sign for thrombosis of the latter [23].
Studies have reported associations between DVAs and choreoballismus [24], obstructive hydrocephalus of the cerebral aqueduct by the DVA [25], ophthalmoplegic migraine [26], tinnitus [27], unilateral sensorineural hearing loss [28], and nerve root compression [29]. In our study, one patient had central facial nerve palsy and a cerebellopontine large DVA (Fig. 2).
Conclusions
DVAs have been most often observed in the frontal lobes and can be encountered in both the supra and infratentorial parenchyma regions. A DVA can have one collecting vein, but more often has two or multiple collecting veins. The DVA caput can be localized in deep, subcortical, juxtacortical, deep + subcortical, or juxtacortical + subcortical regions. A larger diameter of the collecting vein increases the visibility of the DVA on a noncontrast MRI series, and small DVAs can be overlooked even on contrast-enhanced MRI series that are not examined carefully.
References
Ruiz DS, Yιlmaz H, Gailloud P. Cerebral developmental venous anomalies: current concepts. Ann Neurol. 2009;66:271–83.
Ruiz DS, Gailloud P. Cerebral developmental venous anomalies. Child Nerv Syst. 2010;26:1395–406.
Sarwar M, McCormick WF. Intracerebral venous anjioma. Case report and review. Arch Neurol. 1978;35:323–5.
Lasjaunias P, Burrows P, Planet C. Developmental venous anomalies (DVA): the so-called venous anjioma. Neurosurg Rev. 1986;9:233–42.
Lee M, Kim MS. Image findings in brain developmental venous anomalies. J Cerebrovasc Endovasc Neurosurg. 2012;14:37–43.
Saito Y, Kobayashi N. Cerebral venous angiomas: clinical evaluation and possible etiology. Radiology. 1981;139:87–94.
Lee C, Pennington MA, Kenney CM 3rd. MR evaluation of developmental venous anomalies: medullary venous anatomy of venous angiomas. AJNR Am J Neuroradiol. 1996;17:61–70.
Huang YP, Patel SC, Robbins A, Chaudhary M. Cerebral venous malformation and a new classification of cerebral vascular malformations. In: Kapp JP, Schmidek HH, editors. The cerebral venous system and its disorders. Orlando:Grune & Stratton; 1984. pp 373–474.
Garner TB, Curling OD, Kelly DL, Laster DW. The natural history of intracranial venous angiomas. J Neurosurg. 1991;75:715–22.
Wilms G, Demaerel P, Marchal G, Baert AL, Plets C. Gadolinium enhanced MR imaging of cerebral venous angiomas with emphasis on their drainage. J Comput Assist Tomogr. 1991;15:199–206.
Valavanis A, Wellauer J, Yasargil MG. The radiological diagnosis of cerebral venous angioma: cerebral angiography and computed tomography. Neuroradiology. 1983;24:193–99.
Ostertun B, Solymosi L. Magnetic resonance angiography of cerebral developmental venous anomalies: its role in differential diagnosis. Neuroradiology. 1993;35:97–104.
Ruiz DS, Delavelle J, Yιlmaz H, Gailloud P, Piovan E, Bertramello A, et al. Parenchymal abnormalities associated with developmental venous anomalies. Neuroradiology. 2007;49:987–95.
Uchino A, Hasuo K, Matsumoto S, Masuda K. Double cerebral venous angiomas: MRI. Neuroradiology. 1995;37:25–8.
Huber G, Henkes H, Hermes M, Felber S, Terstegge K, Piepgras U. Regional association of developmental venous anomalies with angiographically occult vascular malformations. Eur Radiol. 1995;6:30–7.
Santucci GM, Leach JL, Ying J, Leach SD, Tomsick TA. Brain parenchymal signal abnormalities associated with developmental venous anomalies: detailed MR imaging assessment. AJNR Am J Neuroradiol. 2008;29:1317–23.
Abe T, Singer RJ, Marks MP, Norbash AM, Crowley RS, Steinberg GK. Coexistence of occult vascular malformations and developmental venous anomalies in the central nervous system: MR evaluation. AJNR Am J Neuroradiol. 1998;19:51–7.
Tsui YK, Tsai FY, Hasso AN, Greensite F, Nguyen BV. Susceptibility-weighted imaging for differential diagnosis of cerebral vascular pathology: a pictorial review. J Neurol Sci. 2009;287:7–16.
de Souza JM, Domingues RC, Cruz LC Jr., Domingues FS, Iasbeck T, Gasparetto EL. Susceptibility-weighted imaging for the evaluation of patients with familial cerebral cavernous malformations: a comparison with T2-weighted fast spin-echo and gradient-echo sequences. AJNR Am J Neuroradiol. 2008;29:154–8.
Dammann P, Barth M, Zhu Y, Maderwald S, Schlamann M, Ladd ME, et al. Susceptibility-weighted magnetic resonance imaging of cerebral cavernous malformations: prospects, drawbacks, and first experience at ultra-high field strength (7-Tesla) magnetic resonance imaging. Neurosurg Focus. 2010;29(3):E5.
Oran I, Kiroglu Y, Yurt A, Ozer FD, Acar F, Dalbasti T, et al. Developmental venous anomaly (DVA) with arterial component: a rare cause of intracranial hemorrhage. Neuroradiology. 2009;51:25–32.
Hanson EH, Roach CJ, Ringdahl EN, Wynn BL, DeChancie SM, Mann ND, et al. Developmental venous anomalies: appearance on whole-brain CT digital subtraction angiography and CT perfusion. Neuroradiology. 2011;53:331–41.
Dorn F, Brinker G, Blau T, Kabbasch C, Reiner M, Liebig T. Spontaneous thrombosis of a DVA with subsequent intracranial hemorrhage. Clin Neuroradiol. 2012; doi:10.1007/s00062-012-0190-x
Burke L, Berenberg RA, Kim KS. Choreoballismus: a nonhemorrhagic complication of venous angiomas. Surg Neurol. 1984;21:245–8.
Yagmurlu B, Fitoz S, Atasoy C, Erden I, Deda G, Unal O. An unusual cause of hydrocephalus: aqueductal developmental venous anomaly. Eur Radiol. 2005;15:1159–62.
Berbel-Garcia A, Martinez-Salio A, Porta-Etessam J, Saiz-Diaz R, Gonzalez-León P, Ramos A, et al. Venous angioma associated with atypical ophthalmoplegic migraine. Headache. 2004;44:440–2.
Malinvaud D, Lecanu JB, Halimi P, Avan P, Bonfils P. Tinnitus and cerebellar developmental venous anomaly. Arch Otolaryngol Head Neck Surg. 2006;132:550–3.
Ferreira D, Mendes V, Vide A, Costa JD. Developmental venous anomaly of the internal auditory canal in a child with unilateral sensorineural hearing loss—a rare association. Pediatr Radiol. 2012;42:1021–3.
Peterson AM, Williams RL, Fukui MB, Meltzer CC. Venous angioma adjacent to the root entry zone of the trigeminal nerve: implications for management of trigeminal neuralgia. Neuroradiology. 2002;44:342–6.
Conflict of Interest
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gökçe, E., Acu, B., Beyhan, M. et al. Magnetic Resonance Imaging Findings of Developmental Venous Anomalies. Clin Neuroradiol 24, 135–143 (2014). https://doi.org/10.1007/s00062-013-0235-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00062-013-0235-9