
Abstract
Objectives
This study aimed to identify which are the socio-demographic factors that can describe health information users’ profiles in Europe and assess which are the factors distinguishing users and non-users and their association with the use of health-related online information.
Methods
Data from the Flash Eurobarometer No. 404 (2014) was analysed through a multilevel logistic regression model and a propensity score matching.
Results
There were significant differences in the use of the Internet for health information according to gender, age, education, long-term illness and health-related knowledge. Thus, some digital divides persisted in the use of health information online. Results showed that a poor health status was associated with a higher use of the Internet for health purposes only for people having chronic conditions.
Conclusions
Findings show a need to increase people’s eHealth literacy, especially for males over 45 years old not suffering from a long-term illness. In order to limit the misuse of poor or untrustworthy health information that might contribute to higher health disparities, special interest should be focused on population socio-demographic characteristics.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Information and communications technologies (ICTs) have become widely available to the European population, in terms of both accessibility and cost (Eurostat 2018). In the 28 country members of the European Union (EU-28), households with Internet access rose to 87% in the year 2017, approximately 32 percentage points higher than in 2007. The increase in ICT accessibility has especially impacted on the EU-28 population aged between 16 and 74 years. A 85% of this age group reported the use of any ICT tool at least once within the previous 3 months (Eurostat 2018). ICTs are changing the way we acquire and share knowledge, including about health and illnesses. Hence, the Internet is increasingly becoming the first source of information, especially with regard to diseases (Hesse et al. 2010). The Flash Eurobarometer No. 404, which was carried out in the EU-28 in 2014 to investigate how the Internet is used to manage health, showed that 75% of European citizens considered the Internet as a good tool for finding health information (TNS Political and Social 2014). However, recent studies have demonstrated that 40–50% of web pages related to common diseases contained misinformation (Bratu 2018; Waszak et al. 2018; Allcott et al. 2019). Furthermore, social media are largely contributing to diffuse fake news on many health topics (Chou et al. 2018). Since 2015, the European Commission is working to implement a clear, comprehensive and broad set of actions to tackle the spread and impact of online misinformation in Europe, thus protecting EU citizens’ health (European Commission 2019).
The use of ICT, and in particular the Internet, presents both great opportunities and dangers in terms of information seeking that can affect population health. Every day, anybody can find online a great amount of health-related information concerning health habits, social determinants of health, specific diseases and risk factors. Only a fraction of the information is evidence-based (Norman and Skinner 2006). Furthermore, it is possible to compare retrieved information across multiple online sources whose trustworthiness is variable: health forums, institutional websites, generic health-related websites, blogs, e-mailing and chatting with health experts or services, and social media (Coulter et al. 2006; Stevenson et al. 2007; Tonsaker et al. 2014; McMullan 2016). The Internet has actually become very important for people willing to obtain quick and free health-related information, in order to take healthcare decisions for themselves or for their family, or simply out of curiosity (Devine et al. 2016). There is a great availability of public data on opinions, attitudes and behaviours which is continuously generated online. On the one hand, this data can be useful for promoting healthy conducts and preventing risky behaviours. On the other hand, knowledge derived from poor and misleading data can cause harm by letting people think that they have acquired medical skills and self-efficacy for fulfilling treatment goals and improving adherence based on advice found online (Iverson et al. 2008). In fact, the autonomous online search of health information can lead to medically inaccurate beliefs and risky health behaviour (Vance et al. 2009) Therefore, the access and use of quality online information have become a major public health priority (WHO 2014).
The concept of eHealth literacy has been described as the ‘ability to seek, find, understand and appraise health information from electronic sources and apply knowledge gained to addressing or solving a health problem’ (Norman and Skinner 2006). The four dimensions of eHealth literacy (‘seek’, ‘find’, ‘understand’ and ‘appraise’) are all essential for empowering users to better manage their health, improve health control and illness prevention, facilitate the early identification of disease symptoms and treatment choices, and simplify the communication between healthcare professionals and patients (Tan and Goonawardene 2017; Risling et al. 2017). Seeking and finding health-related information online are the first steps to become eHealth literate. Unequal access to information can determine low eHealth literacy by jeopardizing understanding, appraisal and application of health-related information in a digital environment. In other words, inequalities in information accessibility can produce inequalities also in the health and social well-being of populations (Estacio et al. 2017).
In view of this, it is important to identify and understand who health information users are and which factors determine their utilization of health information online. There is still no consensus among the scientific community regarding which social and demographic characteristics are associated with online health information seeking (Nölke et al. 2015). Therefore, specific studies on the profiles of online health-related information users are needed.
The present work aims at (1) identifying which are the social and demographic factors that better describe the profile of health information users in 28 European countries and (2) studying their association with online health information usage.
In relation to these objectives, the following hypotheses were defined:
H1 Internet use to search for health-related information varies among European countries.
H2 Although ICT access has increased in the European context, divides in the use of health information online can still be found.
H3 Individuals who have poor health present a higher use of health information online.
H4 Individuals with poor knowledge of health topics use more the Internet to decrease their health information gap.
Methods
Data and variables
We have used data from the Flash Eurobarometer No. 404: Eurobarometer on digital health literacy, which was carried out in September 2014 in the 28 EU Member States: Austria, Belgium, Bulgaria, Croatia, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden and UK. The Flash Eurobarometer is a survey conducted by the Leibniz Institute for the Social Sciences on behalf of the European Commission aimed at monitoring the public opinion on a wide range of topics. The specific survey No. 404 assessed the extent to which European citizens use the Internet and online resources to manage their own health. This dataset had a sample size of 26,566 individuals living in private households, regardless of nationality or citizenship, language or legal status. Interviews were carried using the computer-aided telephonic interview (CATI) system, and respondents were called on both fixed lines and mobile phones. The sample design applied in all countries was multi-stage random. A more detailed description of the Flash Eurobarometer No. 404, including sample sizes, question descriptions and response rates per countries, is provided in the website of the European Commission (EU Open Data Portal 2015).
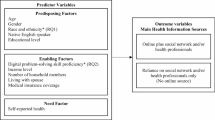
For this specific study, the dependent variable was the use of the Internet to search for health-related information corresponding to the question Q2 of the Flash Eurobarometer No. 404: ‘Within the last 12 months, have you used the Internet to search for health-related information? This could include information on an injury, a disease, illness, nutrition, improving health, etc.’ (‘No’, ‘Yes’). The following items were selected as explanatory variables: Q1, frequency of Internet use (‘Never used for health purposes’, ‘Two or three times a month’, ‘Approximately once a week’, ‘Two or three times a week’, ‘Everyday/Almost every day’); Q33, self-rated health (‘Bad’, ‘Good’); Q34, long-standing illness (‘No long-standing illness’, ‘One long-standing illness’, ‘Multiple long-standing illness’); D4, education (continuous variable measured in year of full education); D2, gender (‘Male’, ‘Female’); D1, age group (‘15–24’, ‘25–34’, ‘35–44’, ‘45–54’, ‘55–64’, ‘65+’); Q36, knowledge of health topics (‘Bad’, ‘Good’); and D18, mobile availability (‘No’, ‘Yes’).
Statistical analysis
Descriptive and inferential statistical methods were applied. Given that the outcome variable was binary and the hierarchical structure of individuals (level-1 units) clustered within countries (level-2 units), a multilevel logistic regression model was used to analyse this nested structure. This analytical solution enabled the study of variations in the use of the Internet to search for health information related to individuals within their particular countries.
Once the relevant indicators were identified in the logistic regression analysis, propensity score matching (PSM) was used to estimate the association considering the whole set of explanatory variables (Austin 2011), so that we could measure and compare the specific divides in the use of the Internet for searching health information among the 28 European countries. According to this approach, a propensity score was calculated for each subject and used to create comparable group pairs based on the statistically significant predictors in the logistic regression analysis (i.e. Gender: Female vs Male; Long-limiting standing illness: Yes vs No; Knowledge: Good vs Bad; and Age: 45+ years vs 15–44 years). Using this binary grouping, divides in the use of Internet to search for health-related information were assessed.
Taking into account the fact that the exposure groups were sufficiently large to warrant reliable estimation of the scores, the use of this analytical technique permitted to balance the distribution of the observed confounders and to remove possible bias that might arise due to these sets of predictors (Austin 2011). In contrast to traditional multivariate techniques, the use of PSM can reduce errors in the estimation of the effect of the confounders on the outcome, while allowing also for the independent assessment of the balance of the observed covariates between groups to be compared (Cepeda et al. 2003).
Stata® 14.0 was used to perform data analysis. Survey sampling weights were applied to account for differential response and non-response rates across countries.
Results
User profiles
Table 1 describes the percentage of individuals in the EU-28 that used the Internet for searching health-related information in the 12 months prior to the survey. In the study sample, 72% of Europeans had used the Internet to search for health-related information during this period. The percentage of female users (77.0%) was higher than the males’ one (65.4%). According to the age group, younger individuals presented a higher usage of the Internet to search for health-related information compared with older groups (81.3% for 25–34 years vs 57.5% for individuals aged over 65 years). Statistically significant differences by self-rated health (SRH) were not found. Finally, people having one or more than one long-standing illness(es) presented a higher use of the Internet to search for health-related information (70.1% people without a long-standing illness vs 76.1% people having more than one long-standing illness). Except for SRH (p > 0.05), all differences were statistically significant at the level of p < 0.01.
Table 2 shows the online sources used to look for health-related information only among the 7077 users who reported having looked for information through any information channel. These sources were mainly official health organizations’ websites (28.3%), followed by generalized search engines (27.3%). Other remarkable information sources were social networks (19.5%) and specific websites and blogs (15.2%). Health-specific mobile apps, online newspapers and magazines, and patient organizations’ websites were less used (below 10%). When examining differences per gender, men used more search engines, while women preferred health organization websites. Social networks were more consulted by women (χ2 = 21.107; p < 0.001).
Topics searched among these users were lifestyle choices (27.4%), healthcare professionals (22.8%), information on vaccinations (14.1%), pharmaceutical products (13.7%) and testimonials on health topics (13%) (Table 3). A smaller proportion of people looked for information on age care, childbirth and psychological well-being (below 5%). Differences per gender were small. However, men were more interested in lifestyle choices than women, while women were more interested in healthcare professionals, vaccinations, and pregnancy and childbirth than men (χ2 = 40.090; p < 0.001).
Social determinants of Internet use for health purposes
Table 4 illustrates the multilevel logistic regression model built to explain the use of the Internet in the previous 12 months to search for health-related information. As we can observe, Internet search for health information significantly varied among European countries (H1). The probability of using the Internet for health purposes increased linearly with the frequency of Internet use, but exclusively among those who presented a frequent use of the Internet (i.e. ‘two or three times a week’, and ‘everyday’). A similar pattern was also found for mobile phone availability, i.e. those who had mobile phones used them also for health information seeking. Compared with men and older groups, women and younger age groups had a higher likelihood of using the Internet for health. Number of education years had a direct relationship with the use of the Internet to search for health-related information. A better self-reported knowledge of health topics and having long-standing illnesses also increased the probability of using the Internet for health information (H2). However, the relationship between self-rated health and the use of the Internet was not found to be statistically significant.
The PSM analysis supported the results of the multilevel logistic model (Table 5). Thus, women had higher propensity to search for health topics on the Internet. The propensity scores also showed that the likelihood of using the Internet to search for health-related information significantly increased with having one or more long-standing illness (H3) and a good knowledge of health topics (H4). Inversely, the increase of age reduced the use of the Internet.
Finally, the resulting propensity scores were used to predict and graphically compare the divides in the use of health information online among the 28 European countries. Figure 1 shows the population risk of limited use of the Internet for health-related information according to gender, age group, knowledge of health topics and having a long-standing illness (i.e. the indicators that explained differences in the outcome variable). In accordance with the results described above, being a male, being above 45 years old and not suffering from a long-term illness increased the risk of a limited use of the Internet to search for health-related information and subsequently the risk of poor eHealth literacy. On the other hand, the association of the knowledge of health topics with the use of the Internet varied across countries.

Data source: Flash Eurobarometer No. 404, EU-28 countries, 2014
Divides in the use of the Internet to search for health-related information across European countries. Note: Central dashed line indicates the average use in Europe.
Discussion
To our knowledge, this is one of the first studies measuring the differences in the search for online health information according to social and demographic factors in a large set of European countries. We compared the use of the Internet to search for health information across different variables that have been considered as relevant in previous literature (Czaja et al. 2006; Gracia and Herrero 2009; Renahy et al. 2010; Neter and Brainin 2012; Kontos et al. 2014; Bidmon and Terlutter 2015; Koo et al. 2016; Estacio et al. 2017; Baumann et al. 2017; Escoffery 2017): social and demographic factors (gender, age, educational level); self-reported health conditions (self-rated health status, long-standing illnesses); health knowledge (i.e. the degree of knowledge on health topics); and the access to the Internet for health-related information (frequency of use of the Internet for health purposes, availability of mobile phones).
Our results show that there are significant differences in the use of health information according to gender, age, education, suffering from a long-term illness and health-related knowledge among European countries (first and second hypotheses of our study). Females searched health-related information on the Internet more frequently than males and also used for health purposes other technological means such as mobile phones. These findings are in line with those of previous studies conducted in France, Germany and USA (Renahy et al. 2010; Bidmon and Terlutter 2015; Baumann et al. 2017; Escoffery 2017). A possible explanation to this gendered use is that women are more likely caregivers, which means that they search for information also for people under their care (e.g. children) which increases their chances to access the Internet for health-related purposes (Renahy et al. 2010; Bidmon and Terlutter 2015; Escoffery 2017). According to previous research, the use of the Internet decreases with age due to the ‘generational shift’ in the general use of technology (Hill et al. 2008; Neter and Brainin 2012; Kontos et al. 2014; Estacio et al. 2017). Our findings are coherent with this assumption since the use of the Internet for health gradually declines with age. This occurs in females earlier than in males, which would denote that the digital generational shift in women might be wider. Indeed, two previous studies found that women ascribe lower self-perceived digital competences (Bidmon and Terlutter 2015) and higher anxiety about using computers (Czaja et al. 2006) compared to men.
The availability of mobile phones is a second digital divide that is significantly associated with the use of online health-related information. This is in line with studies reporting that mobile apps are commonly used for health purposes today (Bidmon and Terlutter 2015; Escoffery 2017).
Males above 45 years old and without long-term illnesses were at higher risk of not looking for health-related information online. This was a well-defined pattern across all countries. A lower knowledge of health issues increased the overall risk of low Internet usage for these purposes in the majority of countries, irrespective of any geographical cluster.
Previous research suggested that a low educational level is a barrier to Internet usage (Czaja et al. 2006; Neter and Brainin 2012; Kontos et al. 2014; Koo et al. 2016; Estacio et al. 2017). In line with this, our results showed significant educational influences on the use of the Internet for health purposes. The likelihood of use of the Internet to look for health-related information increased with the number of study years.
The third hypothesis stated that individuals with poor health use more the Internet to seek for health information than individuals with good health conditions. Contrary to our hypothesis, results showed that self-rated health did not have a significant influence on the usage of the Internet for health purposes. Similarly, this association was not found in a study on general Internet usage in older people where different socio-economic factors were considered (Gracia and Herrero 2009). Another study found this relationship in women (Renahy et al. 2010). This finding might indicate that the search of health-related information is performed not only by people presenting a health problem (either mild or severe), but also by people who might be interested in taking care of their well-being with a health promotion and prevention purpose (Renahy et al. 2010; Baumann et al. 2017).
However, the higher likelihood of usage of ICT by people having chronic conditions is a relevant finding. It suggests that the use of the Internet for health purposes is considered as an important solution to appropriately meet the complex care needs of people with several illnesses (Barbabella et al. 2016).
The fourth hypothesis pointed out a negative relationship between health knowledge and usage of the Internet. Conversely, our results showed a significant association between high knowledge of health topics, as a proxy of eHealth literacy, and the use of the Internet for seeking health-related information. This relationship might also be interpreted the other way round: knowledge of health topics increases because of the use of ICT with health purposes (Ramtohul 2015).
This study presents some limitations that should be addressed in future works. First, the analysis did not include socio-economic factors such as income or occupational status, which were found to be associated with online health information-seeking behaviours with different degrees of prediction in previous studies (Kontos et al. 2014; Baumann et al. 2017). Taking into account the difficulty in contrasting the household income among this large set of countries, we decided to use education as a more comparable indicator of socio-economic status, but future studies should incorporate additional measures that capture the effect of economic differences between social groups. Second, we only explored the first dimension of eHealth literacy, i.e. access to online health-related information, without using validated health literacy scales (Liu et al. 2018). Further studies should explore how socio-demographic and socio-economic factors may influence other dimensions of eHealth literacy, especially the impact of online health information on healthcare decision-making. Third, even though this study identified country-level differences in the Internet usage for health purposes by combining multilevel logistic regression and PSM analysis, it did not explore contextual effects of specific macro-level indicators that might be relevant to understand between-countries variations. Nevertheless, this study sets the starting point to develop this promising line of research.
In conclusion, this study shows that although the degree of accessibility to online information has gradualy increased in the last years, some digital divides still persist in the use of health information online, as reported in our first hypothesis. Our findings suggest that those who use the Internet to seek for health contents are moved and motivated by essential differences based on age, gender, presence of a long-term illness and the degree of knowledge on health topics. A poor health status is associated with a higher Internet usage for health purposes, but only in the case of those having chronic conditions. Our last hypothesis was not verified since a poor health-related knowledge was not associated with a higher search for health information on the Internet. Maybe, a lower health knowledge could be associated with a lower motivation to look for health information. Our results show that there is still a need to increase eHealth literacy levels, especially for males over 45 years old not suffering from a long-term illness. This is highly relevant to reduce the misuse of poor or untrustworthy health information that might contribute to higher health disparities among this specific population. Finally, our study supports the relevance of identifying populations at risk for health misinformation who might be fundamental targets of eHealth literacy interventions such as educational programmes, websites that provide clear and trustworthy health content, and other communication tools (e.g. apps and social medial platforms) conveying evidence-based knowledge.
References
Allcott H, Gentzkow M, Yu C (2019) Trends in the diffusion of misinformation on social media. Res Politics 6:1–8. https://doi.org/10.1177/2053168019848554
Austin PC (2011) An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar Behav Res 46:399–424. https://doi.org/10.1080/00273171.2011.568786
Barbabella MG, Melchiorre S, Quattrini R et al (2016) How can eHealth improve care for people with multimorbidity in Europe?. Eur Obs Health Syst Policies, Berlin
Baumann E, Czerwinski F, Reifegerste D (2017) Gender-specific determinants and patterns of online health information seeking: results from a representative German health survey. J Med Internet Res 19:e92. https://doi.org/10.2196/jmir.6668
Bidmon S, Terlutter R (2015) Gender differences in searching for health information on the internet and the virtual patient-physician relationship in Germany: exploratory results on how men and women differ and why. J Med Internet Res 17:e156. https://doi.org/10.2196/jmir.4127
Bratu S (2018) Fake news, health literacy, and misinformed patients: the fate of scientific facts in the era of digital medicine. Anal Metaphys 17:122–127. https://doi.org/10.22381/AM1720186
Cepeda MS, Boston R, Farrar JT, Strom BL (2003) Comparison of logistic regression versus propensity score when the number of events is low and there are multiple confounders. Am J Epidemiol 158:280–287. https://doi.org/10.1093/aje/kwg115
Chou W-YS, Oh A, Klein WMP (2018) Addressing health-related misinformation on social media. JAMA 320:2417. https://doi.org/10.1001/jama.2018.16865
Coulter A, Ellins J, Swain D et al (2006) Assessing the quality of information to support people in making decisions about their health and healthcare. Picker Institute Europe, Oxford
Czaja SJ, Charness N, Fisk AD et al (2006) Factors predicting the use of technology: findings from the Center for Research and Education on Aging and Technology Enhancement (CREATE). Psychol Aging 21:333–352. https://doi.org/10.1037/0882-7974.21.2.333
Devine T, Broderick J, Harris LM et al (2016) Making quality health websites a national public health priority: toward quality standards. J Med Internet Res 18:e211. https://doi.org/10.2196/jmir.5999
Escoffery C (2017) Gender similarities and differences for e-Health behaviors among U.S. adults. Telemed e-Health. https://doi.org/10.1089/tmj.2017.0136
Estacio EV, Whittle R, Protheroe J (2017) The digital divide: examining socio-demographic factors associated with health literacy, access and use of internet to seek health information. J Health Psychol. https://doi.org/10.1177/1359105317695429
EU Open Data Portal (2015) Flash Eurobarometer 404: Eurobarometer on digital health literacy—datasets. In: EU open data portal. http://data.europa.eu/euodp/en/data/dataset/S2020_404. Accessed 1 June 2019
European Commission (2019) Tackling online disinformation. https://ec.europa.eu/digital-single-market/en/tackling-online-disinformation. Accessed 20 Nov 2019
Eurostat (2018) Digital economy and society statistics—households and individuals. In: Eurostat—stat. Explain. https://ec.europa.eu/eurostat/statistics-explained/index.php/Digital_economy_and_society_statistics_-_households_and_individuals#Internet_access. Accessed 1 June 2019
Gracia E, Herrero J (2009) Internet use and self-rated health among older people: a national survey. J Med Internet Res 11:e49. https://doi.org/10.2196/jmir.1311
Hesse BW, Moser RP, Rutten LJ (2010) Surveys of physicians and electronic health information. N Engl J Med 362:859–860. https://doi.org/10.1056/NEJMc0909595
Hill R, Beynon-Davies P, Williams MD (2008) Older people and internet engagement: acknowledging social moderators of internet adoption, access and use. Inf Technol People 21:244–266. https://doi.org/10.1108/09593840810896019
Iverson S, Howard K, Penney B (2008) Impact of internet use on health-related behaviors and the patient-physician relationship: a survey-based study and review. J Am Osteopath Assoc 108:699–711
Kontos E, Blake KD, Chou WYS, Prestin A (2014) Predictors of eHealth usage: insights on the digital divide from the health information national trends survey 2012. J Med Internet Res 16:e172. https://doi.org/10.2196/jmir.3117
Koo M, Lu M-C, Lin S-C (2016) Predictors of internet use for health information among male and female Internet users: findings from the 2009 Taiwan National Health Interview Survey. Int J Med Inform 94:155–163. https://doi.org/10.1016/J.IJMEDINF.2016.07.011
Liu H, Zeng H, Shen Y et al (2018) Assessment tools for health literacy among the general population: a systematic review. Int J Environ Res Public Health 15:1711. https://doi.org/10.3390/ijerph15081711
McMullan M (2016) Patients using the Internet to obtain health information: how this affects the patient-health professional relationship. Patient Educ Couns 63:24–28. https://doi.org/10.1016/j.pec.2005.10.006
Neter E, Brainin E (2012) eHealth literacy: extending the digital divide to the realm of health information. J Med Internet Res 14:e19. https://doi.org/10.2196/jmir.1619
Nölke L, Mensing M, Krämer A, Hornberg C (2015) Sociodemographic and health-(care-)related characteristics of online health information seekers: a cross-sectional German study. BMC Public Health. https://doi.org/10.1186/s12889-015-1423-0
Norman CD, Skinner HA (2006) eHealth literacy: essential skills for consumer health in a networked world. J Med Internet Res 8:e9. https://doi.org/10.2196/jmir.8.2.e9
Ramtohul I (2015) The adoption of e-health services: comprehensive analysis of the adoption setting from the users perspective. Health Policy Technol 4:286–293. https://doi.org/10.1016/j.hlpt.2015.04.007
Renahy E, Parizot I, Chauvin P (2010) Determinants of the frequency of online health information seeking: results of a web-based survey conducted in France in 2007. Inform Health Soc Care 35:25–39. https://doi.org/10.3109/17538150903358784
Risling T, Martinez J, Young J, Thorp-Froslie N (2017) Evaluating patient empowerment in association with eHealth technology: scoping review. J Med Internet Res 19:e329. https://doi.org/10.2196/jmir.7809
Stevenson FA, Kerr C, Murray E, Nazareth I (2007) Information from the internet and the doctor-patient relationship: the patient perspective—a qualitative study. BMC Fam Pract 8:47. https://doi.org/10.1186/1471-2296-8-47
Tan SS-L, Goonawardene N (2017) Internet health information seeking and the patient-physician relationship: a systematic review. J Med Internet Res 19:e9. https://doi.org/10.2196/jmir.5729
TNS Political and Social (2014) European citizen’s digital health literacy (Flash Eurobarometer 404)
Tonsaker T, Bartlett G, Trpkov C (2014) Health information on the internet. Gold mine or minefield? J R Soc Promot Health 60:407–410
Vance K, Howe W, Dellavalle RP (2009) Social internet sites as a source of public health information. Dermatol Clin 27:133–136. https://doi.org/10.1016/j.det.2008.11.010
Waszak PM, Kasprzycka-Waszak W, Kubanek A (2018) The spread of medical fake news in social media—the pilot quantitative study. Health Policy Technol 7:115–118. https://doi.org/10.1016/J.HLPT.2018.03.002
WHO (2014) The health internet: governing principles for a health top-level domain. In: WHO. http://www.who.int/ehealth/programmes/governance/en/index3.html. Accessed 1 June 2019
Acknowledgements
We would like to acknowledge the support of the University Institute of Research in Social Sustainable Development (INDESS) at the University of Cádiz, and the Ramon and Cajal programme (MIMECO), who contributed to the development of the present manuscript.
Funding
JAG was subsidized by the Ramon and Cajal programme of the Ministry of Economy and Business, European Social Fund (RYC-2016-19353).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Alvarez-Galvez, J., Salinas-Perez, J.A., Montagni, I. et al. The persistence of digital divides in the use of health information: a comparative study in 28 European countries. Int J Public Health 65, 325–333 (2020). https://doi.org/10.1007/s00038-020-01363-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-020-01363-w