
Abstract
Objectives
Our study aimed at determining the prevalence of selected infectious diseases among recently arrived Eritrean refugees in Switzerland.
Methods
In this cross-sectional study, asymptomatic Eritrean migrants aged ≥16 years who arrived <24 months ago were recruited at refugee centres in Switzerland. Infectious disease screening included serology for HIV, hepatitis B and C, syphilis and schistosomiasis, polymerase chain reaction (PCR) for malaria, stool microscopy for helminths and intestinal protozoa and circulating cathodic antigen (CCA) testing in urine for schistosomiasis.
Results
Among 107 participating Eritrean refugees, point-of-care CCA urine test for Schistosoma mansoni was positive in 43 patients (40.2%; 95% CI 31.9–49.5). Stool microscopy detected eggs of S. mansoni in 23 (21.5%; 95% CI 13.7–29.3), Hymenolepis nana in 11 (10.3%; 95% CI 4.5–16.0), and cysts of Giardia intestinalis in 7 participants (6.5%: 95% CI 1.9–11.2). Two tested positive for hepatitis B (1.9%; 95% CI 0.0–4.4) and one for syphilis (0.9%; 95% CI 0.0–2.8), none tested positive for HIV or hepatitis C. Malaria PCR was positive in six participants (5.6%; 95% CI: 1.2−9.9).
Conclusions
Given the high prevalence of S. mansoni infection and potentially severe long-term sequelae of untreated schistosomiasis, routine screening for schistosomiasis in refugees from Schistosoma-endemic regions should be recommended.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Large numbers of refugees arriving in Europe has put migrants’ health high up on the public health agenda (Jakab et al. 2015). A review of the World Health Organization (WHO) European Regional Office on migrants’ health emphasises that evidence of poor health among refugees is mostly confined to maternity and mental health issues (Bradby et al. 2015). Meanwhile, there is a paucity of data on prevalence and burden of infectious diseases among newly arriving refugees in Europe. Among the notifiable diseases in Germany, varicella, tuberculosis, hepatitis B (HBV) and C (HCV), and influenza were the top five infectious diseases among asylum seekers in 2016 (Robert Koch Institute 2016). However, this list of infectious diseases is mainly driven by a high share of asylum seekers from Syria, Afghanistan and Iraq, and to a lesser extent from Albania and Kosovo (Eurostat 2016). Of note, in some European countries, refugees from north-eastern parts of Africa (particularly Eritrea) are the dominant group of migrants. In Switzerland and the United Kingdom, Eritreans made up the largest group among refugees arriving in 2015. Moreover, Eritrea was among the top five countries of origin among migrants entering the Netherlands, Norway, Sweden, Denmark and Malta (EJPD 2016). Most Eritrean refugees travel via Ethiopia and Sudan to Libya from where they cross the Mediterranean Sea to Italy (Fig. 1). An estimated 5000 people, mostly young men, are leaving Eritrea every month and one-quarter of refugees arriving in Italy in 2015 were Eritreans (Laub 2016).

(Source: UNHCR, accessed December 1, 2016 at: http://www.cfr.org/eritrea/authoritarianism-eritrea-migrant-crisis/p37239)
Migration route of Eritrean asylum seekers from Eritrea to Europe
Recent reports from Germany, Sweden and Israel highlight a high incidence of Plasmodium vivax malaria relapses among Eritrean refugees (Kopel et al. 2010; Saidel-Odes et al. 2011; Sonden et al. 2014; Roggelin et al. 2016). Moreover, case series and outbreak reports document high prevalence of scabies and several cases of louse-borne relapsing fever among Eritrean refugees (Hoch et al. 2015; Goldenberger et al. 2015; Jaton et al. 2016). Screening of migrants from Africa arriving in Italy revealed high prevalence of schistosomiasis, particularly among individuals from Mali and Côte d'Ivoire (Beltrame et al. 2017). Yet, to our knowledge, there is no study systematically screening presumably healthy refugees from Eritrea on potentially asymptomatic chronic infectious diseases with potentially severe long-term sequelae.
Since a decade, Eritreans represent an important group among asylum seekers in Switzerland. In 2015 alone, 9666 Eritrean refugees entered the country, representing one-quarter of all asylum seekers (Laub 2016). The aim of this study was to evaluate the prevalence of selected infectious diseases (HIV, HBV, HCV, syphilis, malaria, soil-transmitted helminths, schistosomiasis and intestinal protozoa) among asymptomatic, recently arrived refugees of Eritrean origin. Selection of infectious diseases was based on the possibility of an easy and rapid diagnosis, assumed relevance in the study-population, and the importance to the individual’s health. Eritrean refuges who arrived in Switzerland <24 months ago were screened using a suite of standardised, quality-controlled diagnostic approaches.
Methods
Study population and sample collection
This cross-sectional study screened Eritrean refugees living in centres for asylum seekers in two cantons of north-western Switzerland (Basel-Stadt and Basel-Landschaft) for the following conditions: soil-transmitted helminth and intestinal protozoa infections, schistosomiasis, malaria, syphilis, HIV, HBV and HCV.
Figure 2 displays recruitment and study-flow of participants. Using the cantonal refugee registries, all immigrants registered in these two cantons, aged 16 years and above who arrived from Eritrea within the past 24 months, were contacted through invitation letters written in both, English and Tigrigna (an Eritrean language), and followed-up by a phone call. All consenting asymptomatic Eritrean migrants were enrolled. Asymptomatic was defined as currently not having any physical complaints that led the participant to seek medical care. Exclusion criteria were: (1) no written informed consent; (2) age <16 years; (3) pregnancy or lactation; and (4) manifesting illness at the moment of recruitment. As this study looked at imported infectious diseases, immigrants who had been living in Switzerland for more than 24 months were not considered for enrolment.

Flow of recruitment of study participants
At enrolment, participants filled in a questionnaire on their socio-demographic background and medical history written in Tigrigna. An investigator fluent in Tigrigna was always present to clarify questions where needed. Socio-demographic variables collected are displayed in Table 1. After administering a questionnaire and a clinical assessment by the study physician, participants underwent phlebotomy, provided a urine sample and received two stool containers, one for a native sample and one containing sodium acetate-acetic acid-formalin (SAF) as fixative. Participants were advised to fill the containers during the next two bowel movements, first the SAF-fixed container (approximately 2 g of stool fixed in 10 ml of SAF) and then the native container (approximately 50 g of native stool). Both samples were brought to the laboratory and processed within 24 h. Recruitment lasted for 10 months (from February to November 2016).
Informed oral and written consent was obtained from all participants included in the study. In case of pathologic findings in the screening, participants received appropriate care at the Swiss Tropical and Public Health Institute (Swiss TPH, Basel, Switzerland) or were referred to their general practitioner or another clinic as appropriate. Treatment of parasitic infections was provided at Swiss TPH and followed our recently published guidelines (Neumayr 2016).
Laboratory procedures
Serological screening for HBV (HBS antigen), HCV, HIV, and syphilis [Treponema pallidum haemagglutination (TPHA)] followed standardised diagnostic algorithms. Enzyme-linked immunosorbent assay (ELISA) and immunofluorescent anti-body tests were used for Schistosoma spp. serology (soluble egg-antigen and worm adult-antigen) and ELISA for Strongyloides stercoralis serology. Screening for schistosomiasis was complemented by detection of circulating cathodic antigen (CCA) in urine using a point-of-care test developed by Rapid Medical Diagnostics (Pretoria, South Africa) (Rapid Diagnostics 2016). For detection of helminth ova and cysts of intestinal protozoa in the stool, the SAF-fixed stool container was centrifuged, sediment was treated with ether and centrifuged again (Utzinger et al. 2010). Stool from the native tube was filtered for sedimentation. Sediments of both samples were then assessed by experienced microscopists at Swiss TPH. Screening for malaria was performed through polymerase chain reaction (PCR) using QIAamp DNA Mini Kit (CDC 2016).
Statistical analysis
Data were collected on paper forms and subsequently entered in EpiInfo version 7 [Centers for Disease Control and Prevention (CDC), Atlanta, USA] using double data entry. Statistical analysis is descriptive. Continuous variables are reported as median with inter-quartile range (IQR); prevalence is reported as percentage with 95% confidence intervals (CI). Analyses were run on Stata version 13 (StataCorp LP; College Station, USA) and R Studio (RStudio, Inc; Boston, USA).
Reporting in this manuscript follows the STROBE guidelines for cross-sectional studies (https://www.strobe-statement.org).
Results
Based on the asylum registries in Basel-Stadt and Basel-Landschaft, 151 asylum seekers from Eritrea aged ≥16 years had arrived <24 months ago in Switzerland. Out of these, 121 responded to the invitation letter sent. After briefing and clarification of open questions on the phone, 107 were eligible and consented to participate. Most participants were males (89%) with a median age of 25 years (Table 1).
Findings from infectious diseases screening are summarised in Table 2. Clinical assessment revealed scabies in 10% (95% CI 4.5–16.1). None of the participants were tested positive for HIV or HCV. The two patients reactive for HBS antigen had a HBV DNA viral load of 708 and 191 IU/ml, normal values of transaminases and unremarkable liver function tests. One participant had a reactive TPHA and VDRL without clinical signs of syphilis. Malaria PCR was positive in six (5.6%; 95% CI 1.2–9.9) participants; four were P. vivax and two P. falciparum. All were negative in thin blood films.
Stool microscopy revealed ≥1 pathogenic parasite in 36 (33.6%; 95% CI 24.7–42.5) participants: ova of S. mansoni in 23 (21.5%; 95% CI 13.7–29.3), ova of Hymenolepis nana in 11 (10.3%; 95% CI 4.5–16.0) and cysts of Giardia intestinalis in seven (6.5%; 95% CI 1.9–11.2) participants. The POC–CCA urine cassette test revealed 43 (40.2%; 95% CI 31.9–49.5) positive results for schistosomiasis, while serology was positive in 54 (50.5%; 95% CI 41.0–60.0) participants. Considering egg detection by microscopy alone, 23 (21.5%; 95% CI 13.7–29.3) participants were identified with active S. mansoni infection. If the result of the POC–CCA test is added, the number of detected active schistosomiasis cases doubles to 45 (42.1%). Only one participant had a positive Strongyloides serology.
Discussion
This cross-sectional study conducted in Switzerland screened 107 asymptomatic Eritrean immigrants for a suite of infectious diseases. We found a surprisingly high prevalence of previously undiagnosed schistosomiasis. Indeed, stool microscopy revealed a prevalence of S. mansoni of 21.5%. Considering the combined results from stool microscopy and the more sensitive POC–CCA urine cassette test (van Lieshout et al. 2000; Colley et al. 2013), the prevalence of S. mansoni was as high as 42%. Other, less frequently diagnosed parasitic infections were giardiasis, H. nana infection, malaria and one case of strongyloidiasis. While the prevalence of HIV and HCV was nil, two cases of HBV, both with low viral load and normal liver enzymes, and one case of syphilis were detected. Based on our findings and given the potential serious consequences of untreated schistosomiasis, routine screening of asylum seekers from Eritrea for schistosomiasis should be considered.
How do our data compare to previous studies? Despite high numbers of refugees arriving from Eritrea, data on their health status are scarce. There are several studies reporting on infectious diseases in refugees in general. However, most included a very small share of individuals coming from Eritrea. Most studies report higher HIV, HBV, HCV and syphilis infection rates in sub-Saharan African migrants. For example, Russo and colleagues conducted a survey among asylum seekers in Italy, including 99 immigrants originating from Africa, 60 (61%) of whom were from Eritrea. The overall prevalence of syphilis, HIV, HCV and HBV was 6.1, 5.2, 2.3 and 11.3%, respectively (Russo et al. 2016). A recent review reports a pooled HCV prevalence of 4.4% among migrants from sub-Saharan Africa (Greenaway et al. 2015). Among serum samples collected in Libya, HIV prevalence was 2.2% among Eritreans, 1.1% were HCV/HIV co-infected (Daw et al. 2016). The relatively low HIV prevalence in asylum seekers from Eritrea is in line with the adult HIV prevalence in Eritrea itself, that is estimated at 0.6% (“Eritrea| UNAIDS” 2015).
There are only few studies investigating intestinal parasitic infections among immigrants arriving in Europe. Among 1930 immigrants from sub-Saharan Africa in Spain, 14.4% had schistosomiasis, as revealed by microscopy. However, nearly all study participants were from West Africa (Cobo et al. 2016). A recent study by Abu-Madi and colleagues found that 5.8% of refugees from North and sub-Saharan Africa had helminths in Qatar (Abu-Madi et al. 2016), none had schistosomiasis. In a screening study among children and adolescent refugees arriving in Germany in 2015, 194 individuals originated from sub-Saharan Africa. Out of these, 17.5% carried pathogenic stool parasites and 24.7% had a positive Schistosoma serology (Theuring et al. 2016). However, only 16 (8.2%) of these study participants were Eritreans (S. Theuring, personal communication). Beltrame and colleagues found a S. mansoni prevalence of 38% among refugees from sub-Saharan Africa arriving in Italy. This study did, however, not include Eritrean refugees (Beltrame et al. 2017).
The last survey on schistosomiasis in Eritrea was conducted in 2002 and found an overall prevalence of 2.4% among children (GAHI 2016). A recently published geostatistical analysis estimates the schistosomiasis prevalence in Eritrea at 8.8% (Lai et al. 2015).
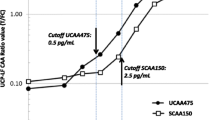
Among our study participants, considering only those with eggs detected in stool, 21.5% had schistosomiasis. The prevalence, however, doubles if all with positive CCA in urine and/or egg detection in faeces are considered as having active schistosomiasis (42.1%). This is in line with a recently published systematic review, where pooled median schistosomiasis prevalence based on the POC–CCA cassette test was 2.5 times higher than by microscopy in populations where 20–29% had S. mansoni eggs detected by Kato-Katz (Kittur et al. 2016). This may be partly explained by a higher sensitivity of POC urine CCA (Ochodo et al. 2015). On the other hand, the CCA test can lead to false positive results in case of haematuria, urinary tract infections, or presence of certain glycoproteins in the urine (Polman et al. 2000; Rapid Diagnostics 2016). Further studies will have to determine the specificity of CCA in migrant populations, additional more sensitive and specific tests, such as circulating anodic antigen (CAA) may be an option (van Lieshout, Polderman, and Deelder 2000). As reported elsewhere, sensitivity and specificity of CCA against stool microscopy was 91 and 74%, respectively (Chernet et al. 2017).
In conclusion, we found a surprisingly high prevalence of schistosomiasis in Eritrean refugees who arrived in Switzerland <24 months before screening. Given the well-known potentially severe long-term consequences, routine screening of immigrants from Eritrea for schistosomiasis should be recommended upon their arrival. Moreover, screening of all migrants arriving from or crossing through Schistosoma-endemic regions may be considered. The rapid and inexpensive POC–CCA urine cassette test offers an opportunity, as already shown in a preliminary study in neighbouring Germany (Becker et al. 2015). However, additional research is needed to determine if individuals with a positive CCA but negative serology and microscopy should be treated for schistosomiasis.
References
Abu-Madi MA, Behnke JM, Ismail A, Boughattas S (2016) Assessing the burden of intestinal parasites affecting newly arrived immigrants in Qatar. Parasites Vectors 9:619. doi:10.1186/s13071-016-1906-6
Becker SL, Marti H, Zimmermann S, Vidacek D, Herrmann M, Utzinger J, Schnabel PA, Bohle RM (2015) Application in Europe of a urine-based rapid diagnostic test for confirmation of schistosoma mansoni infection in migrants from endemic areas. Euro Surveill. doi:10.2807/1560-7917.ES2015.20.23.21151
Beltrame A, Buonfrate D, Gobbi F, Angheben A, Marchese V, Monteiro GB, Bisoffi Z (2017) The hidden epidemic of schistosomiasis in recent African immigrants and asylum seekers to Italy. Eur J Epidemiol. doi:10.1007/s10654-017-0259-6
Bradby H, Humphris R, Newall D, Phillimore J (2015) Public health aspects of migrant health: a review of the evidence on health status for refugees and asylum seekers in the European region. WHO Health Evidence Network Synthesis Reports. Copenhagen: WHO Regional Office for Europe. http://www.ncbi.nlm.nih.gov/books/NBK379418/. Accessed 10 Dec 2016
CDC (2016) CDC-DPDx-Malaria-Diagnostic Findings. https://www.cdc.gov/dpdx/malaria/dx.html. Accessed 10 Dec 2016
Chernet A, Kling K, Sydow V, Kuenzli E, Hatz C, Utzinger J, Lieshout L, Marti H, Labhardt ND, Neumayr A (2017) Accuracy of diagnostic tests for Schistosoma mansoni infection in asymptomatic Eritrean refugees: serology and POC-CCA against stool microscopy. Clin Infectious Dis. doi:10.1093/cid/cix366
Cobo F, Salas-Coronas J, Cabezas-Fernández TM, Vázquez-Villegas J, Cabeza-Barrera MI, Soriano-Pérez MJ (2016) Infectious diseases in immigrant population related to the time of residence in Spain. J Immigr Minor Health 18:8–15. doi:10.1007/s10903-014-0141-5
Colley DG, Binder S, Campbell C, King CH, Tchuenté LT, N’Goran EK, Erko B et al (2013) A five-country evaluation of a point-of-care circulating cathodic antigen urine assay for the prevalence of Schistosoma mansoni. Am J Trop Med Hyg 88:426–432. doi:10.4269/ajtmh.12-0639
Daw MA, El-Bouzedi A, Ahmed MO, Dau AA, Agnan MM, Drah AM, Deake AO, In association with Libyan Study Group of Hepatitis & HIV (2016) Prevalence of human immune deficiency virus in immigrants crossing to Europe from North and Sub-Saharan Africa. Travel Med Infect Dis. doi:10.1016/j.tmaid.2016.10.008
EJPD (2016) Asylstatistik:Staassekretariat für Migration SEM. https://www.sem.admin.ch/sem/de/home/publiservice/statistik/asylstatistik.html. Accessed 14 Dec 2016
Eritrea|UNAIDS (2015) http://www.unaids.org/en/regionscountries/countries/eritrea. Accessed 2 Dec 2016
Eurostat (2016) Asylum statistics–statistics explained. http://ec.europa.eu/eurostat/statistics-explained/index.php/Asylum_statistics#Asylum_applicants. Accessed 2 Dec 2016
GAHI (2016) Distribution of Schistosomiasis Survey Data in Eritrea| Global Atlas of Helminth Infections. http://www.thiswormyworld.org/maps/distribution-of-schistosomiasis-survey-data-in-eritrea. Accessed 10 Dec 2016
Goldenberger D, Claas DJ, Bloch-Infanger C, Breidthardt T, Suter B, Martínez M, Neumayr A, Blaich A, Egli A, Osthoff M (2015) Louse-Borne relapsing fever (Borrelia recurrentis) in an Eritrean refugee arriving in Switzerland, August 2015. Euro Surveill 20:2–5
Greenaway C, Ma AT, Kloda LA, Klein M, Cnossen S, Schwarzer G, Shrier I (2015) The seroprevalence of hepatitis C antibodies in immigrants and refugees from intermediate and high endemic countries: a systematic review and meta-analysis. PLoS ONE 10:e0141715. doi:10.1371/journal.pone.0141715
Hoch M, Wieser A, Löscher T, Margos G, Pürner F, Zühl J, Seilmaier M et al (2015) Louse-Borne relapsing fever (Borrelia recurrentis) diagnosed in 15 refugees from northeast Africa: epidemiology and preventive control measures, Bavaria, Germany, July to October 2015. Eur Surveill. doi:10.2807/1560-7917.ES.2015.20.42.30046
Jakab Z, Severoni S, Ostlin P, Verschuuren M, Stein CE (2015) Refugee and Migrant health: a priority in the WHO European region. Lancet 386(10012):2477–2478. doi:10.1016/S0140-6736(15)01102-2
Jaton L, Pillonel T, Jaton K, Dory E, Prod’hom G, Blanc DS, issot F, Bodenmann P, Greub G (2016) Common skin infection due to panton–valentine leucocidin-producing Staphylococcus aureus strains in asylum seekers from Eritrea: a genome-based investigation of a suspected outbreak. Clin Microbiol Infect 22:739.e5–739.e8. doi:10.1016/j.cmi.2016.05.026
Kittur N, Castleman JD, Campbell CH, King CH, Colley DG (2016) Comparison of Schistosoma mansoni prevalence and intensity of infection, as determined by the circulating cathodic antigen urine assay or by the Kato-Katz Fecal assay: a systematic review. Am J Trop Med Hyg 94:605–610. doi:10.4269/ajtmh.15-0725
Kopel E, Schwartz E, Amitai Z, Volovik I (2010) Relapsing vivax malaria cluster in Eritrean refugees, Israel, June 2010. Eur Surveill 15(26):2
Lai Y, Biedermann P, Ekpo UF, Garba A, Mathieu E, Midzi N, Mwinzi N et al (2015) Spatial distribution of schistosomiasis and treatment needs in Sub-Saharan Africa: a systematic review and geostatistical analysis. Lancet Infect Dis 15:927–940. doi:10.1016/S1473-3099(15)00066-3
Laub Z (2016) Authoritarianism in Eritrea and the Migrant Crisis. http://www.cfr.org/eritrea/authoritarianism-eritrea-migrant-crisis/p37239. Accessed 12 Dec 2016
Neumayr A (2016) Antiparasitic treatment recommendations—a practical guide to clinical parasitology, 1st edn. Tredition GmbH, Hamburg
Ochodo EA, Gopalakrishna G, Spek B, Reitsma JB, Lieshout L, Zolman K, Lamberton P, Bossuyt PMM, Leeflang MMG (2015) Circulating antigen tests and urine reagent strips for diagnosis of active schistosomiasis in endemic areas. Cochrane Database of Syst Rev 11(3):CD009579. doi:10.1002/14651858.CD009579.pub2
Polman K, Diakhate MM, Engels D, Nahimana S, Van Dam GJ, Ferreira STF, Deelder AM, Gryseels B (2000) Specificity of circulating antigen detection for Schistosomiasis mansoni in Senegal and Burundi. Trop Med Int Health 5:534–537
Rapid Diagnostics (2016) Rapid Medical Siagnostical; POC Casette Based Test. http://rapid-diagnostics.com/contactus.html. Accessed 12 Dec 2016
Robert Koch Institute, Dem RKI (2016) Übermittelte Meldepflichtige Infektionskrankheiten Bei Asylsuchenden in Deutschland—meldepflichtige_Infektionskrankheiten_bei_Asylsuchenden.” https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GesundAZ/Content/A/Asylsuchende/Inhalt/meldepflichtige_Infektionskrankheiten_bei_Asylsuchenden.pdf?__blob=publicationFile
Roggelin L, Tappe D, Noack B, Addo MM, Tannich E, Rothe C (2016) Sharp increase of imported Plasmodium vivax malaria seen in migrants from Eritrea in Hamburg, Germany. Malar J 15:325. doi:10.1186/s12936-016-1366-7
Russo G, Vita S, Miglietta A, Terrazzini N, Sannella A, Vullo V (2016) Health profile and disease determinants among asylum seekers: a cross-sectional retrospective study from an italian reception centre. J Public Health (Oxf) 38:212–222. doi:10.1093/pubmed/fdv049
Saidel-Odes L, Riesenberg K, Schlaeffer F, Smolyakov R, Kafka M, Borer A (2011) Eritrean and Sudanese migrants presenting with malaria in Israel”. Travel Med Infect Dis 9:303–305. doi:10.1016/j.tmaid.2011.09.003
Sonden K, Castro E, Törnnberg L, Stenstrom C, Tegnell A, Farnert A (2014) High incidence of Plasmodium vivax malaria in newly arrived Eritrean refugees in Sweden since May 2014. Eur Surveill 19(35):20890
Theuring S, Friedrich-Jänicke B, Pörtner K, Trebesch I, Durst A, Dieckmann S, Steiner F, Harms G, Mockenhaupt FP (2016) Screening for infectious diseases among unaccompanied minor refugees in Berlin, 2014–2015. Eur J Epidemiol 31:707–710. doi:10.1007/s10654-016-0187-x
Utzinger J, Botero-Kleiven S, Castelli F, Chiodini PL, Edwards H, Köhler N, Gulletta M et al (2010) Microscopic diagnosis of sodium acetate-acetic acid-formalin-fixed stool samples for helminths and intestinal protozoa: a comparison among European reference laboratories. Clin Microbiol Infect 16(3):267–273. doi:10.1111/j.1469-0691.2009.02782.x
van Lieshout L, Polderman LA, Deelder AM (2000) Immunodiagnosis of schistosomiasis by determination of the circulating antigens CAA and CCA, in particular in individuals with recent or light infections. Acta Trop 77:69–80
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics statement
The study protocol was approved by the institutional research commission of the Swiss Tropical and Public Health Institute (Swiss TPH, Basel, Switzerland; reference no. FK 120; approval date: June 24, 2015) and the ethics committee of Northwest and Central Switzerland (reference no. EKNZ 2015-353; approval date: November 20, 2015). Participation was voluntary, and hence, people could withdraw from the study at any time without further obligations. Data were processed anonymously.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Chernet, A., Neumayr, A., Hatz, C. et al. Spectrum of infectious diseases among newly arrived Eritrean refugees in Switzerland: a cross-sectional study. Int J Public Health 63, 233–239 (2018). https://doi.org/10.1007/s00038-017-1034-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-017-1034-x