
Abstract
Objectives
Several public health interventions are not described, not evaluated and not transferred. The objective was to assess the feasibility and acceptability of using a description model making a distinction between interventions’ transferable elements, and those that are more context-specific, to make their evaluation and transferability easier.
Methods
The theoretical distinction between an intervention function and its form in a specific context has been empirically explored. A community-based intervention (named “Ciné-Ma-Santé”) has been described, using a “key function/implementation/context” model. This process has been co-constructed through qualitative research and knowledge exchange process between project leaders and researchers from different disciplines.
Results
The use of the model proves feasible and useful for both project leaders and researchers. Nine key functions were described, as well as their implementation and the features of the intervention context.
Conclusions
Rendering explicit key functions of public health interventions could constitute a useful step to their evaluation and transfer. It enables the formulation of hypotheses regarding the potentially standardizable elements of interventions, and elements that can be modified while maintaining the integrity of the intervention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In addition to their effects on population health outcomes, public health interventions should be evaluated with regard to their capacity to decrease social inequalities in health (SIH) (Whitehead 2007; Woodward and Kawachi 2000). The mechanisms that lead to these inequalities are becoming better understood, yet little is known about the features of public health interventions that are involved in SIH reduction (Delpierre and Kelly-Irving 2011; Lang et al. 2009). Even less is known about how (and whether) the results of these interventions transfer across contexts—a gap that is particularly salient with regard to the inherently complex nature of most SIH-reducing public health interventions.
Many scholars in the field of public and population health intervention research (e.g., Pawson and Tilley 1997; Barnes et al. 2003; Hawe and Potvin 2009; Rychetnik et al. 2002) have argued for the importance of developing new theories and methods that have the capacity to capture and track critical intervention/context interactions, not least so as to demonstrate intervention transferability and scalability across contexts. Yet, approaches to complex intervention evaluation remain dominated by randomized control trials (RCTs). Critics who believe RCTs are an inappropriate approach to assessing complex interventions (Mackenzie et al. 2010) point out that the “black box” conceptualization of interventions implicit in RCTs does not facilitate an in-depth understanding of “what works, for whom and in what circumstances” (Pawson and Tilley 1997). For example, RCTs often fail to demonstrate anticipated effects of complex public health interventions, a fact that is frequently interpreted as intervention failure. Few reports about RCTs of public health interventions specify the mechanisms or pathways that may have resulted in these ‘failures’ (Pearson et al. 2001). While some scientists have adapted RCTs in ways that account for the complexity of interventions (e.g., adaptation to local settings) (Hawe et al. 2004; Bonell et al. 2012), most published studies continue to involve the control of contexts and the standardization of interventions and their implementation—notions that some consider anathema to core values in health promotion and public health (e.g., population participation and consideration of contexts) (WHO 1998). Alternative methods from the field of program evaluation are being developed for evaluating complex public health interventions. Theory-based approaches, such as realist evaluation (Pawson and Tilley 1997), do open the above-mentioned ‘black box’ of interventions. However, these approaches may seem difficult to implement, notably due to a lack of methodological guidance (Marchal et al. 2012). Another type of evaluation theory, called “utilization-focused evaluation” (Patton 1997), does not rely on a specific method but focuses on the needs of evaluation users. The evaluator therefore acts as a negotiator between different stakeholders. Some of the critics of this approach refer to the lack of evaluator objectivity and the risk of manipulation (Patton and LaBossière 2012). However, evaluation cannot be restricted to a technical, rational procedure, but rather constitutes a social and political process in which negotiation is central. Participatory evaluation and research gather researchers and practitioners (Cargo and Mercer 2008) to co-construct knowledge that can be useful for both of them.
In the real world, a lot of interventions are implemented without being “subjected to rigorous scientific development and evaluation” (Evans et al. 2014). However, efficacy does not necessarily start with interventions designed by universities or expert authorities, but can start “with interventions designed or shaped by communities and practitioners” (Hawe and Potvin 2009).
One hypothesis is that to enhance knowledge production based on interventions developed by communities and practitioners, more detailed descriptions of these interventions should be provided, with particular attention paid to their theoretical aspects, as well as their implementation and their context. Real-life intervention descriptions often rely on high-level objectives and a range of detailed activities rather than on theoretical aspects underlying those activities. Moreover, evaluation reports contain little information allowing implementers to decide whether it is possible to adapt an intervention to new specific contexts while remaining true to the original intervention (Michie et al. 2009). Many authors address the question of how to reconcile fidelity to an original, effective intervention with the need to adapt to a new context, building on field practitioners’ skills and expertise (Van Daele et al. 2012). Hawe et al. (2004) proposed an RCT allowing both standardization and adaptation to local contexts. In this model, the “key functions” of an intervention are standardized (e.g., education, empowerment, social support enhancement, etc.), but not its “form” (e.g., concrete activities like a number of workshops or a preset curriculum), resulting from the process of implementing those key functions. Intervention integrity is thus defined in terms of its function rather than in terms of its form: the intervention is adaptive to contexts regarding its concrete activities, but remains true to its theory (Hawe et al. 2009).
Based on a community-based intervention (named Ciné-Ma-Santé), we used the distinction made by Hawe et al. between the key functions and the form of an intervention as an analytical lens through which to describe this intervention, focusing on its potentially transferable elements, while taking implementation context into account. The aim of the study was to assess the feasibility, acceptability and usefulness of the use of this model, to empirically test this theoretical distinction, using a co-construction process between project leaders and researchers.
Context
The AAPRISS program
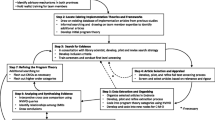
The Ciné-Ma-Santé intervention, which will be described in detail later, is a part of the meta-program AAPRISS, which has been previously described in detail (Lang et al. 2015; Villeval et al. 2015). The AAPRISS program focuses on cancer prevention and health promotion projects in the field of nutrition in the French Midi-Pyrénées region. It aims to analyze the potential impact of these projects on health inequalities, and to co-construct project modifications together with intervention practitioners to reduce or at minimum avoid further increase of SIH. When projects enter the “AAPRISS process”, working groups are set up, bringing together project leaders and researchers from different fields. The aim is to analyze the intervention, propose intervention modifications, and assess those modifications. Five prevention projects have been included in the AAPRISS program on a voluntary basis, including Ciné-Ma-Santé. The key functions and global process of the AAPRISS program are represented in Fig. 1, adapted from Villeval et al. (2015). The position of the present study within this global process appears in red.

Global process and key functions of the “Apprendre et Agir Pour Réduire les Inégalités Sociales de Santé” umbrella program, France, 2011–2015. Adapted from Villeval et al. (2015); reproduced with permission of the Canadian Public Health Association
Ciné-Ma-Santé intervention description
The Ciné-Ma-Santé intervention is part of the “Ateliers Santé Ville” (ASV), a wider community-based program implemented in the northern neighborhoods of the city of Toulouse (Basson et al. 2013). The ASV have been implemented in many other cities in France. They rely on community health values and gather local actors to work on health issues and address SIH in deprived territories. Since 2009, Ciné-Ma-Santé project leaders (i.e., the ASV coordinator, a professional from a local sports association, a public health physician from a child obesity prevention and care association, and local residents) have implemented this intervention once a year, as a half-day event to raise residents’ awareness about nutrition. During this half-day event, several stands are set up in a public park, and health education is provided in schools. The community is offered the opportunity to participate in sports, attend a theater forum, take part in cooking and tasting workshops, etc. At the end of the half day, a movie chosen by residents is shown—hence the name of the intervention. Our hypothesis was, however, that Ciné-Ma-Santé was more than a half-day intervention involving a multiplicity of activities. Rather, this event represents the culmination of the project leaders’ work throughout the whole year.
Methods
A “Key functions/implementation/context” model was developed and tested to describe and analyze the intervention, its implementation, and the context within which it is implemented, to enhance its potential transferability. Once Ciné-Ma-Santé entered the AAPRISS process in 2012, a working group was set up. It involved the Ciné-Ma-Santé project leaders and a group of researchers (a social psychologist, a policy scientist, an epidemiologist, a health promotion methodologist, a public health Ph.D. student, and the AAPRISS project manager). The composition of this working group evolved over time, and three local residents particularly involved in Ciné-Ma-Santé also participated in the last three meetings.
The social psychologist and the policy scientist developed a longitudinal ethnographic approach, focused on the observation of both the Ciné-Ma-Santé half-day itself (30 h of field notes focusing on behaviors, discourses, contexts), and the project leaders’ preparatory and evaluation meetings throughout each year (15 meetings in all). They also observed local residents’ involvement in the preparation, implementation and evaluation of the intervention. In addition, semi-structured interviews were conducted with three project leaders, three local health officials, four association leaders and eight involved residents. All interviews were transcribed and analyzed qualitatively. This inquiry allowed researchers to determine the degree to which and means by which local residents participated and enrolled in the intervention. The people interviewed were chosen according to the following criteria: actual participation in the intervention, commitment relative to its organization and evaluation.
The social psychologist and the policy scientist analyzed the field data and prepared syntheses of the major concepts and themes. Meetings of the AAPRISS working group took place every 3 months, eleven in all over a period of 3 years. During these meetings, the social psychologist and the policy scientist presented their research reports to the project leaders and public health researchers. Based on these analyses and on the project leaders’ experiential and professional knowledge of their intervention, public health researchers undertook the development of the “Key functions/implementation/context” model. Project leaders’ experience was explored with questions such as: “What processes allow the intervention to function?”; “What is the intervention logic underlying implemented activities?”; “What makes this intervention specific?”; “What elements could be modified while following the same logic?”. As a result, the findings presented here reflect a combination of insights gathered and analyzed through university- and community-based lenses. Co-construction between actors from different sectors and disciplines in a knowledge exchange process requires a multiplicity of translations. Knowledge exchange involves the same practitioners and researchers learning from each other throughout the process, and enables common thinking on issues as well as on data production and use (Graham et al. 2006).
This co-construction resulted in the development of a schematic representation showing the combination of transferable key functions and implemented activities. It was refined iteratively until a consensus was reached on this representation of Ciné-Ma-Santé during the meetings of the working group. It enabled Ciné-Ma-Santé to be described in three different ways:
-
1.
Key functions were described. These are defined as essential processes underlying concrete implemented activities, i.e., the functions those activities are meant to have in order to achieve the intervention’s objectives. They were then classified according to M. Whitehead’s typology of program theories for addressing SIH (i.e., strengthening individuals, strengthening communities, improving living and working conditions, promoting healthy macro-policies) (Whitehead 2007). This typology has been used to easily recognize what kind of strategies for reducing health inequalities constitute the intervention represented in the diagram;
-
2.
Significant elements of the context in which the Ciné-Ma-Santé intervention is being implemented were also described, including staff and organizational characteristics, political and social context, and population characteristics (Bauman et al. 1991);
-
3.
The specific form (i.e., concrete activities implemented) of the intervention was also described.
Results
The key functions, context, and implementation of Ciné-Ma-Santé are shown in Fig. 2.

Combination of “Ciné-Ma-Santé” key functions, implementation and context. “Apprendre et Agir Pour Réduire les Inégalités Sociales de Santé umbrella program”, France, 2011–2015
Key functions
Nine key functions were described. They were classified as strengthening individuals or strengthening communities:
-
Key functions 1–4 are strategies aimed at strengthening individuals, i.e., “person-based strategies” (Whitehead 2007).
Key functions 1, 2, and 3 are complementary health education strategies intended for children attending neighborhood schools. Children are both the target of these strategies and a vector for transmission of nutrition messages to their families. Key function 1 consists in “providing knowledge on nutrition through playful activities”, and key function 2 consists in “choosing activities based on pleasure to foster experimentation with taste of food and physical activity”. Project leaders also focused on key function 3: “developing and reinforcing participants’ critical judgment through organization of discussions and debates on nutrition”.
Key function 4 consists in “enhancing the population’s participation at all intervention stages throughout the year (planning, design, implementation, and evaluation)”. This participation process aims to bring together different groups from the neighborhood (residents, professionals from various sectors, local organizations) via the same active movement. It aims to offer people whose role and status in society are not frequently valued the opportunity to be recognized, listened to, and welcomed; and to address communication gaps between individuals, while enhancing meaningful exchanges on nutrition. As project leaders said: “Resident participation is crucial in the intervention logic: they become actors and not just beneficiaries. This participation requires time as well as a lot of upstream work to gain residents’ and partners’ confidence”. This process has evolved over time, and currently, a high level of participation is seen in only a small number of residents, who are not representative of the whole population of interest. As one project leader said during an interview, these residents are “in a dynamic process of participation, they want to participate. They are not here by chance. Anyway, it is hard to reach the residents who do not leave their homes”. However, the empowerment of these residents sets an example for other people living in the neighborhood who are more difficult to reach: “the objective was to involve residents at every stage of the intervention, so that they could transfer this dynamic to other people, by becoming relays”.
-
Key functions 5–9 are strategies for strengthening communities, i.e., strategies to build “social cohesion and mutual support” (Whitehead 2007).
Key functions 5, 6, and 7 are aimed at creating social bonds. Key function 5 consists in “enhancing a cultural and generational mix around nutrition”. Ciné-Ma-Santé leaders combine their various skills to adapt their work to various groups (e.g., in terms of culture and age), who are involved in the intervention to a greater or lesser extent (from residents involved in the intervention management throughout the whole year, to people who just pass through on the day of the event). For the same purpose, key function 6 consists in “choosing a neutral setting for the intervention, so as to foster a mix of populations from different territories”. Choosing a park outside the ASV area in which to run Ciné-Ma-Santé is intended to encourage a mix of people from different neighborhoods. Key function 7 consists in “choosing activities fostering dialogue and collaboration” between all these people.
Key functions 8 and 9 relate to the reinforcement and coordination of a network of partners from institutions and associations. Key function 8 consists in “formalizing a framework of shared values” (e.g., working in partnership, prioritizing community health, external communication and coherent messaging). This framework was developed to strengthen the partnership set up between stakeholders who may have little previous experience working together, to act transversally on different health determinants relating to people’s living environments. As one of the project leaders said, “People participating in this work, in this collective time, need to spend time in the working group where we share objectives, values, ways of working, and need to appropriate what we promote”. The idea is to create a network of partners from ASV territories and other neighborhoods and those working in different sectors. Gathering social work and public health professionals is both the basis and the strength of Ciné-Ma-Santé, as it allows each participant to bring their specific skills to the fore. To foster this collaboration, key function 9 consists in “establishing a mode of coordination based on consensus, co-construction, power-sharing and absence of hierarchical relationship”. This way of working “induces new conceptions of the partnership working on health in the territory: it constitutes a lever to undertake common action, to foster a collective spirit, beyond the intervention itself”, as project leaders said during a working group.
Context
Some elements of the context make the intervention implementation more difficult and could have an adverse influence on its results. Indeed, the context within which the Ciné-Ma-Santé intervention functions is precarious. For instance, it does not have sufficient financial support to cover operating costs. It relies on the collaboration of several other associations, which are themselves precariously funded. As stated by project leaders, the intervention “relies on very unstable resources. […] This causes a major zone of uncertainty around the continuation of the intervention from 1 year to another”.
By contrast, some elements of the context foster the success of the intervention. Indeed, the ASV territory is composed of 7946 residents in six neighborhoods with social difficulties. Drawing on their reflexive attitude toward practice, ASV project leaders have tailored their approach to better meet the ever-changing shifts in the communities’ socio-demographic profiles (e.g., increasing numbers of single-parent families), shifting health profiles (e.g., increasing of levels obesity), and changes in sectors other than health (e.g., rising youth unemployment, disrupted school experiences and school drop-out). The improvement of nutrition is one of the national and regional public health priorities. Their knowledge of local specificities and actors from different fields (social work, sports, health, etc.) allows them to build an actor network and act as translators of these priorities and those of residents and other local actors, creating innovations like Ciné-Ma-Santé. Even if the intervention involves a large variety of stakeholders (sports and social associations, volunteers, residents, health professionals, etc.) who are not necessarily used to working together and usually pursue differing interests, there is now a shared mindset among these stakeholders, who bring to the table their own particular reasons for participating. The group also possesses reflexivity and engages with a deep understanding of local knowledge about the populations and territories in which they have worked for many years.
Implementation
The concrete activities of “Ciné-Ma-Santé” are described in the Fig. 2. The implementation of the intervention key functions through activities is specific to this particular context, and those activities are not transferable to other settings without modification. For instance, Ciné-Ma-Santé Key Function 2 (“Choosing activities based on pleasure to foster experimentation with taste of food and physical activity”) is implemented through a game of rugby, among other activities. In other French regions, where rugby is less popular, this same function could be implemented through other team games.
Discussion
The aim of the study was to assess the feasibility, acceptability and usefulness of using the “key functions/implementation/context” model to describe a community-based intervention.
Model acceptability
At the end of an iterative refinement process, all stakeholders agreed with the representation of the model as presented in Fig. 2. This study draws on principles of participatory research and evaluation (Cargo and Mercer 2008). The intersectorial and interdisciplinary nature of the working group posed the challenge of going beyond professional and disciplinary differences by working on concepts and vocabulary (Villeval et al. 2014), to contemplate the intervention through common frames of reference. Interventional research involving practitioners and researchers entails acknowledging the interests of the various stakeholders and creating a reflective space for debates and negotiations (Bernier 2014). Indeed, knowledge translation between different stakeholders implies the setting of a common ground and the acknowledgment of different realities (Masuda et al. 2014). Finally, based on academic and professional knowledge and thanks to the wealth of exchanges within the working group, the co-construction process resulted in a gain in knowledge for both project leaders and researchers. By describing the key functions and implementation of the Ciné-Ma-Santé intervention, we were able to render explicit certain dimensions that remain implicit in the project leaders’ everyday work. Some key functions were self-evident to them, and thus neither expressed nor highlighted. Indeed, at first they focused more on the description of the intervention form. So at first sight, Ciné-Ma-Santé seems to be a simple event involving a set of activities. The study reveals that behind an apparently simple intervention lie many key functions.
Intervention transferability
Transferability of health promotion interventions raises several questions. Contextualism is indeed one of the “intrinsic features of health promotion” (Potvin and McQueen 2009), and interventions can be considered as “events in systems”, creating and modifying networks of people and activities (Hawe et al. 2009). To some authors, complexity relates more to the context within which the intervention is implemented than to the intervention itself (Shiell et al. 2008). Therefore, an intervention that proves successful somewhere can fail to achieve the same results in another complex context. Transferability goes beyond applicability (the possibility of implementing an intervention process in a new setting) and refers to the possibility of reproducing an intervention’s effects in a new setting (Wang et al. 2006). Transferability is often seen unilaterally, as a way to enhance research use in practice. However, we believe that not only standardized programs and intervention developed by researchers are transferable. Indeed, we adopt a “bottom-up” vision of transferability, based on community-based, non-standardized interventions. This implies working on co-construction between researchers and intervention developers and implementers, to better theorize those interventions and describe the combination of their key functions, implementation and context. In doing so, both innovation and transferability can be enhanced. If an intervention’s key functions are transferred to a new setting, local actors will decide on the form of the replicated intervention according to the specificities of and the knowledge they have about the features of their context. In this way, the interaction between the intervention and its context can have a better chance of producing results. One example of this interaction between an intervention and its context is seen in the Ciné-Ma-Santé key functions 8 and 9: the network of partnerships develops over time and gradually becomes an element of the context supporting perpetuation of the intervention. The recursive effect between intervention and context is indeed one of the features of complex interventions (Lapalme et al. 2013). Greater attention to what constitutes the context of interventions and the processes of interactions between intervention and context is crucial (Shoveller et al. 2015). The development of research aimed at observing similar programs implemented in different contexts would provide better understanding of how health promotion programs interact with different environments, and which contextual elements are crucial or, conversely, prohibitive to their implementation.
Limitations
The major issue faced was the difficulty of making a distinction between intervention function and form. When it comes to replicating a program in another context, some authors highlight the benefit of distinguishing between the “theory of change” (e.g., fostering meetings and relationships between students, parents, and teachers in a casual atmosphere) which refers to the central mechanisms of intervention that have to be faithfully replicated, and the “theory of action” (e.g., a pizza night), which can vary to adapt to different contexts (Funnell and Rogers 2011). However, pizza is an effective means of gathering together adults and adolescents, and another meal could actually modify the intervention logic via its greater or lesser associations with “youth”. Describing key functions requires stakeholders to discuss and negotiate a prioritization of values that will guide the distinction between function and form, and thus the potential transferability of the intervention. A multiplicity of hypotheses has to be formulated, upon which reflection and discussion are always necessary, keeping in mind that the representation of a program is necessarily biased to highlight certain aspects that are specifically interesting to intervention stakeholders (Potvin et al. 2008). Although this diagram made sense for all stakeholders involved in the working group, the content of each category (context, implementation, key functions) can always be questioned.
Evaluating and transferring complex public health interventions raises several questions. Gathering practitioners and researchers and producing not only valid but also useful knowledge is an ongoing challenge for intervention research. Rendering explicit an intervention’s key functions could constitute a useful step in evaluating the intervention’s effects, and enables the formulation of hypotheses regarding potentially transferable elements, as well as those elements that can be modified while maintaining the integrity of the intervention. Although the current study does not answer every question, the development of a “key functions/implementation/context” diagram to enable an intervention’s transferability proves feasible and acceptable for the involved stakeholders, and hence potentially participates in the development of the field.
References
Barnes M, Matka E, Sullivan H (2003) Evidence, understanding and complexity evaluation in non-linear systems. Evaluation 9:265–284
Basson J-C, Haschar-Noé N, Honta M (2013) Toulouse, une «figure urbaine de la santé publique». À propos de l’action publique municipale de lutte contre les inégalités sociales de santé. Rev Épidémiol Santé Publique 61:81–88
Bauman LJ, Stein REK, Ireys HT (1991) Reinventing fidelity: the transfer of social technology among settings. J Community Psychol 19:619–639
Bernier J (2014) La Recherche Partenariale Comme Espace de Soutien à L’innovation. Global Health Promot 21:58–63
Bonell C, Fletcher A, Morton M, Lorenc T, Moore L (2012) Realist randomised controlled trials: a new approach to evaluating complex public health interventions. Soc Sci Med 75:2299–2306
Cargo M, Mercer SL (2008) The value and challenges of participatory research: strengthening its practice. An Rev Public Health 29:325–350
Delpierre C, Kelly-Irving M (2011) To what extent are biological pathways useful when aiming to reduce social inequalities in cancer? Europ J Public Health 21:398–399
Evans R, Scourfield J, Murphy S (2014) Pragmatic, formative process evaluations of complex interventions and why we need more of them. J Epidemiol Community Health. doi:10.1136/jech-2014-204806
Funnell SC, Rogers PJ (2011) Purposeful program theory: effective use of theories of change and logic models. Wiley, New York
Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, Robinson N (2006) Lost in knowledge translation: time for a map? J Contin Educ Health Prof 26:13–24
Hawe P, Potvin L (2009) What is population health intervention research? Can J Public Health 100(1):8–14
Hawe P, Shiell A, Riley T (2004) Complex interventions: how “out of control” can a randomised controlled trial be? BMJ 328:1561–1563
Hawe P, Shiell A, Riley T (2009) Theorising Interventions as events in systems. Am J Community Psychol 43:267–276
Lang T, Kelly-Irving M, Delpierre C (2009) Inequalities in health: from the epidemiologic model towards intervention. Pathways and accumulations along the life course. Rev Epidémiol Santé Publique 57:429–435
Lang T, Bidault E, Villeval M, Alias F, Gandouet B, Servat M, Théis I, Breton E, Haschar-Noé N, Grosclaude P (2015) A health equity impact assessment umbrella program (AAPRISS) to tackle social inequalities in health: program description. Global Health Promot. pii:1757975914568127 (Epub ahead of print)
Lapalme J, Bisset S, Potvin L (2013) Role of context in evaluating neighbourhood interventions promoting positive youth development: a narrative systematic review. Int J Public Health 59:31–42
Mackenzie M, O’Donnell C, Halliday E, Sridharan S, Platt S (2010) Do health improvement programmes fit with MRC guidance on evaluating complex interventions? BMJ (Clin Res Ed.) 340:c185
Marchal B, van Belle S, van Olmen J, Hoerée T, Kegels G (2012) Is realist evaluation keeping its promise? A review of published empirical studies in the field of health systems research. Evaluation 18:192–212
Masuda JR, Zupancic T, Crighton E, Muhajarine N, Phipps E (2014) Equity-focused knowledge translation: a framework for “reasonable action” on health inequities. Int J Public Health 59:457–464
Michie S, Fixsen D, Grimshaw JM, Eccles MP (2009) Specifying and reporting complex behaviour change interventions: the need for a scientific method. Implement Sci 4:40
Patton MQ (1997) Utilization-focused evaluation: the new century text, 3rd edn. Sage, Thousand Oaks
Patton MQ, LaBossière F (2012) L’évaluation axée sur l’utilisation. In: Ridde V, Dagenais C (eds) Approches et pratiques en évaluation de programmes, 2nd edn. Presses de l’Université de Montréal, Montréal, pp 145–160
Pawson R, Tilley N (1997) Realistic evaluation. Sage, London
Pearson TA, Lewis C, Wall S, Jenkins PL, Nafziger A, Weinehall L (2001) Dissecting the “black box” of community intervention: background and rationale. Scand J Public Health 29:5–12
Potvin L, McQueen DD (2009) Practical dilemnas for health promotion evaluation. In: Potvin L, McQueen DD (eds) Health promotion evaluation practices in the Americas—values and research. Springer, New York, pp 25–45
Potvin L, Bilodeau A, Gendron S (2008) Trois Défis Pour L’évaluation En Promotion de La Santé. Promot Educ 15:17–21
Rychetnik L, Frommer M, Hawe P, Shiell A (2002) Criteria for evaluating evidence on public health interventions. J Epidemiol Community Health 56:119–127
Shiell A, Hawe P, Gold L (2008) Complex interventions or complex systems? Implications for health economic evaluation. BMJ 336:1281–1283
Shoveller J, Viehbeck S, Di Ruggiero E, Greyson D, Thomson K, Knight R (2015) A critical examination of representations of context within research on population health interventions. Crit Public Health. doi:10.1080/09581596.2015.1117577
Van Daele T, Van Audenhove C, Hermans D, Van Den Bergh O, Van Den Broucke S (2012) Empowerment implementation: enhancing fidelity and adaptation in a psycho-educational intervention. Health Promot Int 29:212–222
Villeval M, Ginsbourger T, Bidault E, Alias F, Delpierre C, Gaborit E, Kelly-Irving M, Manuello P, Grosclaude P, Lang T (2014) L’interdisciplinarité en action: les «mots-pièges» d’une recherche interdisciplinaire. Santé Publique 26:155–163
Villeval M, Bidault E, Gaborit E, Grosclaude P, Haschar-Noé N, Lang T (2015) Un programme de recherche interventionnelle (AAPRISS) visant à réduire les inégalités sociales de santé: méthodes et validation. Can J Public Health 106:e434–e441
Wang S, Moss JR, Hiller JE (2006) Applicability and transferability of interventions in evidence-based public health. Health Promot Int 21:76–83
Whitehead M (2007) A typology of actions to tackle social inequalities in health. J Epidemiol Community Health 61:473–478
WHO (1998) Health promotion evaluation: recommendation to policy-makers. Report of the WHO European Working Group on Health Promotion Evaluation. World Health Organisation Europe, Copenhagen. doi:10.1111/j.1365-2214.2004.00453.x/full
Woodward A, Kawachi I (2000) Why reduce health inequalities? J Epidemiol Community Health 54:923–929
Acknowledgments
This work was supported by the Institut National du Cancer (INCA N° 2011-009), the Agence Nationale de la Recherche (ANR-11-INEG-0003 “EVALISS”), the Agence Régionale de Santé Midi-Pyrénées (ARS), and the Fondation ARC pour la recherche sur le cancer for the PhD student MV (File n°DOC20140601025). We would like to thank the AAPRISS Scientific Committee: Franco Berrino, Pierre Blaise, Pierre Chauvin, Hercberg Serge, France Lert, Louise Potvin, and Alfred Spira.
The AAPRISS group: B Almudever, L Birelichie, E Breton, A Bulle, F Cayla, C Delpierre, P Ducournau, E Gaborit, B Gandouet, T Ginsbourger, E Godeau, A Guichard, N Haschar-Noé, M Kelly-Irving, A Lacouture, C Martin, A Mayère, P Manuello, I Poirot-Mazère, E Salaméro, M Servat, F Sicot, F Sordes-Ader, I Theis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
For the AAPRISS group see “Acknowledgments”.
Rights and permissions
About this article

Cite this article
Villeval, M., Bidault, E., Shoveller, J. et al. Enabling the transferability of complex interventions: exploring the combination of an intervention’s key functions and implementation. Int J Public Health 61, 1031–1038 (2016). https://doi.org/10.1007/s00038-016-0809-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-016-0809-9