
Abstract
Objectives
To analyze the association between physical inactivity in different domains and direct public healthcare expenditures in adults and to identify whether the clustering of physical inactivity in different domains would contribute to increased public healthcare.
Methods
The sample composed of 963 adults randomly selected in a middle-size Brazilian city. Annual healthcare expenditure was estimated including all items registered in the medical records in the last 12 months prior to the interview. Habitual physical activity was estimated using Baecke questionnaire, which considers three components of physical activity (work, sports and leisure-time activities).
Results
Higher healthcare expenditures of medicines were associated with lower physical activity at work (OR 1.58 [1.06–2.35]), sport (OR 1.57 [1.12–2.18]) and physical inactivity in three domains (OR 2.12 [1.18–3.78]). Expenditures related to medicine (r = 0.109 [95 % CI 0.046–0.171]) and overall expenditures (r = 0.092 [95 % CI 0.029–0.155]) were related to physical inactivity, independently of age, sex, smoking, blood pressure and obesity.
Conclusions
Physically inactive subjects in different domains of physical activity have increased likelihood to be inserted at groups of higher healthcare expenditure.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
There is a high prevalence of physical inactivity among adults worldwide (Fernandes and Zanesco 2010; Imbeault et al. 2013). This is a great concern because physical inactivity is a relevant risk factor related to chronic diseases and early mortality (Admiraal et al. 2011; Arsenault et al. 2010; Beunza et al. 2007; WHO 2006). Parallel to this there is increasing literature, identifying that chronic diseases have a significant burden over health care costs in both developed and developing countries (Arredondo et al. 2005; Bahia et al. 2012; Hogan et al. 2003). Chronic diseases have been associated to higher expenditures and health care services, specially related to diabetes. In Mexican health system, the increase in health care costs associated with chronic diseases has been higher than expected in a period of 2 years (Arredondo et al. 2005). In Brazil, in a recent study (Bahia et al. 2012) estimated the total yearly costs with all the diseases related to overweight and obesity around US$ 2.1 billion, which represents approximately 10 % of entire outpatient costs. In the United States of America, Hogan et al. (2003) found that the direct and indirect costs related to medicines for diabetes control expenditures were US$ 132 billion.
With this in mind, strategies to combat this increasing demand on public health expenditures have been formulated and, in turn, the promotion of physical activity (PA) has been pointed out as relevant investment in the mitigation of health care expenditures (Davis et al. 2014); mainly because higher habitual PA has been linked to lower medicine use and health care costs, even in people with chronic diseases (Bertoldi et al. 2006; Codogno et al. 2011). On the other hand, recent document identified that there are methodological challenges to be overcome, such as difficult in the assessment of the outcomes (in this case, health care expenditures) (Davis et al. 2014).
Moreover, PA is a behavioral variable, which is manifested in different settings (e.g. occupational activity, sporting activities and leisure-time activity) (Mann et al. 2013; de Sa et al. 2014) and these components seem to be independent of each other (Christofaro et al. 2013; Fernandes et al. 2008). Abu-Omar and Rütten (2008) identified that PA performed in different components can affect differently related-health variables, but the actual burden of the PA performed in different components over health care costs is still unclear. Probably, the main difficulties on the assessment of strategies targeting promotion of PA (Davis et al. 2014) are related to specific characteristics, like adequate definition of terms.
Therefore, the aims of this study were (1) to analyze the association between physical inactivity in different components and direct public health care expenditures in adults and, (2) to identify whether the clustering of physical inactivity in different components would contribute to increased public health care expenditures independently of obesity, aging, smoking and blood pressure.
Methods
Sample and sampling
This cross-sectional study with retrospective design was carried out in the city of Bauru (central region of São Paulo State and ~300,000 inhabitants), Brazil. Prior to implementation, the study was approved by the Ethics Committee Group from Universidade Estadual Paulista—UNESP (Bauru campus) (Protocol number 1046/46/01/10) and all subjects signed a standard written consent form.
The sample size was composed of adults over 50-year-old (age range associated with development of chronic diseases) of both sexes, randomly selected in five Basic Health care Units (BHU); each one located in a different region of the city (north, south, east, west and center regions). In Brazil, BHU constitutes a primary health care center, which hosts a wide variety of health professionals (e.g. general practitioner, gynecologist, obstetrician, psychiatry, dentistry and nursing) and offers health services to the population of a specific region of the city (Codogno et al. 2011). BHU are administered by local municipality government (buy of medical devices/products and payment of health professional staff), which receives resources by the federal government.
The patients attended in a specific BHU have a permanent clinical record in this BHU, in which all medical service related to the patient are obligatorily registered. The main activities of a BHU are related to preventive/palliative actions (e.g. medical consultations, exams’ schedule [performed in hospitals and clinical laboratories outside the BHU], medicine delivery [mainly related to the treatment of chronic diseases] and vaccination) and more complex cases (e.g. surgeries, bone fractures and victims of car accidents) are directed to hospital centers.
Sample size was estimated based on the percentage of Brazilian population that is attended exclusively by the Brazilian public health care system (60 %) (Kilsztajn et al. 2003) and using as parameters a 3.8 % error (arbitrary because there are no other similar studies), 5 % significance (z = 1.96) and design effect of 50 % (using cluster sampling including BHU), reaching a final sample size of at least 958 participants (minimum of 192 in each BHU). After fieldwork, carried out during 2010, the final sample was composed of 963 adults of both genders. In this study, three researchers performed all measurements and, of these, just two researchers, with previous experience in this kind of research, performed the assessment of the annual health care expenditures of the patients.
Annual health care expenditures
There is absence of widely accepted methodologies to estimate health care expenditures and the lack of communication between local municipality and federal government becomes hard to estimate accurately the expenditures. Therefore, the adopted methodology to assessment of annual health care expenditures was according to descripted by Codogno et al. (2011). Briefly, after permission of the local municipality health secretariat, BHU offices provided standard tables related to the reimbursement of the services and health professionals staff. For example, the amount of money paid by a specific medication was divided by the dosage of the medication delivered to the patient, as well it was computed the amount of money paid by the medical consultation, in which the health professional prescribed the medicine. The adopted methodology provides the exact amount of money paid by the federal government with each patient. Finally, the health care expenditures were divided into: medication dispensed, laboratory tests performed, medical consultations and overall expenditures.
Annual health care expenditure of each subject was estimated including all items registered in the medical records in the last 12 months prior to the interview conducted in this study. After that, all expenditures were computed in the Brazilian currency (Real) and converted to US dollar using the average value of the dollar against the Brazilian currency in the 12 months of 2009 (Codogno et al. 2011). Additionally, inflation observed in the Brazilian economy during 2011 (6.50 %), 2012 (5.84 %) and 2013 (5.91 %) were used to adjust the monetary values.
For statistical procedures involving categorical data, overall and specific indicators of expenditures were ranked and stratified into quartiles and the highest quartile of expenditures (≥P75) was adopted as dependent variable.
Components of physical activity
Habitual PA can be divided into three different components such as work, sport practice and leisure-time. The questionnaire developed by Baecke et al. (1982) is composed of 16 questions scored on a 5-points Likert scale ranging from never to always/very often. The PA level is calculated by specific equations and is expressed as scores for each PA component (higher score denotes higher PA). The sample was divided into quartiles according to the PA score and participants were classified as followed: bottom quartile (≤P25), middle quartiles (≥P25 and ≤P75) or high quartile (≥P75) within each component of PA (work, sports practice and leisure-time). After that, it was analyzed in how many components of PA the participant was inserted in the bottom quartile (≤P25), ranging from none (presence in none of the bottom quartiles of the PA components) to three (presence in the bottom quartile of the three components).
Structured interview, anthropometry and blood pressure
A structured face-to-face interview and anthropometric measures were carried out by three trained researcher at the BHU. In this moment of assessment, some variables potentially related to the health care expenditures in Brazilian population were analyzed and treated as potential confounders in this study.
The following data were obtained through interviews and confirmed in medical records: (1) socio-demographic variables (sex, chronological age [structured as categorical variable: <65 year-old and ≥65 year-old]); (2) smoking habits (categorized as “yes” [current smokers independently of number of cigarettes per day] and “no”: former smokers or never smoked; (3) formal education and economic status were assessed by a specific and previously validated Brazilian questionnaire (ABEP 2010), which estimates the family income and includes the level of formal education.
Through anthropometry measurements, body mass index (BMI) was calculated using measurements of weight (digital scale with maximum weight of 150 kg) and height (wall mounted stadiometer with maximum height of 2 m) (Lohman et al. 1988) and obtained dividing weight by squared height (kg/m2). In this study, obesity was defined as BMI ≥30 kg/m2.
The measurements of systolic (SBP) and diastolic (DBP) blood pressure at rest (seat position per at least 10 min) were performed according to protocol of the VI Brazilian Guidelines of Hypertension (2010) and using auscultatory method (only two previously trained researchers performed the blood pressure measurements).
Statistical procedures
Numerical variables of health care expenditures had non-parametric distributions and thus these variables were analyzed under logarithm transformation. Analysis of covariance (ANCOVA) compared economic variables according to physical inactivity, controlled by sex (categorical), age (numerical), blood pressure (numerical), BMI (numerical) and smoking (categorical). For this specific analysis, descriptive statistic was composed by estimated mean and 95 % confidence interval (95 % CI) provided by ANCOVA. Bonferroni post hoc test was applied when necessary and measures of effect size were provided by eta-square (ES-r) values. Kruskal–Wallis’s test compared numerical variables with non-parametric distributions and, when necessary, Mann–Whitney’s was applied as post hoc test. Bivariate and partial (controlled by sex, age, blood pressure, BMI and smoking) correlations were calculated, using Pearson’s correlation. Categorical variables were presented as rates and Chi square test analyzed the association between economic outcomes and independent variables. Binary logistic regression was used to estimate the magnitude of the association between cluster of physical inactivity and economic variables (expressed as odds ratio [OR] and 95 % confidence intervals [95 %CI]). The Hosmer and Lemeshow’s test was used to describe how fit were the multivariate models (p value >0.05 denotes an adequately fit model). Statistical significance was set at a p value <0.05 and the software BioEstat (version 5.0) performed all analyzes.
Results
Overall sample was composed mainly of women and 707 (73.4 %) and 45 % (n = 433) of the subjects presented were ≥65-year-old. Regarding components of PA, 6.5 % of the sample (n = 63) were in the lowest quartile simultaneously in three components, while 12.1 % (n = 117) and 30.2 % (n = 291) of the sample were in two and one component, respectively. There was a significant association between higher age (≥65 year-old [p value = 0.001]), arterial hypertension (p value = 0.004) and higher number of sedentary PA components (Table 1).
Higher health care expenditures of medicines were positively associated with lower PA at work (p value = 0.029), sport (p value = 0.022) and clustering of components of PA (p value = 0.003). In the same way, higher overall health care expenditures were associated with lower PA at leisure-time (p value = 0.021) and clustering of components of PA (p value = 0.017) (Table 2).
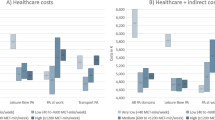
In the multivariate model, independently of other potential confounders (Fig. 1, panels a and b), lower PA at work (OR 1.58 [1.06–2.35]) and sport (OR 1.57 [1.12–2.18]) remain still associated with higher health care expenditures related to medicines discharge. Similarly, lower physical activities in two (OR 1.75 [1.09–2.82]) and three (OR 2.12 [1.18–3.78]) components were still associated with higher expenditures too. Overall expenditures were still associated with lower physical at leisure-time (OR 1.53 [1.08–2.15]), likewise, only subjects with lower PA in all components had higher overall expenditures (OR 2.28 [1.27–4.11]).

Multivariate associations between physical activity components and highest health care expenditures in adults (Brazil, 2010 [n = 963]). OR odds ratio, 95 % CI 95 % confidence interval; Model adjusted by sex, age, formal education, smoking habit, basic healthcare unit, body mass index, systolic and diastolic blood pressure; All adjusted models presented non-significant p value for Hosmer–Lemeshow’s test (work × medicines p value = 0.806; sport × medicines p value = 0.692; clustering × overall p value = 0.542), except the model Leisure-time × Overall (p value = 0.011)
ANCOVA identified that, after control by sex, age, blood pressure, BMI and smoking, the number of physically inactive components explained little, but significant variance in the outcomes (small effect size for both: 1.0 % to medicine and 0.7 % to overall expenditures). Moreover, expenditures related to medicine (r = 0.077 [95 % CI 0.014–0.139]) and overall expenditures (r = 0.067 [95 % CI 0.004–0.130]) were related to physical inactivity, independently of control of the above mentioned variables (Table 3).
Complementally, by analyzing the relationship between different components of PA it was found that the leisure-time component was related with sport (ρ = 0.28; p value = 0.001) and work (ρ = 0.14; p value = 0.001), while work and sport did were not (ρ = −0.03; p value = 0.266). Finally, overall PA score (sum of the PA scores of all three components) was significantly and negatively related to overall expenditures (r = −0.127 [95 % CI −0.189 to −0.064]).
Discussion
The present study found association between higher health care expenditure and physically inactive behavior in different components of PA among adults; and this leads to believe that accumulation of sedentary lifestyle in different PA components increases the risk of presenting higher expenditures.
In this study, physical inactivity was responsible by approximately 1 % of the variance observed in overall expenditures. Katzmarzyk et al. (2000) identified that in 1999 approximately 2.5 % of all health care costs in Canada were attributed to physical inactivity. Our findings are similar to previous data reporting that 1–4 % of the total health care costs related can be attributed to physical inactivity (Davis et al. 2014). Therefore, regarding to health care costs, reducing physical inactivity would be a relevant action on the mitigation of primary health care expenditures. These data are particularly relevant because if primary health care is effective, there is cost saving in the secondary and tertiary health care (Saha et al. 2013).
Another noteworthy finding in our study was the more relevant effect of the physical inactivity in the expenditures related to medicine. Recent literature has shown an association between overall PA level and lower health care expenditure (Bertoldi, Hallal and Barros 2006; Codogno et al. 2011) especially from medication (Codogno et al. 2011). However, the impact of physical activity in different components of PA on health care expenditures is unclear. According to these findings, to analyze the long-term impact of a corporate health and wellness program on health utilization and expenditures among employees of a big company, an USA study indicated a large reduction in medical care expenditure over the 4-year program period (approximately $224.66 per employee per year). These benefits came from reduced inpatient use, fewer mental health visits, and fewer outpatient visits compared with the baseline period, showing that benefits may have substantial health and economic benefits in later years (Ozminkowski et al. 2002). However, despite the importance of pronounced relationships of different components of PA to health indicators, research evolving to economic impact of these interactions is up till now not published.
The initial hypothesis of our study to explain the relationship between physical inactivity and increased expenditures was based in its positive relation with body adiposity. Other research shows that men engaged in either sport activities or walking during leisure-time have lower prevalence of obesity. Moreover, increased sedentary behavior during leisure-time (watching TV) is associated with obesity also (Fernandes et al. 2010). In fact, in the analyzed dataset, the ANCOVA measures identified that BMI was responsible by 3.6 % and 2.5 % of the variance in medicine and overall expenditures, but this effect size was independent of the physical inactivity (which was significantly too). These findings identify that PA promotion could affect health care expenditures by its effect in weight loss (e.g. through effect in inflammatory variables without weight loss) (Balducci et al. 2010; Lima et al. 2014) and, therefore, the expenditures saving could be higher in patients who become physically active and experienced weight loss (Williams et al. 2014).
Another result that requires attention is the significant relationship between the different components of PA. It was found that practice of PA in leisure-time was associated with work and sport activities. Thus, although some components may be independent of each other especially among adolescents (Fernandes et al. 2008), these results indicate that being physically active in the leisure-time components can affect activity in other areas and, therefore, overall PA would be increased in other components too. In fact, higher leisure-time PA is positively associated with better self-rated health (Abu-Omar and Rütten 2008) and, therefore, physically active people would be more motivated to engage in other non-sedentary activities, as well less likely to visit doctor (Kolbe-Alexander, Conradie and Lambert 2013). Moreover, effectiveness of the promotion of physical exercise in cost saving in primary health care setting is usually measured through measures of the burden of the disease in the life of the patient (e.g. quality-adjusted life-year), an outcome strictly related to perception of quality of life (Saha et al. 2013).
This study has strengths, such as the random selection of the sample and the quality in the measurement of the direct health care expenditures. On the other hand, limitations should be considered too. Even with plausible biological pathways to support our findings, the cross-sectional study does not allow conclude about causality. In fact, a cohort study has been conducted with this sample and, in the future, it will be possible ratify or not our findings in a longitudinal design. Our estimation could have been be underestimated, because this study analyzed only direct expenditures related to patient treatment/attendance and was not computed the money paid in the maintenance of the BHU facility (e.g. water services, electric energy and cleaning services). Finally, economic losses related to absenteeism and hospitalizations were not computed because and, thus, should be considered in future studies.
In conclusion, physically inactive subjects in different components of PA have increased likelihood to be inserted at groups of higher health care expenditure. Increase of PA in different components of PA seems to be effective in the mitigation of health care expenditures even without weight loss.
References
Abu-Omar K, Rütten A (2008) Relation of leisure time, occupational, domestic, and commuting physical activity to health indicators in Europe. Prev Med 47:319–323. doi:10.1016/j.ypmed.2008.03.012
Admiraal WM, van Valkengoed IG, L de Munter JS, et al (2011) The association of physical inactivity with Type 2 diabetes among different ethnic groups. Diabet Med 28:668–72. doi:10.1111/j.1464-5491.2011.03248.x
Arredondo A, Zuñiga A, Parada I (2005) Health care costs and financial consequences of epidemiological changes in chronic diseases in Latin America: evidence from Mexico. Public Health 119:711–720. doi:10.1016/j.puhe.2005.01.009
Arsenault BJ, Rana JS, Lemieux I et al (2010) Physical inactivity, abdominal obesity and risk of coronary heart disease in apparently healthy men and women. Int J Obes (Lond) 34:340–347. doi:10.1038/ijo.2009.229
Associação Brasileira de Empresas de Pesquisa (ABEP) (2010) Dados com base no Levantamento Sócio Econômico 2008—IBOPE. Disponible: www.abep.com.br. Accessed 10 March 2014
Baecke JAH, Burema J, Frijters JER (1982) A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36:936–942
Bahia L, Coutinho ES, Barufaldi LA et al (2012) The costs of overweight and obesity-related diseases in the Brazilan public health system: cross-sectional study. BMC Public Health 12:440. doi:10.1186/1471-2458-12-440
Balducci S, Zanuso S, Nicolucci A et al (2010) Anti-inflammatory effect of exercise training in subjects with type 2 diabetes and the metabolic syndrome is dependent on exercise modalities and independent of weight loss. Nutr Metab Cardiovasc Dis 20:608–617. doi:10.1016/j.numecd.2009.04.015
Bertoldi AD, Hallal PC, Barros AJD (2006) Physical activity and medicine use: evidence from a population-based study. BMC Public Health 6:224. doi:10.1186/1471-2458-6-224
Beunza JJ, Martínez-González MA, Ebrahim S et al (2007) Sedentary behaviors and the risk of incident hypertension: the SUN Cohort. Am J Hypertens 20:1156–1162. doi:10.1016/j.amjhyper.2007.06.007
Brazilian Society of Hypertension (2010) VI Diretriz Brasileira de Hipertensão Arterial. Rev Bras Hipertens 17:4
Christofaro DG, Ritti-Dias RM, Chiolero A et al (2013) Physical activity is inversely associated with high blood pressure independently of overweight in Brazilian adolescents. Scand J Med Sci Sports 23:317–322. doi:10.1111/j.1600-0838.2011.01382.x
Codogno JS, Fernandes RA, Sarti FM et al (2011) The burden of physical activity on type 2 diabetes public health care expenditures among adults: a retrospective study. BMC Public Health 11:275. doi:10.1186/1471-2458-11-275
Davis JC, Verhagen E, Bryan S et al (2014) Consensus Statement from the first Economics of Physical Inactivity Consensus (EPIC) Conference (Vancouver). Br J Sports Med 48:947–951. doi:10.1136/bjsports-2014-093575
de Sa TH, Garcia LM, Claro RM (2014) Frequency, distribution and time trends of types of leisure-time physical activity in Brazil, 2006-2012. Int J Public Health 59:975–982. doi:10.1007/s00038-014-0590-6
Fernandes RA, Zanesco A (2010) Early physical activity promotes lower prevalence of chronic diseases in adulthood. Hypertens Res 33:926–931. doi:10.1038/hr.2010.106
Fernandes RA, Freitas Junior IF, Cardoso JR et al (2008) Association between regular participation in sports and leisure time behaviors in Brazilian adolescents: a cross-sectional study. BMC Public Health 8:329. doi:10.1186/1471-2458-8-329
Fernandes RA, Christofaro DG, Casonato J et al (2010) Leisure time behaviors: prevalence, correlates and associations with overweight in Brazilian adults. A cross-sectional analysis. Rev Med Chil 138:29–35. doi:10.4067/S0034-98872010000100004
Hogan P, Dall T, Nikolov P (2003) Economic costs of diabetes in the US in 2002. Diabetes Care 26:917–932. doi:10.2337/diacare.26.3.917
Imbeault P, Makvandi E, Batal M et al (2013) Physical inactivity among francophones and anglophones in Canada. Can J Public Health 104:S26–S30
Katzmarzyk PT, Gledhill N, Shephard RJ (2000) The economic burden of physical inactivity in Canada. CMAJ 163:1435–1440
Kilsztajn S, Rossbach A, Câmara MB et al (2003) Serviços de saúde, gastos e envelhecimento da população brasileira. Rev Bras Estud Popul 20:93–108
Kolbe-Alexander TL, Conradie J, Lambert EV (2013) Clustering of risk factors for non-communicable disease and healthcare expenditure in employees with private health insurance presenting for health risk appraisal: a cross-sectional study. BMC Public Health 21(13):1213. doi:10.1186/1471-2458-13-1213
Lima MC, Barbosa MF, Diniz TA et al (2014) Early and current physical activity: relationship with intima-media thickness and metabolic variables in adulthood. Braz J Phys Ther 18:462–469
Lohman TG, Roche AF, Mertorell R (1988) Anthropometric Standardization Reference Manual. IHuman Kinectics Books, Champaign
Mann KD, Hayes L, Basterfield L et al (2013) Differing lifecourse associations with sport-, occupational- and household-based physical activity at age 49–51 years: the Newcastle thousand families study. Int J Public Health 58:79–88
Ozminkowski RJ, Ling D, Goetzel RZ et al (2002) Long-term impact of Johnson & Johnson’s Health & Wellness Program on health care utilization and expenditures. J Occup Environ Med 44:21–29
Saha S, Carlsson KS, Gerdtham UG et al (2013) Are lifestyle interventions in primary care cost-effective?–An analysis based on a Markov model, differences-in-differences approach and the Swedish Björknäs study. PLoS One 8:e80672. doi:10.1371/journal.pone.0080672
Williams ED, Eastwood SV, Tillin T et al (2014) The effects of weight and physical activity change over 20 years on later-life objective and self-reported disability. Int J Epidemiol 43:856–865. doi:10.1093/ije/dyu013
World Health Organization. Promoting physical activity for health—a framework for action in the WHO European region. Steps toward a more physically active Europe. Regional office for Europe, 2006 [consulted 2014 April 06]. Available at: http://www.euro.who.int/Document/NUT/Instanbul_conf_edoc10.pdf
Acknowledgments
The development of this work was partially supported by Brazilian Government through a PhD scholarship from CAPES and by the Brazilian Ministry of Science and Technology (CNPq) Projects no: 457448/2013-0, Project no: 401178/2013-7 and Project no: 476244/2013-7.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Codogno, J.S., Turi, B.C., Kemper, H.C.G. et al. Physical inactivity of adults and 1-year health care expenditures in Brazil. Int J Public Health 60, 309–316 (2015). https://doi.org/10.1007/s00038-015-0657-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-015-0657-z