
Abstract
Objectives
Although the past two decades have involved changes in the living conditions of the oldest old in Sweden, little is known about how health inequalities have developed in this group during the period. This study explores the educational disparities in a wide range of health outcomes among the oldest old in Sweden between 1992 and 2011.
Methods
The study uses the repeated cross-sectional design of the SWEOLD survey, a nationally representative survey of the oldest old in Sweden with comparable data from 1992, 2002, and 2011. The development of educational disparities in health was tracked across the three waves.
Results
The results show that although the prevalence of most health problems increased during the period, the prevalence of disability in activities of daily living decreased. Despite these changes, educational disparities in health remained largely unaffected.
Conclusions
The results of the study suggest that the association between education and health is remarkably robust. It prevailed into the oldest age groups, was consistently found for a wide range of health problems, and tended to be stable over extended periods of time.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
It is now well known that socioeconomic inequalities in health prevail into old age. In studies of socioeconomic inequalities in health during old age, socioeconomic position is commonly assessed by income, social class (e.g., based on last occupation or main lifetime occupation), or education (e.g., years of education or highest attained educational level).The results tend to show that older adults who have worked in manual occupations, have little education, or have low incomes are more likely to experience health problems and die at younger ages than older adults who have worked in non-manual occupations, have more education, or have higher incomes (Kibele 2014; Knesebeck et al. 2003; Leopold and Engelhartdt 2013; Ploubidis et al. 2013). However, less is known about how these inequalities have developed over time (Fors et al. 2008; Freedman et al. 2002). The few studies that have explored trends in health inequalities among older adults over time, conducted in societies that differ substantially in terms of social and economic conditions, have revealed diverging patterns.
A review of trends in disability and functioning among older adults in the United States during the 1980s and the 1990s suggested mixed results regarding trends in disability and functioning by educational level. However, some of the results suggest that the relative gap in the prevalence of disability between different educational groups increased between 1982 and 1996 (Freedman et al. 2002; Schoeni et al. 2001). In another US study on older adults (70+ years), the researchers found that the relative socioeconomic inequalities in disability increased between 1982 and 2002 (Schoeni et al. 2005).
Similarly, a study of older adults (aged 65+ years) in England between 1992 and 2007 showed that although the prevalence of impaired mobility and physical functioning decreased among all educational groups and occupational groups, the decrease was smallest among those with less education and those with a history as manual workers. However, the prevalence of other indicators of health remained stable over time in all socioeconomic groups (Martin et al. 2012).
Additionally, Dutch researchers found evidence of increasing relative inequalities in the prevalence of disabilities among older women (aged 55–65 years) by educational level in the Netherlands between 1992 and 2002. Among men, on the other hand, the relative inequalities in disabilities by educational level remained stable over the period (Hoogendijk et al. 2008).
Evidence suggests that the inequalities in health among older adults in the Nordic countries have been stable, at least during the 1990s. In studies of adults aged 65–84 years in Finland, researchers found that the relative educational inequalities in health and disability did not change significantly between 1993 and 2003 (Sulander et al. 2006, 2009).
We have previously shown substantial socioeconomic inequalities in health and functioning among older adults in Sweden (Fors et al. 2008, 2009, 2012, 2013a; Thorslund and Lundberg 1994). Moreover, an earlier study of trends in relative health inequalities among adults aged 55+ years in Sweden between 1992 and 2002 did not find any changes in the association between occupational groups and health during the period (Fors et al. 2008).
The aim of this study is to explore the trends in educational inequalities in health among adults aged 77+ years in Sweden from 1992 to 2011. Health problems are assessed in terms of suboptimal self-rated health, musculoskeletal pain, psychological distress, impaired mobility, problems with activities of daily living (ADL), impaired physical function, and lung function (peak expiratory flow rate).
At this point, little is known about whether health inequalities among the oldest old in Sweden have changed in recent decades. Yet, developments have occurred during this period that could impact the association between education and health among the oldest old.
Some of these developments might increase health inequalities in the older population. While income inequalities among those aged 65 and older decreased between 1995 and 2007 in several European countries (van Vliet et al. 2012), older adults in Sweden have experienced increasing income inequalities. Between 1991 and 2004, income inequality, as measured by Gini coefficients for equivalent disposable income, increased from 0.18 to 0.23 among those aged 75 years or older in Sweden (Gustafsson et al. 2009).
Moreover, as observed in several countries, the rates of survival to old age and during old age increased during the period (Christensen et al. 2009; Statistics Sweden 2013). It has been suggested that this development is, partly, driven by increased survival among people with health problems (Rosén and Haglund 2005). As poor health is more common among those with lower education (Mirowsky and Ross 2003), this development could mean that more unhealthy people with lower education now survive to older ages. This, in turn, could cause increasing health inequalities in old age.
On the other hand, other developments might be accompanied by decreasing health inequalities in the older population. In line with the development observed in several European countries (van Vliet et al. 2012), the proportion of adults aged 65+ years living in poverty in Sweden decreased during the period. This pattern was found for relative poverty (defined as having an income less than 60 % of the median income in the population) and for absolute poverty (as defined by the Swedish National Board of Health and Welfare) (Gustafsson et al. 2009).
Additionally, in line with the development observed in several other countries, the proportion of older adults with higher education increased in Sweden during the period. In 1992, about a quarter of those aged 77+ years had an education beyond grade school. In 2011, the corresponding proportion was 42 % (see Table 1). So, although education beyond grade school was previously a privilege reserved for a selected group, it has become more common. It is thus reasonable to assume that the group with more education than grade school has become less selected, at least in terms of social background. This development may, in turn, mitigate the health inequalities between the educational groups.
A previous study using the same data as this study showed that the prevalence of several health problems either increased or remained stable between 1992 and 2011. Yet, the proportion of older adults who reported problems with their ADL shrank significantly (Fors et al. 2013b). Similarly, decreasing prevalences of ADL disability in old age have been observed in Denmark, Japan, and Finland during the period (Christensen et al. 2013; Schoeni et al. 2006; Sulander et al. 2006). The evidence from the US, on the other hand, is ambiguous, a systematic review showed conflicting evidence for the period spanning the late 1980s and 1990s (Freedman et al. 2002). The extent to which these changes in prevalence rates have been accompanied by changes in the patterns of socioeconomic health inequalities is as yet unknown.
Methods
Data
The study used data from the Longitudinal Study of the Living Conditions of the Oldest Old (SWEOLD) from 1992, 2002, and 2011. SWEOLD is a nationally representative survey of the oldest old (77+ years) in Sweden (Lennartsson et al. 2014). The study sample includes those who have previously been included in the study sample of the Swedish Level of Living Survey (LNU), a nationally representative survey of Swedish adults, but who were too old (i.e., older than 75) at the last wave of interviews. As the first wave of SWEOLD (1992) was conducted 1 year after an LNU wave, the lower age limit of SWEOLD became 77. While the data have longitudinal properties, this study is entirely based on cross-sectional analyses of the three waves. In the 2011 survey, an extra sample of individuals randomly selected from the Swedish population was added in the oldest age groups (85+ years). This oversampling and an underrepresentation of 77-year olds in the 1992 survey were adjusted by weighting. The response rates for the three surveys were 90.4 % (1992), 84.4 % (2002), and 86.2 % (2011).
The sample encompasses older individuals who were living at home as well as in institutions. Most interviews (>60 % in all survey waves) were conducted face-to-face in the older person’s home. However, when this was not possible, the interviews were conducted by telephone. If direct interviews with the older persons were not possible, indirect interviews with proxies (e.g., relatives or caregivers) were conducted instead. The characteristics of the sample are described in Table 1.
Variables
Education was measured as level of education, distinguishing between those who had a grade school education or less and those who had an education beyond grade school.
Self-rated health was assessed by the question: ‘How would you rate your general health? Good, poor, or somewhere in between?’ Those who responded ‘poor’ or ‘somewhere in between’ were classified as having suboptimal self-rated health.
Musculoskeletal pain was assessed with an index based on questions about whether the respondent, during the past 12 months, had experienced pain in the shoulders, back, hips, hands, elbows, or knees. Those who reported having experienced slight pain in at least three areas or severe pain in at least one area were classified as having problems with musculoskeletal pain.
Psychological distress was assessed with an index of two questions, one on nervous problems (anxiety) and one on depression/deep sadness. Those who reported either slight problems in both of these areas or severe problems in at least one area were classified as having psychological distress.
Impaired mobility was assessed with an index that consisted of two questions. Those who reported being unable to walk 100 m without problems and/or being unable to walk up and down stairs without problems were classified as having impaired mobility.
Activities of daily living problems were assessed with an index that consisted of five items. Respondents who reported problems with at least one of the following activities were classified as having ADL problems: getting in and out of bed, getting dressed, going to the toilet by themselves, eating, and washing their hair.
Impaired function was assessed with an index of physical tests. The respondents were asked to: (1) pick up a pencil from the floor, (2) rise up from a chair without using the armrests, (3) lift a packet of salt (1 kg), (4) touch their right ear with their left hand and vice versa, (5) touch the toes of their right foot with their left hand and vice versa, (6) place both hands under their thighs, and (7) turn both hands. Respondents who were unable to do at least one of the tests were classified has having impaired function.
Lung function was assessed by peak expiratory flow (L/min). The respondents performed three independent measures of exhalation, and the best result was used as an indicator of lung function. This measure of lung function is highly correlated with the general health of older persons (Roberts and Mapel 2012).
Because of the subjective nature of the global self-rated health question, only responses from direct interviews were included in the analyses (i.e., responses from proxy interviews were not included). Similarly, data on physical function and lung function came only from those who were directly interviewed and fit enough to take the tests. All other indicators also include responses given by proxies.
Statistical analyses
As a first step, we explored the time trends in unadjusted prevalences of health problems both for the total population, and by level of education. The statistical significances of the differences were assessed using logistic regressions.
Similarly, time trends in average lung function were first assessed by plotting the average performance on the expiratory flow rate test. This was done separately for men and women, as performance on these tests vary substantially by gender. The statistical significances of the differences were assessed using ordinary least squares (OLS) regressions.
Finally, the patterns were analyzed using multivariate logistic regressions and OLS regressions (for lung function). The results of the multivariate analyses of the dichotomous outcomes are presented as average marginal effects (AME), and the results of the final analyses of peak expiratory flow performance are presented as β-values. The AME should be interpreted as the average difference in probability of the outcome depending on the value of the independent variable. These estimates are shown with 95 % confidence intervals.
Results
Figure 1 shows the unadjusted prevalences of suboptimal self-rated health, musculoskeletal pain, psychological distress, impaired mobility, ADL problems, and impaired function by level of education and survey year. The prevalences of health problems increased for both educational groups during the period for all outcomes, except ADL problems.

Unadjusted prevalences of health problems by educational level in Sweden, 1992–2011. Solid black lines denote estimates for those with a grade school education or less, solid gray lines denote estimates for those with an education beyond grade school, and black dotted lines denote estimates for the population as a whole
The probability of suboptimal self-rated health increased from 47 % in 1992 to 52 % in 2011. While there were substantial differences by level of education in the probability of suboptimal self-reported health (i.e., those with a higher level of education reported better health on average), the trend over time was similar in both educational groups; thus, the education-related gap in health remained stable over the period.
A similar pattern was observed for the prevalence of musculoskeletal pain. The probability of pain increased from 36 % in 1992 to 48 % in 2011. A clear and stable gap in the probability of pain was observed between the two educational levels: those with a higher level of education were less likely to report problems with musculoskeletal pain.
The prevalence of psychological distress also increased during the period, from 9 % in 1992 to 17 % in 2011. However, there were only minor differences by level of education in the likelihood psychological distress in 1992 and 2002, and no differences at all in 2011.
The prevalence of impaired mobility also increased over the period, from 46 % in 1992 to 54 % in 2011. There was a substantial and stable gap between respondents from the two educational groups: those with a lower level of education were more likely to report impaired mobility throughout the whole period.
The prevalence of ADL problems, on the other hand, followed quite a different pattern. The likelihood of ADL problems decreased from 27 % in 1992 to 23 % in 2011. Substantial differences by level of education were also observed in the probability of ADL problems. Those with a lower level of education were more likely to report problems than those with a higher level. However, these inequalities decreased somewhat during the period.
The prevalence of impaired function remained fairly stable during the period, with 49 % in 1992 to 51 % in 2011. Substantial differences by level of education were observed in throughout the period, but they were substantially smaller in 2002 than in 1992 and 2011.
The observed long-term (1992–2011) changes in the prevalences of health problems were statistically significant (P < 0.05) for musculoskeletal pain, psychological distress, and impaired mobility; but not for self-rated health, ADL, or impaired function. The observed educational differences in health were statistically significant for all periods and outcomes except for psychological distress in 2002 and 2011, ADL in 2002, and impaired function in 2002.
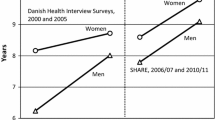
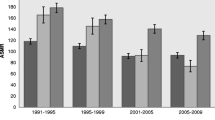
Figure 2 shows the average peak expiratory flow performance by gender and level of education. Perhaps most striking is the decrease in average performance observed among both women and men. Women’s average performance sank from 280 L/min in 1992 to 246 L/min in 2011. Men’s average performance sank from 403 L/min in 1992 to 387 L/min in 2011. A clear difference in predicted performance by level of education was observed in both women and men: those with a grade school education or less perform worse, on average, than those with education beyond grade school. These educational differences attenuated during the period.

Average lung function (peak expiratory flow rate) by educational level in Sweden, 1992–2011. Solid black lines denote estimates for those with grade school education or less, solid gray lines denote estimates for those with an education beyond grade school, and black dotted lines denote estimates for the population as a whole
The observed long-term (1992–2011) changes in the average peak expiratory flow performance were statistically significant for women, but not for men. The observed educational differences in average performance were statistically significant for women in 2002 and 2011, and for men during all periods.
Table 2 shows the differences by educational level and the time trends in probabilities for the dichotomous outcomes in terms of AME. In sum, the results show that those with a lower level of education were statistically significantly and more likely to report health problems in all domains except psychological distress. The strongest association was found between level of education and impaired function: those with a grade school education or less had a 15.9 % point higher probability of failing at least one of the functional tests than those with an education beyond grade school. However, as seen in Fig. 1, this strong association was only discernible in 1992 and 2011. In 2002, the association was between education and functional impairment was substantially weaker.
Moreover, the probability of health problems increased significantly over the period in all domains except ADL problems and impaired function. The probability of experiencing impaired functional impairment increased significantly between 1992 and 2002, but decreased between 2002 and 2011. Thus, the long-term trend in functional impairment, between 1992 and 2011, showed no significant changes.
Conversely, the probability of ADL problems decreased over the period. In 2011, the probability of reporting ADL problems was almost five percentage points lower than in 1992. This decrease was statistically significant.
Table 3 shows the regression estimates of peak expiratory flow performance. The analyses showed significant differences in the average performance of both women and men by level of education: those with a higher level of education significantly outperformed those with a lower level of education. Moreover, average performance decreased significantly in both women and men during the period.
As the final step in the analysis, we checked for statistically significant interactions between education and period in their association with the different health indicators (results not shown). This was done to assess whether any statistically significant changes in the magnitude of the health inequalities occurred during the period. The results yielded one statistically significant interaction effect (p = 0.003) between education and period, in the analysis of impaired function. Further analyses, stratified by period, revealed that there were substantial, statistically significant associations between education and impaired function in 1992 and 2011 whereas the association was substantially weaker and not statistically significant in 2002.
Discussion
This study explored patterns and trends in health and health inequalities among the oldest old in Sweden during the period 1992 to 2011. In sum, the results showed that—with the exception of ADL problems—the prevalence of all indicators of health problems increased during the period. The prevalence of ADL problems, on the other hand, decreased significantly during the period.
All indicators of health but psychological distress were distinctly stratified by education. Individuals with a grade school education or less were more likely to report and exhibit health problems than individuals with a higher level of education. These differences were remarkably stable over the whole period. The only significant change that occurred in these patterns was that the inequalities in performance on tests of physical function were attenuated and rendered statistically insignificant in 2002, only to re-emerge in 2011 as strongly and significantly as in 1992. Hence, this change in pattern may reflect a statistical fluke rather than an actual change in the population. While all health outcomes in the study are at risk for artifactual variation, the indicators of physical function, lung function, and self-rated health are perhaps more susceptible than the other indicators. As they are assessed by tests and subjective judgments, we only have data for those who were well enough to take the tests, and to answer for themselves. Subsequently, the analyses of these outcomes are based on smaller samples and, thus, more vulnerable to fluctuations.
The results should be interpreted with caution. The samples in the study were small, and the health indicators used were crude and are difficult to interpret from a clinical perspective. Even though the surveys were conducted in a comparable manner and response rates exceeded 80 % in all three waves, it is possible that the meaning of the self-rated health indicators have changed over the period. In other words, it is possible that the aspirations and points of reference of the oldest old with regard to their own health have changed during the period. Such a development could lead to changes in the reported prevalence of health problems that do not correspond to changes in actual morbidity. However, as the patterns of performance on the physical tests largely mimic those observed for self-reported health problems, it is unlikely that the increase in self-reported health problems can be solely explained by changes in aspirations and frames of reference.
Furthermore, the indicator of education is crude and dichotomous, and a great deal of variance in educational achievements is unaccounted for in the study. As these unmeasured differences in education are likely associated with health, the study probably underestimates differences in health by level of education.
While the studies are not directly comparable, it is interesting to note that, in contrast with the widening disparities observed among older adults observed in the US (Shoeni et al. 2001, 2005), and partly in the Netherlands and UK (Hoogendijk et al. 2008; Martin et al. 2012), there were no indications of changes in the magnitude of the educational disparities in health among the oldest old in Sweden. Instead the results suggest, in accordance with previous findings from Finland and Sweden (Sulander et al. 2006, 2009; Fors et al. 2008), that the association between education and health among the oldest old is remarkably stable. It has remained largely unaffected by the educational expansion, increasing income inequalities, decreasing poverty rates, increasing survival, and changing prevalences of health problems. Thus, the impact of these developments on the magnitude of the educational disparities in health seems to have been either negligible, offset by each other, or offset by other factors. At the same time, the change in the educational structure means that the proportion of the population in the advantaged group, with higher education, increased over time as the proportion in the disadvantaged group, with less education, decreased.
However, despite this favorable development, there were statistically significant increases in the (unadjusted) prevalences of musculoskeletal pain, psychological distress, and impaired mobility during the period. Similarly, unadjusted models also revealed a statistically significant worsening of the average lung function among women during the period. Hence, it seems the increasing average education in the population have, at best, served to constrain the negative trend observed for these health outcomes.
In conclusion, these results suggest that the health status of the oldest old has decreased over the last two decades. However, in contrast to the increases in rates of health problems, the rates of disability decreased significantly between 2002 and 2011.
In other words, the results only partly support any notion suggesting that health improvements among older adults may serve to soften the societal challenges of the aging population in terms of health and social care provision. Moreover, despite these health changes, substantial and stable education-related differences were found in almost all indicators of health. Thus, the results suggest that the association between socioeconomic position and health is remarkably robust. It persists into the oldest age groups, is consistently found in a wide range of health outcomes, and tends to be stable over extended periods of time.
References
Christensen K, Dolbhammer G, Rau R, Vaupel JW (2009) Ageing populations: the challenges ahead. Lancet 374:1196–1208
Christensen K, Thinggaard M, Oksuzyan A et al (2013) Physical and cognitive functioning of people older than 90 years: a comparison of two Danish cohorts born 10 years apart. Lancet 382:1507–1513
Fors S, Lennartsson C, Lundberg O (2008) Health inequalities among older adults in Sweden 1991-2002. Eur J Public Health 18(2):138–143
Fors S, Lennartsson C, Lundberg O (2009) Childhood living conditions, socioeconomic position in adulthood, and cognition in later life: exploring the associations. J Gerontol B Soc Sci 64B(6):750–757
Fors S, Modin B, Koupil I, Vågerö D (2012) Socioeconomic inequalities in circulatory and all-cause mortality after retirement—the impact of mid-life income and old age pension: evidence from the Uppsala Birth Cohort Study. J Epidemiol Community Health 66:e16
Fors S, Agahi N, Shaw BA (2013a) Paying the price? The impact of smoking and obesity on health inequalities in later life. Scand J Public Health 41(2):134–141
Fors S, Lennartsson C, Agahi N, Parker MG, Thorslund M (2013b) Äldre har fått fler hälsoproblem, men klarar vardagen bättre [Older people manage their everyday activities better despite increases in health problems]. Läkartidningen 110:CA33
Freedman VA, Martin LG, Schoeni RF (2002) Recent trends in disability and functioning among older adults in the United States: a systematic review. JAMA 288(24):3137–3146
Gustafsson B, Johansson M, Palmer E (2009) The welfare of Sweden’s old-age pensioners in times of bust and boom from 1990. Ageing Soc 29:539–561
Hoogendijk E, Broese van Groenou M, van Tilburg T, Deeg D (2008) Educational differences in functional limitations: comparisons of 55-65-year-olds in the Netherlands in 1992 and 2002. Int J Public Health 53:281–289
Kibele EUB (2014) Individual- and are-level effects on mortality risk in Germany, both East and West, among male Germans aged 65+. Int J Public Health 59:439–448
Knesebeck Ovd, Lüschen G, Cockerham WC, Siegrist J (2003) Socioeconomic status and health among the aged in the United States and Germany: a comparative cross-sectional study. Soc Sci Med 57(9):1643–1652
Lennartsson C, Agahi N, Hols-Salén L et al (2014) Data resource profile: The Swedish Panel Study of Living Conditions of the Oldest Old (SWEOLD). Int J Epidemiol 43(3):731–738
Leopold L, Engelhartdt H (2013) Education and physical health trajectories in old age. Evidence from the Survey of Health, Ageing and Retirement in Europe (SHARE). Int J Public Health 58:23–31
Martin LG, Schoeni RF, Andreski PM, Jagger C (2012) Trends and inequalities in late-life health and functioning in England. J Epidemiol Community Health 66:874–880
Mirowsky J, Ross CE (2003) Education, social status and health. Aldine de Gruyter, New York
Ploubidis GB, Mathenge W, De Stavola B, Grundy E, Foster A, Kuper H (2013) Socioeconomic position and later life prevalence of hypertension, diabetes and visual impairment in Nakuru, Kenya. Int J Public Health 58:133–141
Roberts MH, Mapel DW (2012) Limited lung function: impact of reduced peak expiratory flow on health status, health care utilization, and expected survival in older adults. Am J Epidemiol 176(2):127–134
Rosén M, Haglund B (2005) From healthy survivors to sick survivors–implications for the twenty-first century. Scand J Public Health 33(2):151–155
Schoeni RF, Freedman VA, Wallace RB (2001) Persistent, consistent, widespread, and robust? Another look at recent trends in old-age disability. J Gerontol B Soc Sci 56B(4):S206–S218
Schoeni RF, Martin LG, Andreski PM, Freedman VA (2005) Persistent and growing socioeconomic disparities in disability among the elderly: 1982-2002. Am J Public Health 95(11):2065–2070
Schoeni RF, Liang J, Bennett J, Sugisawa H, Fukaya T, Kobayashi E (2006) Trends in old-age functioning and disability in Japan, 1993–2002. Population studies. J Demogr 60(1):39–53
Statistics Sweden (2013) Sveriges framtida befolkning 2013–2060 [The future population of Sweden 2013–2060]. Statistics Sweden 2013; BE 18 SM 1301
Sulander T, Martelin T, Sainio P, Rahkonen O, Nissinen A, Uutela A (2006) Trends and educational disparities in functional capacity among people aged 65–84 years. Int J Epidemiol 35:1255–1261
Sulander T, Rahkonen O, Nummela O, Uutela A (2009) Ten year trends in health inequalities among older people, 1993–2003. Age Ageing 38(5):613–617
Thorslund M, Lundberg O (1994) Health and inequalities among the oldest old. J Aging Health 6:51–69
van Vliet O, Been J, Caminada K, Goudswaard K (2012) Pension reform and income inequality among older people in 15 European countries. Int J Soc Welfare 21:S8–S29
Acknowledgments
Stefan Fors gratefully acknowledges financial support from the Swedish Research Council for Health, Working Life and Welfare: grant 2012-0761.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fors, S., Thorslund, M. Enduring inequality: educational disparities in health among the oldest old in Sweden 1992–2011. Int J Public Health 60, 91–98 (2015). https://doi.org/10.1007/s00038-014-0621-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-014-0621-3