
Abstract
Objectives
Potential health hazards for the environment and people living nearby landfills and incinerators are claimed to be related to several methods of waste management. Independent systematic review of the scientific literature is a key procedure to support the lay public and policy makers to achieve informed decisions.
Methods
The study design and potential biases of papers retrieved in this comprehensive literature search were analyzed.
Results
The most consistent result is that the risks of congenital anomalies and hospitalization due to respiratory disease are likely to be real nearby special waste landfills. From the very little information on exclusively urban waste depots it is reasonable to say that correct management of landfill does not increase the risk of these health effects. It is confirmed that historically incinerators are an important source of pollution and harm for the health of populations living nearby; however, changes in technology are producing more reassuring results.
Conclusions
A moderate level of confidence is possible in limited areas of knowledge, implying the need to overcome the limitations of current studies about exposure assessment and to control confounders at the individual level.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Management of solid waste disposal is a priority issue in the organization of modern societies. In spite of the increasing recycling activities, landfills and incinerators are widely used to manage the final phase of waste disposal. Potential health hazards for the environment and people living nearby are claimed to be related to waste management, which is known to release potentially harmful substances although in small quantities and at very low levels. Many uncertainties surround the assessment of health effects, and the need for independent systematic reviews of the current scientific information is urgent in order to provide the lay public and policy makers with reliable lines of scientific knowledge. A number of reviews are already available (Vrijheid 2000; Hu and Shy 2001; Rushton 2003; Dolk and Vrijheid 2003; Department for Environment, Food and Rural Affairs (DEFRA) 2004; Franchini et al. 2004; Michaels and Monforton 2005; Minichilli et al. 2005; Linzalone and Bianchi 2007; World Health Organization (WHO) 2007; Russi et al. 2008; Signorelli et al. 2008; Giusti 2009; Porta et al. 2009). The reviews underline the difficulties in interpreting data from primary studies because of the lack of accurate exposure information and control of potential confounders. This problematic interpretation further complicates a scenario where risk communication is poorly manageable, risk perception is greatly biased, and conflicting interests become the dominant issues for discussion, implying huge difficulties in managing public health issues affecting the safety of communities. This review updates the evaluation of evidence (19 more papers on landfills and 13 on incinerators included in the tables in the “Electronic supplementary material”) derived from the literature on the health effects of landfills and incinerators in people living in their proximity and discusses the degree of uncertainty associated with the risk estimates, thereby providing researchers, citizens, and institutions with an updated independent piece of evidence. This process has been promoted by the Italian authorities after the dramatic garbage management failures in Campania, an Italian area where the safety of communities has been put in danger by very bad organization and the presence of several illegal landfills; the resultant potential health hazards in some areas of Campania are associated with higher mortality rates for various diseases in comparison with those in other regional areas (Altavista et al. 2004; Comba et al. 2006; Martuzzi et al. 2009; Fazzo et al. 2008, 2011).
Methods
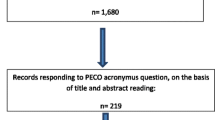
The scientific literature was scrutinized through computerized literature searches using PubMed, Embase, Web of Science, and the Cochrane Library from 1 January 1983 to 1 June 2012. The search strategy consisted in the use of various combinations, in line with the specific database language, of the terms “incinerat* OR “refuse disposal” OR “refuse disposals” OR landfill*”, “population* OR habitant*”, “environmental exposure”, “environmental disease”; the search was subsequently improved using more restrictive terms related to both exposure to disposal sites and disease outcomes. Primary publications on the health effects of landfills and/or incinerators on the population living in the proximity were the subject of this systematic review. Other types of papers (systematic reviews, biomonitoring of toxic agents in the proximity of waste disposal sites, environmental impact estimation) were consulted in order to integrate all the available scientific information for the interpretation of the results. The search was completed using the references identified in the retrieved papers and any highlighted by the working group. A total of 201 relevant papers were identified, 101 on landfills and 100 on incinerators. The papers were screened for eligibility by two independent reviewers; disagreements were resolved by discussion. Out of 100 papers on landfills, 71 were excluded (1 systematic review, 1 duplicate paper, 1 focused on occupational exposure, 34 biological studies, 34 other non-relevant types of papers); therefore 29 papers were evaluated (4 cohort studies, 8 case–control studies, 17 ecological studies). Out of 100 papers on incinerators, 69 were excluded (2 systematic reviews, 1 duplicate paper, 1 focused on occupational exposure, 29 biological studies, 36 other non-relevant types of papers); therefore 31 papers were evaluated (2 cohort studies, 9 case–control studies, 17 ecological studies, 3 cross-sectional studies). The list of excluded papers is reported in Appendix A (Electronic supplementary material).
Information on study subjects (number, age, gender, country), exposure assessment, outcome assessment, estimated effects, and potential bias were independently abstracted by three observers using a predefined format, and disagreements were resolved by discussion. Characteristics of the studies are reported in Appendices B and C (Electronic supplementary material) for landfills and incinerators, respectively. The tables therein are arranged by outcome.
To assess the size and direction of potential biases an evaluation scale is proposed that envisages exposure assessment, outcome assessment, and confounding control (Table 1). For each item the null value (0) indicates that no influence on the estimation is likely, a positive sign that the effect estimates could be less (+) or more (++) overestimated, and a negative sign that the effect estimates could be less (−) or more (− −) underestimated. As for exposure assessment, underestimation is considered according to the study designs; conversely for outcome and confounding assessment, overestimation is considered (Porta et al. 2009; WHO 2007; Franchini et al. 2004; Giusti 2009). The results of this evaluation were discussed among three authors (SP, EB, and PC) and the grade was assigned according to the majority rule in case of inconsistencies.
An attempt to define the relationship between the process (landfill/incinerator) and the various diseases in terms of potential cause–effect evaluation was performed according to Porta et al. (2009), using the International Agency for Research on Cancer (IARC) criteria for carcinogenesis (IARC–WHO, 2013). The results of this evaluation were discussed among three authors (SP, EB, and PC) and the relationship was assigned according to the majority rule in case of inconsistencies.
Results
Studies on communities living near landfills
Twenty-nine papers on the health effects in communities living in the proximity of landfills were evaluated. One of the major issues in the evaluation was the difficulty in distinguishing between solid urban waste and other types of wastes. There is not yet a standardized definition of the various types of wastes. The terms dangerous, special, toxic, industrial, and commercial are not uniformly used in different countries and over time periods. Moreover, the types of wastes disposed in a landfill may have changed over time. The outcomes considered in the papers were all cancers, birth defects, respiratory diseases, and total mortality. In some papers multiple outcomes were evaluated.
Cancer
The relationship between landfills and cancer has been evaluated in seven studies (5 ecological, 1 cohort, and 1 case–control)
Colorectal
A cohort study carried out in Finland compared the incidence of colorectal cancer in a community in the proximity of a landfill containing industrial and urban wastes to that in a control cohort (Pukkala and Pönkä 2001). No difference was found, but the low number of cases and the lack of adjustment for confounders, beside age and sex, make the results less reliable. An ecological study in Australia evaluated mortality and incidence in populations living nearby a landfill containing urban special and dangerous wastes, both liquid and solid, did not find any risk excess, but again involved a low number of cases (Williams and Jalaludin 1998).
Liver
In an ecological study that analyzed mortality in a community living in an Italian area containing a landfill, an incinerator, and a refinery, liver cancer mortality was not different in populations living at various distances from the sites, after adjustment for age and deprivation index and separately by sex (Michelozzi et al. 1998). In another Italian study a potential risk was found in males, but no adjustment was made and information on outcomes cannot be related to the distance from the landfills (Minichilli et al. 2005). A Canadian case–control study found no significant trend in populations living at various distances from an urban waste landfill, adjusting for some confounders (Goldberg et al. 1999). Multiple comparisons on 30 cancer sites and the low number of cases suggest that caution be adopted in interpreting these results. A Brazilian ecological study of urban landfills in Sao Paolo found no difference comparing people living at less and more than 2 km from several sites (Gouveia and Ruscitto do Prado 2010a).
Bladder
A large national ecological study, carried out in the UK, analyzed the incidence of bladder cancer in populations living at various distances from a landfill site (Jarup et al. 2002) and did not detect any association, nor when only special wastes were considered. Two other studies were unable to detect any association (Williams and Jalaludin 1998; Gouveia and Ruscitto do Prado 2010a).
Larynx
A significant decrease of mortality rates as the distance from the sites increased was reported in Italy, but with low numbers (Michelozzi et al. 1998). Another study in Canada did not detect any association (Williams and Jalaludin 1998).
Lung
None of the three evaluated studies was able to detect any association (Williams and Jalaludin 1998; Michelozzi et al. 1998; Pukkala and Pönkä 2001).
Kidney
Two studies found a modest non-significant increase in risk (Michelozzi et al. 1998; Goldberg et al. 1999).
Lymphomas
Only one study (Goldberg et al. 1999) found a significant association, whereas those by Williams and Jalaludin (1998) and Michelozzi et al. (1998) did not.
Leukemia
Two studies in children (Jarup et al. 2002; Gouveia and Ruscitto do Prado 2010a) and four in adults (Williams and Jalaludin 1998; Michelozzi et al. 1998; Jarup et al. 2002; Gouveia and Ruscitto do Prado 2010a) were unable to detect any association.
Brain
No association was found in a UK study (Jarup et al. 2002). An increased risk only in males living in the proximity of the landfill was detected in a US study (Williams and Jalaludin 1998), limited by low numbers of cases.
Other cancers
In a previously described study no association was found for breast, uterus, prostate, stomach, and skin cancers (Williams and Jalaludin 1998). Goldberg found an increased risk for pancreatic cancer but not for prostate (Goldberg et al. 1999). Another study found an increased risk for skin and pancreatic cancers only in males (Pukkala and Pönkä 2001).
Birth defects and reproductive disorders
Out of the 22 studies analyzing the relationship between these disorders and the presence of landfills, 13 are ecological, 2 cohort, and 7 case–control.
Birth defects in general
Six studies found statistically significant associations (Fielder et al. 2000, 2001; Elliott et al. 2001, 2009; Palmer et al. 2005; Vrijheid et al. 2002), but five other studies (Morris 2003; Dummer et al. 2003b; Boyle et al. 2004; Kloppenborg et al. 2005; Gouveia and Ruscitto do Prado 2010a) did not. In the UK an ecological study of residential distance from a site, the risk of congenital malformations was higher; however, that risk was also detected by analyzing data before the opening of the landfill (Fielder et al. 2000). A national UK study analyzed congenital anomalies and low birth weight in populations living at different distances from a large number of waste sites (19,196) (Elliott et al. 2001). A statistically significant association was found (RR 1.05), but it disappeared for urban solid waste (RR 0.99) when analyzed separately from toxic waste (RR 1.08) (Elliott et al. 2009). A Danish national ecological investigation found no association in comparing people living at different distances from the sites (Kloppenborg et al. 2005). Evaluating the rates before and after the opening of 24 landfills in Wales, Palmer et al. (2005) found a significant increase over time. Among residents of areas close to 15 landfills in Brazil no association was detected comparing rates of people living at less than 2 km and the whole city, after adjustment for sex and age (Gouveia and Ruscitto do Prado 2010a). Another UK study reported on a landfill where all kinds of wastes (urban solid, industrial, and special) were transferred, and compared three areas close to site and 26 distant areas (Fielder et al. 2001). After the opening of the site a significant risk increase in the closest areas was found, but the authors cautiously interpreted the findings owing to poor accuracy and incompleteness of data. A Scottish investigation found no association in residents at less than 2 km from the site compared with those at more after adjustment for age and deprivation index (Morris 2003). A multicenter case–control study (EUROHAZCON), carried out in five countries (Belgium, Denmark, France, Italy, and the UK), found a significant increase in congenital malformations in people living nearby sites containing dangerous substances (Vrijheid et al. 2002). Caution is suggested in interpreting the results owing to the difficulty in correctly classifying the sites according to their dangerousness. A previous investigation on dangerous waste landfills had found conflicting results (Geschwind et al. 1992). In a UK retrospective cohort study stratifying by three time periods and four types of landfills, Dummer et al. (2003b) found no association. A similar lack of association was found in a study on urban solid wastes in Northern Ireland (Boyle et al. 2004).
Non-chromosomal birth defects
The EUROHAZCON case–control study detected an increase in risk of non-chromosomal birth defects in people living at less than 3 km from landfills containing both urban solid and industrial or toxic wastes (Dolk et al. 1998). In this study a statistically significant increased risk was found in the subgroups of neural-tube defects (OR 1.86), malformations of the cardiac septa (OR 1.49), and anomalies of great arteries and veins (OR 1.81).
Nervous system birth defects
In a UK retrospective cohort study in which data were stratified by three time-periods and four types of landfills, congenital anomalies were significantly higher close to urban solid waste landfills (Dummer et al. 2003b), whereas a previous study had not found this relationship (Croen et al. 1997). Another study confirmed the association for a landfill containing toxic substances (Marshall et al. 1997).
Cardiovascular defects, hypo- and epispadias, oral defects
Statistically significant higher risk of hypo- and epispadias was detected in children living close to industrial toxic wastes (Geschwind et al. 1992). For cardiovascular and oral anomalies no such risk was found in another investigation (Croen et al. 1997).
Down syndrome
No association was found for Down syndrome in the analysis of 6,829 sites (Jarup et al. 2007).
Sirenomelia and cyclopia
The two studies on this malformations analyzed four cases of sirenomelia and four of cyclopia (Castilla and Mastroiacovo 2008; Orioli et al. 2009). The identification of a possible cluster of sirenomelia has to be interpreted cautiously in the light of this very low number of observations.
Low birth weight
A retrospective cohort study in Alaska took into account several confounders and classified sites according to dangerousness, finding a risk nearby the sites with intermediate and high dangerous levels (Gilbreath and Kaas 2006). An ecological study in the UK, part of the EUROHAZCON on mixed sites, found a small significant risk increase in residents at less than 3 km, evaluating seven areas close to ten sites (Morgan et al. 2004). A case control study in Quebec found a small increase in risk which persisted after adjustment for several confounders; however, it did not find any association with preterm births (Goldberg et al. 1995). As reported in a previous section a nationwide UK study reported an increase, with no distinction between the types of waste disposed (Elliott et al. 2001). Only an ecological UK study, described above, found no association (Fielder et al. 2000).
Respiratory diseases
A retrospective Finnish study on a site containing urban and industrial wastes reported an increase of asthma incidence (Pukkala and Pönkä 2001), and an ecological investigation in the UK found an increase in hospitalization for respiratory diseases, again dealing with a waste site also containing industrial wastes (Fielder et al. 2001). In another retrospective US cohort study the results suggested an increased rate of hospitalization for asthma and respiratory diseases (Ma et al. 2007).
Total mortality
Three ecological studies reported on this association: no association was reported in one (Williams and Jalaludin 1998), whereas in two there was some indication of a positive association (Fielder et al. 2001; Minichilli et al. 2005). However, in the study by Williams and Jalaludin (1998) the detected risk was consistent with that reported before the opening of the site; in the other studies there is no indication of the distance from the site. No association was found in a US cohort study (Gensburg et al. 2009).
Studies of communities living near incinerators
Thirty-one papers on the health effects in the communities living in the proximity of incinerators were evaluated. The following outcomes were considered: cancers (15), birth defects (10), respiratory diseases (5), cardiovascular diseases (1), total mortality (1), and skin disease (1). In some papers multiple outcomes were evaluated.
Cancer
Fifteen studies analyzed the relationship between incinerators’ activity and cancer. Most studies are ecological or case–control and only one is based on a retrospective cohort.
All cancers
Three ecological (Elliott et al. 1996; Goria et al. 2009; Federico et al. 2010) and one retrospective cohort study (Ranzi et al. 2011) evaluated the association between incinerators and all cancers in adults. In a UK ecological study the incidence increased; however, no adjustment for relevant confounders was performed and the authors claimed to be cautious in their interpretation (Elliott et al. 1996). In an Italian study no association was reported in the four geographical areas analyzed (Federico et al. 2010), whereas another Italian cohort study reported an increase in all-cancer mortality (RR 1.47) in women exposed to elevated levels of heavy metals (>2 ng/m3) (Ranzi et al. 2011). In a modeling risk estimation study a linear relationship was found, but limitations in study design and patient selection imply problems of interpretation (Goria et al. 2009). In an ecological study no excess risk of cancer mortality was found in children aged less than 5 years (Gouveia and Ruscitto do Prado 2010b), but according to analyses coming from a companion study to that of Elliott et al. (1996) the influence of population migration might influence the results owing to poor accuracy of the case findings (Knox 2000). Overall, the evidence appears weak and conflicting.
Non-Hodgkin lymphomas
Three ecological studies and one cohort study found no association (Elliott et al. 1996, Federico et al. 2010; Gouveia and Ruscitto do Prado 2010b; Ranzi et al. 2011), whereas two case–control studies and one ecological study found a positive association with dioxin levels (Viel et al. 2000; Floret et al. 2003; Viel et al. 2008a), especially in women (Viel et al. 2008a); however, some exposure measurement errors may misestimate the effects. An ecological Italian study reported higher Standardized Mortality Ratio (SMR) between 1986 and 1992 for non-Hodgkin lymphomas (not for Hodgkin lymphomas) in a municipality where an incinerator had operated until 1985 (Biggeri and Catelan 2005).
Sarcoma and soft tissues
Six ecological (Elliott et al. 1996; Viel et al. 2000; Floret et al. 2004; Biggeri and Catelan 2005; Viel et al. 2008a; Federico et al. 2010), two case–control (Comba et al. 2003; Zambon et al. 2007), and one cohort studies (Ranzi et al. 2011) provide data. No association was shown in five (Elliott et al. 1996; Floret et al. 2004; Biggeri and Catelan 2005; Federico et al. 2010; Ranzi et al. 2011). The other studies reported: (a) significant risk increase associated with living less than 2 km from the site, but based on five cases and with a very wide confidence interval (Comba et al. 2003); (b) significant risk increase by level and duration of exposure, especially in women (Zambon et al. 2007); (c) risk increase but at exposure levels higher than those detectable in more modern incineration technologies (Viel et al. 2000, 2008a). The evidence of risk due to an old-generation plant is convincing.
Breast
No association was found in a case–control and a cohort study (Viel et al. 2008b; Ranzi et al. 2011). A small association was found in a study designed to compare different ways of modeling exposure and confounding, and the results are strongly limited by this study objective (Goria et al. 2009).
Lung
Two ecological studies and one case–control study reported a risk excess in people living close to the emission site (Elliott et al. 1996; Biggeri et al. 1996; Parodi et al. 2004). In the studies carried out in Italy, there might be an exposure misclassification because other pollution sources were present but not identified (Biggeri et al. 1996; Parodi et al. 2004). More recent investigations, with better exposure measurement, found no association (Federico et al. 2010; Gouveia et al. 2010b; Ranzi et al. 2011).
Colorectal
An increased risk with distance from the site was reported in the UK, but the authors cautiously suggest possible overestimation due to poor control of confounding factors (Elliott et al. 1996). No risk was found in an ecological study in Italy, with a good outcome measurement (Federico et al. 2010). In the same region another cohort study found higher mortality in men and higher incidence in women, but the increased risk was found at heavy metal exposure levels of 1–2 ng/m3 and not at higher levels (Ranzi et al. 2011).
Liver
Recent studies found no association (Federico et al. 2010; Gouveia et al. 2010b; Ranzi et al. 2011). A less recent investigation in the UK had found a significant risk increase associated with smaller distances from the sites (Elliott et al. 1996). A subsequent analysis of this data and including a histological evaluation of cancer cases confirmed the findings. (Elliott et al. 2000). A Brazilian study carried out in rural deprived areas found an association, but its validity is diminished by flaws in the study design (Goria et al. 2009).
Larynx
Three ecological studies and one cohort study found convincing associations (Elliott et al. 1996; Federico et al. 2010; Gouveia et al. 2010b; Ranzi et al. 2011)
Leukemia
An Italian ecological study found a modest risk increase in residents between 2 and 3.5 km from the site, but not at shorter distances; the authors suggest that this risk is hardly linkable with the distance from the site (Federico et al. 2010). No association was found in a cohort study in adults in Italy (Ranzi et al. 2011) and in an ecological study in children in Brazil (Gouveia et al. 2010b). A UK ecological study in children under 16 years found a risk increase but with a mixed exposure (incinerator and industrial combustion) (Knox 2000).
Stomach
An ecological study found a significant risk increase associated with the distance from the site, but control of confounding factors was poor (Elliott et al. 1996). An Italian cohort study reported a risk increase for women exposed to heavy metal levels of 1–2 ng/m3, but not for those exposed to higher levels (Ranzi et al. 2011).
Bladder
No association was found either in a UK ecological study (Elliott et al. 1996) and in an Italian cohort study (Ranzi et al. 2011).
Cerebral, myeloma, lymphatic system, prostate
Only one study reported on these cancers (Ranzi et al. 2011); no association was found between incidence and mortality for these diseases and exposure to heavy metals in populations living nearby two incinerators.
Birth defects and reproductive disorders
Ten studies were evaluated (Lloyd et al. 1988; Jansson and Voog 1989; Williams et al. 1992; ten Tusscher et al. 2000; Cresswell et al. 2003; Dummer et al. 2003a; Tango et al. 2004; Cordier et al. 2004; Vinceti et al. 2008; Cordier et al. 2010): eight ecological, one case–control, and one retrospective cohort study. The results are often inconsistent; however, the paper by Cordier is relevant for interpretation because confounders were controlled for on an individual basis, through a questionnaire (Cordier et al. 2010).
Orofacial defects
No risk increase was found for cleft palate by a Swedish study (Jansson and Voog 1989), whereas both in France and the Netherlands a risk increase was detected (ten Tusscher et al. 2000; Cordier et al. 2004). However, the site analyzed in the Dutch study was open to many chemical substances (ten Tusscher et al. 2000).
Urinary tract defects
The French study by Cordier showed a risk increase (around double after adjustment) for congenital urinary tract defects when women, resident within 10 km from 21 active incinerators, were exposed to atmospheric dioxin and dioxin deposits in the ground during the first months of pregnancy (Cordier et al. 2010). The authors also suggest a possible role of the dioxin in contaminating locally produced food. These data together with those for renal dysplasia require special attention.
Other congenital anomalies
Two studies reported a modest risk increase of spina bifida, cardiac defects, and renal dysplasia in the areas proximal to the incinerator (Dummer et al. 2003a; Cordier et al. 2004). No significant association was found for low birth weight and reproductive defects (Tango et al. 2004), chromosomal and non-chromosomal anomalies (Cresswell et al. 2003), spontaneous abortion and other studied reproductive outcomes (Vinceti et al. 2008). Occurrence of twin and female births were increased (Williams et al. 1992; Lloyd et al. 1988).
Respiratory diseases
Two studies reported a decrease in respiratory function and an increase in respiratory wheezing in children living in the proximity of an incinerator (Hsiue et al. 1991; Miyake et al. 2005). Increased prevalence of chronic respiratory symptoms was detected in other studies comparing populations resident at various distances from the site (Lee and Shy 1999; Shy et al. 1995). In an Italian retrospective cohort a higher respiratory disease mortality was found in men exposed to heavy metals levels of 0.5–1 ng/m3; however, no risk was detected in individuals exposed to higher levels (Ranzi et al. 2011). In the same investigation no difference was found for total mortality and hospitalization for respiratory diseases.
All-cause mortality and cardiovascular diseases
Ranzi found that total mortality in women was associated with the presence of an incinerator at any level of exposure to heavy metals, and an increase in cardiovascular disease mortality in women, in hospitalization for chronic cardiac insufficiency and acute myocardial infarction in men in the mid-category exposure (0.5–1 ng/m3) to heavy metals, but not for the highest (higher than 2 ng/m3) (Ranzi et al. 2011).
Skin diseases
A Japanese study found no association with atopic dermatitis (Lee and Shy 1999), but a reporting bias and poor control of confounding factors indicate a unsatisfactory quality of the paper.
Discussion
The evaluation of the possible health effects has to be done taking into account two relevant issues: (a) in the majority of the papers on landfills it is virtually impossible to distinguish the role of urban solid from other types of waste coming from different sources; (b) the evolving technology of modern incinerators, with improved control of dioxin and heavy metals emission, may enhance the inconsistencies of the results. Because of these constraints any conclusion has to be viewed in the light of variability and some uncertainty in the results. Nevertheless, this review appears to have new important information if compared with the latest published systematic review (Porta et al. 2009).
Landfills
For total mortality evidence is insufficient to indicate a role of urban solid waste; moreover, the lack of control of important confounding factors in most papers is a real issue. For cancers the inadequate level of evidence already reported in previous reviews (Porta et al. 2009) is supported by more recent data (Gouveia et al. 2010a). More intriguing are the results on birth defects and reproductive disorders. An effect is detectable for toxic wastes, as pointed out by old and more recent papers, but this is much less clear when only urban solid wastes are considered. The evaluation of 9,565 landfills in the UK in which Elliott et al. (2009) distinguished between deposits of non-special from special or unknown waste confirmed an effect of the latter and no evidence of harm from the former. The environmental impact evaluation performed by the INTARESE group in three European countries (Italy, Slovakia, and the UK) on residents living at less than 2 km from a landfill with mixed waste estimated an excess risk of 1.96 newborns with defects in the period 2001–2030 (Forastiere et al. 2011). It is reasonable to conclude that the risk of congenital anomalies is likely to be real. Within the framework of a correct management of landfill of strictly urban waste, the risk of these defects is less likely, indicating that solid waste should be very accurately selected before being thrown in a landfill.
Incinerators
Papers dealing with the health effects of incinerators active in the years 1969–1996 consistently report a detectable risk of some cancers in the populations living nearby. The good quality studies confirm these data, as pointed out in other reviews (Franchini et al. 2004; Linzalone and Bianchi 2007; Porta et al. 2009). The large UK study by Elliott et al. (1996) on 72 incinerators found a risk excess for all cancers, stomach, colorectal, liver, lung, and non-Hodgkin lymphomas; other studies carried out in Italy, France, and the UK indicate some suggestive but not consistent results for non-Hodgkin lymphomas and soft tissue sarcomas (Elliott et al. 1996; Viel et al. 2000; Comba et al. 2003; Floret et al. 2004; Zambon et al. 2007; Viel et al. 2008a; Federico et al. 2010; Ranzi et al. 2011). One study that did not detect any association is quite interesting for a number of reasons (Ranzi et al. 2011): the investigation was carried out on a technologically advanced plant which had undergone a number of improvements; the observations were based on a complex model of dispersion as an estimate of exposure; morbidity and mortality were quite accurately evaluated. The paper also provides an interesting analysis comparing emissions at different time periods relative to a different technology: the ratios of concentrations of released substances in 2008 compared with the period 1994–1996 are 0.214 for total suspended particulate, 0.20 for mercury and cadmium, and 0.0001 for dioxins [polychlorinated dibenzo-p-dioxins (PCDD) and polychlorinated dibenzofurans (PCDF)]. These data suggest a dramatic change in the amount of dangerous emissions and the need for accurate monitoring of pollution. In the comparison between older and newer observations, the results for cancer incidence and mortality are largely not consistent.
Attention should be paid to the risk excess for urinary tract defects as reported in a well-designed study by Cordier et al. (2010), even if other studies are inconsistent. Orofacial defects are reported to be associated with exposure to special waste incinerators, whereas no risk is found for reproductive disorders such as spontaneous abortion (Vinceti et al. 2008).
A first general comment is that, historically, incinerators have been consistently indicated as an important source of pollution and harm for the health of populations living nearby the sites. Studies on biomarkers support this: populations exposed to emissions more than others have higher biological levels of released substances (Gonzalez et al. 2000; Reis et al. 2007). Where an incinerator had been the only source of pollution in a defined area for many years in the past, the harmful effects on the health have been consistently detected in a later period (Viel et al. 2000). Second, where a health impact of the change of technology has been reported (as for the Italian study by Ranzi et al. 2011) the results appear reassuring; however, this implies new challenges for the evaluation of environmental impact on health in other societal environments. New objectives of evaluation are needed: (a) the size of incinerators, accurate measurement of nanoparticles; (b) markers of “minor”, but not less important health outcomes (respiratory symptoms, annoyance of the residents, stress-induced risk conditions). The evaluation of the aforementioned conditions in public health should include both incinerators and landfills owing to their association with the quality of life of residents during the time of exposure (de Wet et al. 2011).
Main methodological issues
Environmental epidemiology of waste disposal suffers from limitations conducive to inadequate or contrasting results: because most disease are “rare” in populations, a large number of individuals have to be observed for a long time period to identify a potential determinant, and studies carried out in small communities for a limited number of years lack statistical power; specific attention is often given to communities where exposure is “visibly” higher compared with others, thereby emphasizing the effect; exposure is mostly not based on individual measurements or accurate modeling of differences in population groups; potential concomitant causes of harm to health should be measured and controlled for in the analyses as confounders such as the socioeconomic conditions; the lack of information on individual risk factors competitive for many diseases such as smoking, dietary habits, alcohol use, and occupation, is mostly common. This large variety of conditions impaired the calculation of summary estimates of risks through meta-analyses.
Cause–effect relationship
A summary table (Table 2), using the IARC criteria for cause–effect evaluation, as described in the methods (IARC–WHO) is proposed. Although this classification is applied to evaluate the causal role of potential carcinogens, it allows us to compare the conclusions proposed by us with those by Porta et al. (2009), the latest comprehensive systematic review performed before ours. Only two categories (limited and inadequate) have been used because of the insufficient design of the evaluated studies that suffer from poor exposure measurement, outcome definition, and adjustment for confounding factors. Nevertheless, we have important hints. The category limited is used for some disease, indicating points-of-attention for etiology, the estimation of risks, and their management in public health. One reassuring point is that we should appreciate the continuous improvement in research design and analysis of the relevant investigations. The choices on the mode of waste disposal management are not “neutral”; powerful political and economic interests play a great role “like the choices on energy production, mode of transportation or greenhouse gas emission” and often stand “predominant over the epidemiological evidence” (Forastiere et al. 2008). Within this framework—similarly to other public health decisions taken on a scientific basis—in order to overcome issues of conflicts of interest in scientific production and to avoid the construction of false reassurances or deplorable uncertainties (Michaels and Monforton 2005), it is advantageous to rely on independent systematic reviews where transparency of methods and rigorous evaluation criteria can be checked by the readers.
References
Altavista P, Belli S, Bianchi F, Binazzi A, Comba P, Del Giudice R, Fazzo L, Felli A, Mastrantonio M, Musmeci L, Pizzuti R, Svarese A, Trinca S, Uccelli R (2004) Mortalità per causa in un’area della Campania con numerose discariche di rifiuti. Epidemiol Prev 28(6):311–321
Biggeri A, Catelan D (2005) Mortalità per linfoma non Hodgkin e sarcomi dei tessuti molli nel territorio circostante un impianto di incenerimento di rifiuti solidi urbani. Campi Bisenzio (Toscana, Italia) 1981–2001. Epidemiol Prev 29(4–5):156–159
Biggeri A, Barbone F, Lagazio C, Bovenzi M, Stanta G (1996) Air pollution and lung cancer in Trieste, Italy: spatial analysis of risk as a function of distance from sources. Environ Health Perspect 104:750–754
Boyle E, Johnson H et al (2004) Congenital anomalies and proximity to landfill sites. Ir Med J 97(1):16–18
Castilla E, Mastroiacovo P et al (2008) Sirenomelia and cyclopia cluster in Cali, Colombia. Am J of Med Genet Part A 146(20):2626–2636
Comba P, Ascoli V, Belli S, Benedetti M, Gatti L, Ricci P, Tieghi A (2003) Risk of soft tissue sarcomas and residence in the neighborhood of an incinerator of industrial wastes. Occup Environ Med 60:650–683
Comba P, Bianchi F, Fazzo L, Martina L, Menegozzo M, Minichilli F, Mitis F, Musmeci L, Pizzuti R, Santoro M, Trinca S, Martuzzi M (2006) Cancer mortality in an area of Campania (Italy) characterized by multiple toxic dumping sites. Ann NY Acad Sci 1076:449–461
Cordier S, Chevrier C, Robert-Gnansia E, Lorente C, Brula P, Hours M (2004) Risk of congenital anomalies in the vicinity of municipal solid waste incinerators. Occup Environ Med 61:8–15
Cordier S, Lehebel A et al (2010) Maternal residence near municipal waste incinerators and the risk of urinary tract birth defects. Occup Environ Med 67(7):493–499
Cresswell PA, Scott JES et al (2003) Risk of congenital anomalies near the Byker waste combustion plant. J Public Health Med 25(3):237–242
Croen LA, Shaw GM, Sanbonmatsu L, Selvin S, Bufflers PA (1997) Maternal residential proximity to hazardous waste sites and risk for selected congenital malformations. Epidemiology 8:347–354
de Wet T, Plagerson S, Harpham T, Mathee A (2011) Poor housing, good health: a comparison of formal and informal housing in Johannesburg, South Africa. Int J Public Health 56:625–633
Department for Environment, Food and Rural Affairs (DEFRA) (2004) Review of environmental and health effects of waste management: municipal solid waste and similar wastes, UK 2004. DEFRA, London
Dolk H, Vrijheid M (2003) The impact of environmental pollution on congenital anomalies. Br Med Bull 68:25–45
Dolk H, Vrijheid M, Armstrong B, Abramsky L, Bianchi F, Garne E, Nelen V, Robert E, Scott JE, Stone D, Tenconi R (1998) Risk of congenital anomalies near hazardous-waste landfill sites in Europe: the EUROHAZCON study. Lancet 352:423–427
Dummer TJB, Dickinson HO, Parker L (2003a) Adverse pregnancy outcomes around incinerators and crematoriums in Cumbria Northwest England, 1956–1993. J Epidemiol Commun Health 57:456–461
Dummer TJB, Dickinson HO et al (2003b) Adverse pregnancy outcomes near landfill sites in Cumbria, northwest England, 1950–1993. Arch Environ Health 58(11):692–698
Elliott P, Shaddick G, Kleinschmidt I, Jolley D, Walls P, Beresford J, Grundy C (1996) Cancer incidence near municipal solid waste incinerators in Great Britain. Br J Cancer 73:702–710
Elliott P, Eaton N, Shaddick G, Carter R (2000) Cancer incidence near municipal solid waste incinerators in Great Britain. Part 2: histopathological and case-note review of primary liver cancer cases. Br J Cancer 82:1103–1106
Elliott P, Briggs D, Morris S, de Hoogh C, Hurt C, Jensen TK, Maitland I, Richardson S, Wakefield J, Jarup L (2001) Risk of adverse birth outcomes in populations living near landfill sites. Br Med J 323:363–368
Elliott P, Richardson S, Abellan JJ, Thomson A, de Hoog C, Jaruo L, Briggs DJ (2009) Geographic density of landfill sites and risk of congenital anomalies in England. Occup Environ Med 66:81–89
Fazzo L, Belli S, Minichilli F, Mitis F, Santoro M, Martina L, Pizzuti R, Comba P, Martuzzi M, Bianchi F, Working Group (2008) Cluster analysis of mortality and malformations in the Provinces of Naples and Caserta (Campania Region). Ann Ist Super Sanità 44:99–111
Fazzo L, De Santis M, Mitis F, Benedetti M, Martuzzi M, Comba P, Fusco M (2011) Ecological studies of cancer incidence in an area interested by dumping waste sites in Campania (Italy). Ann Ist Super Sanità 47:181–191
Federico M, Pirani M et al (2010) Cancer incidence in people with residential exposure to a municipal waste incinerator: an ecological study in Modena (Italy), 1991–2005. Waste Manag 30(7):1362–1370
Fielder HMP, Poon-King CM et al (2000) Assessment of impact on health of residents living near the Nant-y-Gwyddon landfill site: retrospective analysis. Br Med J 320(7226):19–22
Fielder HMP, Palmer SR et al (2001) Addressing environmental health concerns near Trecatti Landfill Site, United Kingdom. Arch Environ Health 56(6):529–553
Floret N, Mauny F, Challier B, Arveux P, Cahn JY, Viel JF (2003) Dioxin emissions from a solid waste incinerator and risk of non-Hodgkin lymphoma. Epidemiology 14:392–398
Floret N, Mauny F et al (2004) Dioxin emissions and soft-tissue sarcoma: results of a population-based case-control study. Rev Epidemiol Sante Publique 52(3):213–220
Forastiere F, Badaloni C et al (2011) Health impact assessment of waste management facilities in three European countries. Environ Health Glob Access Sci Sour 10(1):53
Forastiere F, Perucci CA (2008) Rifiuti, prove scientifiche e decisioni politiche: quale ruolo per l’epidemiologia. Epidemiol Prev 32(1):5–7
Franchini M, Rial M, Buiatti E, Bianchi F (2004) Health effects of exposure to waste incinerator emissions: a review of epidemiological studies. Ann Ist Super Sanita 40(1):101–115
Gensburg LJ, Pantea C et al (2009) Mortality among former Love Canal residents. Environ Health Perspect 117(2):209–216
Geschwind SA, Stolwijk J, Bracken M, Fitzgerald E, Stark A, Olsen C, Melius G (1992) Risk of congenital malformations associated with proximity to hazardous waste sites. Am J Epidemiol 195:1197–1207
Gilbreath S, Kaas PH (2006) Adverse birth outcomes associated with open dumpsites in Alaska native villages. Am J Epidemiol 164:518–528
Giusti L (2009) A review of waste management practices and their impact on human health. Waste Manage (Oxford) 29:2227–2239
Goldberg MS, Goulet L, Riberdy H, Bonvalot Y (1995) Low birth weight and preterm births among infants born to women living near a municipal solid waste landfill site in Montreal, Quebec. Environ Res 69:37–50
Goldberg MS, Siemiatyck J, DeWar R, Dèsy M, Riberdy H (1999) Risk of developing cancer relative to living near a municipal solid waste landfill site in Montreal, Quebec, Canada. Arch Environ Health 54:291–296
Gonzalez CA, Kogevinas M, Gadea E, Huici A et al (2000) Biomonitoring study of people living near or working at a municipal solid-waste incinerator before and after two years of operation. Arch Environ Health 55(4):259–267
Goria S, Daniau C et al (2009) Risk of cancer in the vicinity of municipal solid waste incinerators: importance of using a flexible modelling strategy. Int J Health Geogr 8:31
Gouveia N, Ruscitto do Prado R (2010b) Spatial analysis of the health risks associated with solid waste incineration: a preliminary analysis. Rev Bras Epidemiol 13(1):3–10
Gouveia N, Ruscitto do Prado R (2010a) Health risks in areas close to urban solid waste landfill sites. Rev Saude Publica 44(5):1–8
Hsiue TR, Lee SS, Chen HI (1991) Effects of air pollution resulting from wire reclamation incineration on pulmonary function in children. Chest 100:698–702
Hu SW, Shy CM (2001) Health effects of waste incineration: a review of epidemiological studies. J Air Waste Manag Assoc 51:1100–1109
International Agency for Research on Cancer (IARC)–WHO. http://monographs.iarc.fr/ENG/Preamble/currentb6evalrationale0706.php. Accessed 22 July 2013
Jansson B, Voog L (1989) Dioxin from Swedish municipal incinerators and the occurrence of cleft lip and palate malformations. Int J Environ Stud 34:99–104
Jarup L, Briggs D, de Hoogh C, Morris S, Hurt C, Lewin A, Maitland I, Richardson S, Wakefield J, Elliott P (2002) Cancer risks in populations living near landfill sites in Great Britain. Br J Cancer 86:1732–1736
Jarup L, Morris S, Richardson S, Briggs D, Cobley N, de Hoog C, Gorog K, Elliot P (2007) Down syndrome in births near landfill sites. Prenat Diagn 27:1191–1196
Kloppenborg SCh, Brandt UK, Gulis G, Ejstrud B (2005) Risk of congenital anomalies in the vicinity of waste landfills in Denmark; an epidemiological study using GIS. Cent Eur J Public Health 13:137–143
Knox E (2000) Childhood cancers, birthplaces, incinerators and landfill sites. Int J Epidemiol 29:391–397
Lee JT, Shy CM (1999) Respiratory function as measured by peak expiratory flow rate and PM10: six communities study. J Expo Anal Environ Epidemiol 9(4):293–299
Linzalone N, Bianchi F (2007) Incinerators: not only dioxins and heavy metals, also fine and ultrafine particles. Epidemiol Prev 31(1):62–66
Lloyd OL, Lloyd MM, Williams FL, Lawson A (1988) Twinning in human populations and in cattle exposed to air pollution from incinerators. Br J Ind Med 45:556–560
Ma J, Kouznetsova M, Lessner L, Carpenter D (2007) Asthma and infectious respiratory disease in children—correlation to residence near hazardous waste sites. Paediat Resp Rev 8:292–298
Marshall EG, Gensburg LJ, Deres DA, Geary NS, Cayo MR (1997) Maternal residential exposure to hazardous wastes and risk of central nervous system and musculoskeletal birth defects. Arch Environ Health 52(6):416–425
Martuzzi M, Mitis F, Bianchi F, Minichilli F, Comba P, Fazzo L (2009) Cancer mortality and congenital anomalies in a region of Italy with intense environmental pressure due to waste. Occup Environ Med 66(11):725–732
Michaels D, Monforton C (2005) Manufacturing uncertainty: contested science and the protection of the public’s health and environment. Am J Public Health 95(Suppl 1):S39–S48
Michelozzi P, Fusco D, Forastiere F, Ancona C, Dell’Orco V, Perucci CA (1998) Small area study of mortality among people living near multiple sources of air pollution. Occup Environ Med 55:611–615
Minichilli F, Bartolacci S, Buiatti E, Pallante V, Scala D, Bianchi F (2005) Studio di mortalità intorno a sei discariche di rifiuti in Toscana. Epidemiol Prev 29(5–6) Suppl:53–56
Miyake Y, Yura A, Misaki H, Ikeda Y, Usui T, Iki M, Shimizu T (2005) Relationship between distance of schools from the nearest municipal waste incineration plant and child health in Japan. Eur J Epidemiol 20:1023–1029
Morgan OWC, Vrijheid M et al (2004) Risk of low birth weight near EUROHAZCON hazardous waste landfill sites in England. Arch Environ Health 59(3):149–151
Morris SE, Thompson AOW et al (2003) No excess risk of adverse birth outcomes in populations living near special waste landfill sites in Scotland. Scottish Med J 48(4):105–107
Orioli IM, Mastroiacovo P, Lopez-Camelo JS, Saldarriaga W, Isaza C, Aiello H, Zarante I, Castilla E (2009) Clusters of sirenomelia in South America. Birth Defects Res A Clin Mol Teratol 85(2):112–118
Palmer SR, Dunstan FDJ et al (2005) Risk of congenital anomalies after the opening of landfill sites. Environ Health Perspect 113(10):1362–1365
Parodi S, Baldi R, Benco C, Franchini M, Garrone E, Vercelli M, Pensa F, Puntoni R, Fontana V (2004) Lung cancer mortality in a district of La Spezia (Italy) exposed to air pollution from industrial plants. Tumori 90:181–185
Porta D, Milani S et al (2009) Systematic review of epidemiological studies on health effects associated with management of solid waste. Environ Health 8:60
Pukkala E, Pönkä A (2001) Increased incidence of cancer and asthma in houses built on a former dump area. Environ Health Perspect 109:1121–1125
Ranzi A, Fano V, Erspamer L, Lauriola P, Perucci CA, Forastiere F (2011) Mortality and morbidity among people living close to incinerators: a cohort study based on dispersion modeling for exposure assessment. Environ Health. 24(10):22
Reis MF, Sampaio C, Brantes A, Aniceto P, Melim M, Cardoso L, Gabriel C, Simão F, Segurado S, Miguel JP (2007) Human exposure to heavy metals in the vicinity of Portuguese solid waste incinerators. Int J Hyg Environ Health 210(3–4):447–454, 439–446, 455–459
Rushton L (2003) Health hazards and waste management. Br Med Bull 68:183–197
Russi MB, Borak JB, Cullen MR (2008) An examination of cancer epidemiology studies among populations living close to toxic waste sites. Environ Health 26:7–32
Shy CM, Degnan D, Fox DL, Mukerjee S, Hazucha MJ, Boehlecke BA, Rothenbacher D, Briggs PM, Devlin RB, Wallace DD, Stevens RK, Bromberg PA (1995) Do waste incinerators induce adverse respiratory effects? An air quality and epidemiological study of six communities. Environ Health Perspect 103:714–724
Signorelli C, Riccò M, Vinceti M (2008) Inceneritori e rischi per la salute umana: lo stato dell’arte. Ann Ig 20:251–277
Tango T, Fujita T, Tanihata T, Minowa M, Doi Y, Kato N, Kunikane S, Uchiyama I, Tanaka M, Uehata T (2004) Risk of adverse reproductive outcomes associated with proximity to municipal solid waste incinerators with high dioxin emission levels in Japan. J Epidemiol 14:83–93
ten Tusscher GW, Stam GA et al (2000) Open chemical combustions resulting in a local increased incidence of orofacial clefts. Chemosphere 40(9–11):1263–1270
Viel JF, Arveux P, Baverel J, Cahn JY (2000) Soft-tissue sarcoma and non-Hodgkin’s lymphoma clusters around a municipal solid waste incinerator with high dioxin emission levels. Am J Epidemiol 152:13–19
Viel JF, Daniau C, Goria S, Fabre P, de Crouy-Chanel P, Sauleau EA, Empereur-Bissonnet P (2008a) Risk for non Hodgkin’s lymphoma in the vicinity of French municipal solid waste incinerators. Environ Health 7:51. doi:10.1186/1476-069X-7-51
Viel JF, Clément MC, Hägi M, Grandjean S, Challier B, Danzon A (2008b) Dioxin emissions from a municipal solid waste incinerator and risk of invasive breast cancer: a population-based case-control study with GIS-derived exposure. Int J Health Geogr 7:4
Vinceti M, Malagoli C et al (2008) Adverse pregnancy outcomes in a population exposed to the emissions of a municipal waste incinerator. Sci Total Environ 407(1):116–121
Vrijheid M (2000) Health effects of residence near hazardous waste landfill sites: a review of the epidemiological literature. Environ Health Perspect 108(suppl I):101–112
Vrijheid M, Dolk H et al (2002) Hazard potential ranking of hazardous waste landfill sites and risk of congenital anomalies. Occup Environ Med 59(11):768–776
WHO, Regional Office for Europe, Copenhagen (2007) Population health and waste management: scientific data and policy options. In: Mitis F, Martuzzi M (eds) Report of a WHO workshop Rome, Italy, 29–30 March 2007. WHO Regional Office for Europe, Copenhagen
Williams A, Jalaludin B (1998) Cancer incidence and mortality around a hazardous waste depot. Aust N Z J Publ Health 22(3 Suppl):342–346
Williams FL, Lawson AB, Lloyd OL (1992) Low sex ratios of births in areas at risk from air pollution from incinerators, as shown by geographical analysis and 3-dimensional mapping. Int J Epidemiol 21:311–319
Zambon P, Ricci P, Bovo E, Casula A, Gattolin M, Fiore AR, Chuiosi F, Guzzinati S (2007) Sarcoma risk and dioxin emissions from incinerators and industrial plants: a population-based case-control study (Italy). Environ Health 6:19
Acknowledgments
We thank Vanna Pistotti for library search strategies and Francesco Forastiere, Pietro Comba, Ennio Cadum, Andrea Ranzi, Carla Ancona, and Fabrizio Bianchi for comments and suggestions. The authors declare their full responsibility for the production, analysis, and interpretation of the results and the conclusions of the systematic review. This review has been made possible through a grant from the Regione Campania Authority addressed by the Center for Disease Control of the Italian Ministry of Health.
Conflict of interest
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the special issue “Environment and Health Reviews”.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Mattiello, A., Chiodini, P., Bianco, E. et al. Health effects associated with the disposal of solid waste in landfills and incinerators in populations living in surrounding areas: a systematic review. Int J Public Health 58, 725–735 (2013). https://doi.org/10.1007/s00038-013-0496-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-013-0496-8