
Abstract
Objectives
The study covers development and evaluation of an innovative counselling aid in an intervention study. The main purpose of the study was to establish whether improvements in nutrition and physical activity behaviour according to standard recommendations can be demonstrated.
Methods
OPTIMAHL 60plus is a quasi-experimental study in which participants were assigned in clusters to an intervention or control group. The study was conducted in low socio-economic-status districts in Bremen, Germany. 423 elderly participated at baseline and 369 after 3 months intervention. Face-to-face interviews (24-h recall and frequency questionnaire) were conducted at T0 and T1. χ 2-tests, sign-test and logistic regression were used for statistical analyses.
Results
No significant differences could be shown when comparing the intervention versus control group at T1. Significant changes from T0 to T1 in the intervention group were identified for daily fruit and vegetable (χ 2-test, p = 0.04), and for weekly fish consumption (χ 2-test, p = 0.04). However, similar results could also be shown for the control group.
Conclusions
A practical counselling aid for elderly was developed and evaluated. Changes in the health behaviour of elderly were identified, but effects could not be clearly traced to the intervention.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The OPTIMAHL 60plus study aims to optimise the nutrition and physical activity (PA) behaviour of elderly people. Furthermore, the intention of the study is to maintain and enhance the quality of life as well as to increase the autonomy of this group (Dreas et al. 2009). It is often difficult to ensure a balanced diet in elderly. There are deficits in the consumption of vegetables and fruits, fish and dairy (-products). Nutrient supply is also insufficient and particularly folic acids, vitamin D and calcium are not regularly consumed (Fabian and Elmadfa 2008). Folic acids from fruits and vegetables as well as vitamin B12 are responsible for the decomposition of homocysteine. A high level of homocysteine was described as a risk factor for the development of cardiovascular diseases (Weikert et al. 2005).
Vitamin D and calcium play a vital role in the prevention of osteoporosis. Vitamin D is built under sunlight exposure and from vitamin D rich foods like fatty saltwater fish. Since elderly on average spend less time outdoors, the supply of vitamin D through food is especially important. The calcium contained in dairy (-products) is also important to preserve bone density (Deutsche Gesellschaft für Ernährung et al. 2001; Morgan 2008).
Physical activity and physical capability are not only preventive factors in relation to the preservation of the bone density. Cardiovascular and musculoskeletal diseases including falls can be prevented by regular physical activity (American College of Sports Medicine 1998; Stewart 2005; Tinetti et al. 1994; Tinetti 2003; WHO 1998; Williamson et al. 2009).
In addition, studies mainly from Scandinavia document that the morbidity of elderly is influenced by a positive change of the physical activity behaviour. Interventions focusing on physical activity can optimise the muscle function, the control over body posture and the speediness of walking (Howe et al. 2007; Karinkanta et al. 2007; Latham et al. 2004). Being physically active also has psychological and mental benefits as it helps in maintaining or even increasing autonomy and competency until old age (Akbaraly et al. 2009; Anderson et al. 2010; Voelcker-Rehage et al. 2005).
To improve the physical activity and nutrition behaviour of elderly people, an interdisciplinary counselling aid was developed in a participatory way together with the target group. Elderly participants (with and without migration background) discussed various types of counselling aids specifically developed for the OPTIMAHL 60plus study in focus groups. The preferred counselling aid was improved and again tested for easy understanding in focus groups with elderly persons (Hassel et al. 2010). A picture of the counselling aid can be found in Keimer et al. (2011). In a second step, the effectiveness of this counselling aid was evaluated in a quasi-experimental study. The counselling aid covers fruit and vegetable (FV), dairy (-products) (D) and fish (F) consumption as well as physical activity (PA), and includes feedback on target and daily performance and advice for improvement. The concept of the counselling aid is based on the self-regulation model by Kanfer (1977). The handling of the aid is very easy: whenever the participant has consumed one serving of, e.g., vegetables, he/she can tick one of the circles in the first column. At the end of the day, the participant receives a graphical feedback on his/her daily performance through the comparison with recommendations and knows which of the four aspects still needs improvement. The aid can be wiped off using a wet tissue and can then be re-used the next day.
Due to their complexity, already existing didactical counselling aids for behaviour change in nutrition and physical activity are not considered eligible for the target group of elderly people (Murphy and Barr 2007; Park Nicollet Health Source 2009; Reinhardt and Brevard 2002; Stehle et al. 2005; US Department of Agriculture 1992; US Department of Agriculture 2009).
Four main hypotheses were formulated. These hypotheses considered a significant increase in the four main health topics concerning the consumption of (1) fruits and vegetables, (2) dairy products, (3) fish, and (4) the minutes of daily physical activity in the intervention group.
In this paper, the results of the outcome evaluation (T0–T1) will be described, some basic results of T2 are included and the strengths and limitations of the study will be discussed.
Methods
Design
The study was conducted between 2007 and 2009 in low socio-economic status (SES) districts in the city of Bremen, Germany. The baseline survey (T0) took place in September 2008 and the first follow-up (T1) in December 2008/January 2009. A second follow-up (T2) took place in June/July 2009. The focus of our analyses is on a T0–T1 comparison, as this was the basis of our power calculation (see below).
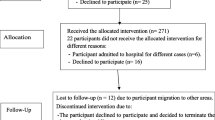
Inclusion criteria were age 57 years and above and the ability to care for oneself. Participants were recruited on a voluntary basis in cooperation with several community partners. The recruitment took place in the community partners’ institutions or in church groups. Elderly with migration background were recruited through visits to mosques and with the assistance of the Center for Migrants and Intercultural Studies (ZIS). In addition, 139 participants were recruited through press releases. 51 of these were assigned to the intervention and 88 to the control group to reach the required sample size in both groups. Neighbourhoods with low SES were identified through an existing social index. The social index for Bremen indicates disadvantaged neighbourhoods according to 24 social indicators such as percentage of migrants, percentage of unemployment and percentage receiving welfare support (Der Senator für Arbeit, Frauen, Jugend, Gesundheit und Soziales 2006). We paid special attention to the inclusion of meeting places and churches/mosques in the 29 most disadvantaged districts (of a total of 79 listed).
Participants were recruited in groups and assigned to the intervention or control group according to districts.
The statistical power calculation was based on the comparison of two equally sized groups (170 participants in control and intervention group each). We assumed a positive behaviour change of ~5 % in the control group. Using a global level of significance of α = 5 %, a positive behaviour change of 15 % in the intervention group should be detected at a power of 80 % (β = 0.2). Based on these assumptions, 170 elderly were needed in the intervention and control group, respectively.
According to standard (international) guidelines displayed on the counselling aid, a daily intake of five servings of FV, three servings of D per day, one serving of F per week plus 30 min of moderate to vigorous PA per day is recommended (DGE et al. 2001; DiPietro 2001; WHO 2009). As recommended by the German Nutrition Society (DGE), the servings of FV, D and F were measured as the participant’s handful. To clarify the PA intensity to participants, we used a Borgscale (Borg 1985) from 1 to 10, where 10 is the most vigorous activity.
Sample characteristics
In total 481 elderly consented to participate. Of these, 423 (329 women, 94 men) aged 57–95 years fulfilled the inclusion criteria. After the three-month follow-up, 369 participants (293 women, 76 men) remained in the study for T1. The 54 persons who dropped out between T0 and T1—38 (17.4 %) from the intervention and 16 (7.8 %) from the control group—were excluded from data analyses. The remaining participants were aged between 57 and 93 years and 180 were in the intervention group and 189 in the control group. 247 participants (208 women, 39 men) remained in the study for T2—133 in the intervention and 114 in the control group. Baseline comparisons were conducted using the Wilcoxon-test (see Table 1).
Intervention
The intervention in OPTIMAHL 60plus was carried out over a three-month period from September until December 2008. Participants in the intervention group were invited to regular meetings in easily reachable meeting places such as community partners’ institutions, churches and mosques. In total, the intervention comprised seven sessions in small groups of generally 6–10 elderly and lasted 45–60 min. During the first session, a detailed explanation of the counselling aid was given. In each session, the elderly discussed health topics related to the counselling aid. Standard health information on PA and nutrition and cooking recipes were handed out at the end of each session. All meetings were led by trained moderators.
The control group had no meetings but received the standard health information and cooking recipes by post. The health information followed the international recommendations on healthy eating and physical activity (DGE et al. 2001; DiPietro 2001; WHO 2006). The participants in the control group received the counselling aid after the study had ended. All material was available in German, Turkish and Russian, to make sure the study is understood by all participants from different ethnic backgrounds. In addition, the intervention group meetings were translated into Russian or Turkish, if necessary.
Measures and analysis strategy
Nutrition and physical activity behaviour was measured in the control and the intervention group at three different points in time: baseline survey (T0), after three months (T1) and at nine-month follow-up (T2). This paper reports the detailed results of T0 and T1 and gives an overview of T2 results. Face-to-face interviews were conducted by trained interviewers using a standardised instrument. Nutrition and PA behaviour was measured by 24-h recall and frequency questionnaire (FQ). In this paper, we focus on the results of the 24-h recall when suitable (for FV, D and PA) and use data from the FQ only if necessary as the potential for bias is larger in the latter.
For preliminary analyses, a \( \chi^{2} \) test (α = 0.05) was used to compare categories of consumed servings in the intervention and control group at T0, T1 and T2, which were classified according to the health recommendations. For the main analysis we initially considered the changes (difference in number of servings and difference in minutes of being physically active) between T0 and T1 and performed a two-sided sign-test (α = 0.05) to examine behaviour changes within both groups. To investigate the potential influence of the counselling aid in combination with the group meetings in the intervention group (independent variable) on a positive health behaviour change, i.e. increase in consumption of FV, D and F or increase in minutes of PA (as binary dependent variable), logistic regression analyses for each aspect were carried out to estimate odds ratios (OR) and 95 % confidence intervals (CI) with and without adjusting for sex, age and migration background. Analyses including the sign-test and the logistic regression were performed twice: first considering all participants and second considering a subsample where all participants who already fulfilled the health recommendations of the respective health aspect at both surveys T0 and T1 were excluded; e.g. participants who reached the recommended five servings of vegetables and fruits per day at T0 and at T1 were excluded.
The study received ethical approval through the Ethics Committee of Bremen University, Germany.
Results
The results are reported separately for the consumption of FV, D, F, and PA. Descriptive comparisons of intervention and control groups are followed by a group comparison at T0, T1 and T2 using a \( \chi^{2} \) test. Thereafter, results of the changes over time from T0 and T1 in the intervention and control group are presented. A comparison of the sign-test (M) and regression analyses results for all four health aspects is provided in Table 2. We performed subsample analyses for exploratory purposes. The subsample analyses serve to identify trends that need further investigation in the future.
Fruits and vegetables
Overall daily mean consumption of FV was 2.9 servings at T0 and 3.3 at T1 with minor differences between the control and intervention group. In total 71 participants (19.2 %) reached the recommended level of five servings/day (DGE et al. 2001) at T0 and 94 participants (25.5 %, + 5.9 %) at T1. For the intervention and control group the numbers were 34 (18.9 %) and 37 (19.6 %) at T0 and 49 (27.2 %; + 8.3 %) and 45 (23.8 %; + 4.2 %) at T1, respectively.
This change from T0 to T1 was statistically significant in both groups (\( \chi^{2} \) test, p = 0.04) (see Fig. 1).

Consumption of fruits and vegetables in the intervention (IG) and control group (CG) T0–T1 (24-h recall) in the study OPTIMAHL 60plus, Bremen (Germany), 2007–2009
This result was replicated using the sign-test (intervention group M = 20.5, p < 0.001; control group M = 14.5, p = 0.019) (Table 2). However, when comparing consumption of servings of intervention versus control group at both time points using a \( \chi^{2} \) test, no significant differences could be detected (Table 3). Similarly, at T2 no significant differences in the consumption of servings of FV in the intervention versus control group were seen (χ 2-test, p = 0.37). Using a multivariate regression analysis, no significant difference in the frequency of a positive behaviour change in the intervention versus the control group could be identified (OR = 1.23, CI = 0.81–1.84) even after adjusting for demographic variables (sex, age and migration background) (OR = 1.29, CI = 0.84–1.96). As in the full sample, the \( \chi^{2} \) test results of the subsample indicated statistically significant changes for the intervention and control group. Again, the regression results for the subsample were also not different (see Table 2).
Dairy products
Overall daily mean consumption of dairy products (including milk) was two servings at both time points, with minor differences between the intervention and the control group.
A total of 143 participants (38.8 %), 76 participants (42.2 %) in the intervention and 67 (35.4 %) in the control group reached the recommended level of three servings/day (DGE et al. 2001) at T0. At T1 the overall number of participants reaching the recommendations increased to 146 participants (39.6 %, + 0.8 %): 76 (42.2 %) in the intervention and 70 (37 %, +1.6 %) in the control group (Table 3). As expected, the \( \chi^{2} \) test comparing intervention with control group at both time points showed no differences (Table 3). T2 results showed no differences either (p = 0.08).
The results of the time trend (T0–T1) showed neither in the intervention group (\( \chi^{2} \) test, p = 0.13) nor in the control group (\( \chi^{2} \) test, p = 0.39) statistically significant results. Similarly, the sign-test as well as the logistic regression showed no significant differences in the groups (Table 2 for complete data).
Similar to the results reported above, the subsample analyses, using a logistic regression analysis, indicated a non-significant 32 % increase in dairy product consumption of the intervention group subsample (Table 2).
Fish
At T0 a total of 294 (79.7 %) participants reached the recommended one serving/week (DGE et al. 2001), 147 (81.7 %) in the intervention group and 147 (77.8 %) in the control group. There was a slight consumption increase from T0 to T1 in both groups where 327 (88.6 %, + 8.9 %) persons reached the recommended level: 90.6 % (+ 8.9 %) in the intervention group and 86.6 % (+ 8.8 %) in the control group.
This change from T0 to T1 was statistically significant in both the intervention group (\( \chi^{2} \) test, p = 0.04) and the control group (\( \chi^{2} \) test, p = 0.05) (see Fig. 2), with slightly different results when the sign-test was used (intervention group M = 99.5, p < 0.01; control group M = 7, p = 0.07). However, the comparison of changes in the intervention versus the control group using multivariate regression analysis indicated no differences (Table 2), similar to results obtained from \( \chi^{2} \) tests (Table 3). When only the restricted sample after exclusion of participants already reaching the recommended servings at both time points was analysed, the results remained essentially unchanged. When looking at the \( \chi^{2} \) test results at T2 (intervention vs. control group), no differences could be detected (χ 2-test, p = 0.99).

Consumption of fish in the intervention (IG) and control group (CG) T0–T1 (Food Frequency Questionnaire) in the study OPTIMAHL 60plus, Bremen (Germany), 2007–2009
Physical Activity
The recommendation for physical activity is 30 min/day with a moderate to vigorous intensity (DiPietro 2001; WHO 2006). Overall mean duration in this sample was 172.9 min (167.6 min for the intervention and 178.1 min for the control group) at T0. The mean duration decreased for all groups at T1—to 157.1 min for the whole sample and 153.7 min in the intervention group. The mean duration decreased to 160.4 in the control group. It was interesting to see that over 90 % of participants in both groups at T0 as well as at T1 reached 30 min/day, but not with the required intensity level.
Comparing the minutes of PA for both groups at T0 and at T1, the results were non-significant (T0: χ 2-test, p = 0.41; T1: χ 2-test, p = 0.47) (Table 3). The same is true for the results at T2 (χ 2-test, p = 0.61). The results of the time trend (T0–T1) were also non-significant in intervention (χ 2-test, p = 0.73) and control group (χ 2-test, p = 0.11).
Similarly, when looking at the change of intensity level from T0 to T1, the results of the χ 2-test showed non-significant values in both group (intervention group: p = 0.91; control group: p = 0.16).
Detailed analyses related to PA using the sign-test and the logistic regression are included in Table 2. Overall, physical activity was not affected by the intervention, however, the relatively high levels of any activity in the study population are noteworthy.
Discussion
In a participatory process, we developed a simple counselling aid for elderly people and evaluated its effects in a controlled interventional study design.
The results generally do not show any significant differences in the health behaviour change between intervention and control groups. Significant within group changes were seen in the consumption of fruit and vegetables as well as in the consumption of fish, hinting towards unspecific time-dependent changes in both groups. Additionally, after adjustment for confounders, results of the logistic regression for fruit, vegetable and fish, particularly in the subsample, indicate that the frequency of behaviour change appears to be somewhat more pronounced in the intervention group than in the control group. In conclusion, the intervention using the counselling aid embedded in group meetings shows some advantages in changing the nutrition behaviour of elderly compared to the health information/cooking recipes received by the control group, which also show some positive effects on nutrition behaviour. Thus, self-regulatory measures in the form of a counselling aid (intervention group) or as health information (control group) may maintain or even increase autonomy and competency in old age. Further studies need to be undertaken to exactly identify study components which are most effective.
The tendencies to improve the nutritional behaviour in the intervention and control group from T0 to T1 might be due to the distributed health information, which implicitly included the recommended numbers of servings/minutes of PA per day. We expected that the information would also have some effect on the health behaviour in the control group. However, we believed that the use of the counselling aid in combination with motivational intervention meetings would result in greater effects, which was partially confirmed by our study. This assumption was based on previous studies in which community-based interventions are described as effective in changing health behaviour (Fitzpatrick et al. 2008; Hendrix et al. 2008; Karinkanta et al. 2007; Pomerleau et al. 2005).
The results of T2 have to be considered with care, since the sample size of n = 133 in the intervention and n = 114 in the control group does not reach the necessary n = 170 as defined by the power calculation. Nevertheless, the T2 results support those of the T0–T1 comparisons, at least for the analyses undertaken so far.
Strengths and limitations of this study
The first limitation is related to the recruitment in OPTIMAHL 60plus. The short period of time for recruitment (Keimer et al. 2011) led us to target elderly also through the media (press release). The optimisation of health behaviour in both groups may thus also be due to selection bias. Almost two-thirds of the 139 participants recruited via the press were assigned to the control group (see Table 1). The control group could have had more interested and more mobile participants, which may have caused greater behaviour improvements from T0 to T1. However, a sensitivity analysis showed that there were no differences in the health behaviour at baseline (T0) or a better improvement at follow-up (T1).
Second, women were over-represented in the study with n = 293. One reason for this may be that women tend to be more interested in (nutrition) behaviour change studies (Kolip and Altgeld 2006). Third, for physical activity the behaviour change results were not clear. When looking at the duration of being physically active/day, over 90 % of participants were at least 30 min physically active. Besides sports activities, this variable also included household activities, walking (up- and downstairs) and grocery shopping. However, the recommended level of moderate to vigorous PA was not reached. There are several explanations for this: in the 24-h recall related to PA we asked participants about eight types of activity during the previous day at five time points during the day, where they had to additionally report the perceived intensity—which was complex and time-consuming. It is also possible that the subjective impression of moderate to vigorous activity in this age group was not accurately assessed using a 24-h recall or PAFQ. Another reason for the little increase in the duration of minutes of PA per day from T0 to T1 could be that the intervention is better at improving the eating behaviour in elderly but not so much the PA duration and intensity. Intervention studies providing a more active PA component may show clearer results (Fitzpatrick et al. 2008).
Fourth, contamination between intervention and control groups is often a problem in intervention studies. For OPTIMAHL 60plus, the intervention and control districts were chosen, so that they are not located directly next to each other, thereby reducing the potential for contamination between the two groups. In addition, we felt it reasonable to assume that most elderly people stay in their residential districts of the city, where they have their daily living arrangements and their social network.
There are also several strengths of the OPTIMAHL 60plus study. One of the strengths relates to the study design: it was a well implemented intervention programme in a community setting, which has been identified as a fruitful and effective health promotion strategy (Keller et al. 2004).
Second, the counselling aid was designed as a self-regulatory tool. Hence, the focus of this aid lies on empowerment rather than help from outside. We assumed that with this underlying principle, the effects could be sustainable. This is being examined in further analyses.
Third, the OPTIMAHL 60plus study adds the development of a unique and innovative counselling aid for elderly (Hassel et al. 2010), which has been identified in this study as useful and acceptable for the participants. Due to its success in the study, the counselling aid was further developed adding the component of beverages and is now distributed by the consumer advice centres in Germany to 10.000 elderly per year.
Conclusion
Within OPTIMAHL 60plus an easy to understand and innovative counselling aid to improve the health behaviour of elderly was developed. Already existing counselling aids, like the food pyramid, are not suitable for this age group since they are too complex (Hassel et al. 2010).
The study shows that an intervention does not necessarily need to be complex. The use of standard health information sent by post may be sufficient for some groups to change their health behaviour.
Based on our work, we recommend to involve the target group (of elderly in our case) when developing a tool to help change the participants’ nutrition and PA behaviour. Thus, tools that are acceptable for and understood by the target groups can be employed in research, and potentially transferred into practice, as successfully demonstrated following our study.
References
Akbaraly TN, Portet F, Fustinoni S, Dartigues JF, Artero S, Rouaud O, Touchon J, Ritchie K, Berr C (2009) Leisure activities and the risk of dementia in the elderly: results from the Three-City Study. Neurology 73:854–861
American College of Sports Medicine (1998) American College of Sports Medicine Position Stand. Exercise and physical activity for older adults. Med Sci Sports Exerc 6:992–1008
Anderson F, Annett M, Bischof WF (2010) Lean on Wii: physical rehabilitation with virtual reality Wii peripherals. Stud Health Technol Inform 154:229–234
Borg G (1985) An introduction to Borg’s RPE-scale. Movement, Ithaca
Der Senator für Arbeit Frauen Gesundheit Jugend und Soziales (2006) Sozialindikatoren 2005 [Social Indicators 2005]. Report No. 7. Bremen
Deutsche Gesellschaft für Ernährung (DGE), Österreichische Gesellschaft für Ernährung (ÖGE), Schweizerische Gesellschaft für Ernährung (SGE), Schweizerische Vereinigung für Ernährung (SVE) (2001) Referenzwerte für die Nährstoffzufuhr [Reference Values for Nutrient Supply], 1st edn. Umschau Buchverlag, Frankfurt/Main
DiPietro L (2001) Physical activity in aging: changes in patterns and their relationship to health and function. J Gerontol A Biol Sci Med Sci 56(2):13–22
Dreas JA, Boeckmann M, Keimer KM (2009) Optima(h)l 60plus. Besser essen und leben im Alter. Die Entwicklung und Erprobung einer Beratungshilfe zur Optimierung des Ernährungs- und Bewegungsverhaltens bei Menschen über 60 Jahre. [Optima(h)l 60 plus. development and test of an instrument for the elderly for an autonomous optimisation of nutrition and physical activity behavior.]. Ernährung und Medizin 24(3):119–122
Fabian E, Elmadfa I (2008) Nutritional situation of the elderly in the European Union: data of the European Nutrition and Health Report (2004). Ann Nutr Metab 52(Suppl 1):57–61
Fitzpatrick SE, Reddy S, Lommel TS et al (2008) Physical activity and physical function improved following a community-based intervention in older adults in Georgia senior centers. J Nutr Elder 27(1–2):135–154
Hassel H, Schulte B, Keimer KM (2010) Participatory development of an instrument for the elderly for an autonomous optimisation of their nutrition and physical activity profile. Health Educ J 69(3):353–361
Hendrix SJ, Fischer JG, Reddy RD et al (2008) Fruit and vegetable intake and knowledge increased following a community-based intervention in older adults in Georgia senior centers. J Nutr Elder 27(1–2):155–178
Howe TE, Rochester L, Jackson A, Banks PM, Blair VA (2007) Exercise for improving balance in older people. Cochrane Database Syst Rev (4):CD004963
Kanfer FH (1977) The many faces of self-control, or behavior modification changes its focus. In: Stuart RB (ed) Behavioral self-management. Brunner/Mazel, New York, pp 1–48
Karinkanta S, Heinonen A, Sievanen H et al (2007) A multi-component exercise regimen to prevent functional decline and bone fragility in home-dwelling elderly women: randomized, controlled trial. Osteoporos Int 18(4):453–462
Keimer KM, Dreas JA, Hassel H (2011) Recruiting elderly with a migration and/or low socio-economic status in the intervention study OPTIMAHL 60plus. J Prim Prev 32(1):53–63
Keller LO, Strohschein S, Lia-Hoagberg B, Schaffer MA (2004) Population-based public health interventions: practice-based and evidence-supported. (Part I). Public Health Nurs 21(5):453–468
Kolip P, Altgeld T (2006) Geschlechtergerechte Gesundheitsförderung und Prävention. Theoretische Grundlagen und Modell guter Praxis [Gender Specific Health Promotion and Prevention. Theoretical Basics and Models of Good Practice]. Juventa, Weinheim
Latham NK, Bennett DA, Stretton CM, Anderson CS (2004) Systematic review of progressive resistance strength training in older adults. J Gerontol A Biol Sci Med Sci 59(1):48–61
Morgan KT (2008) Nutritional determinants of bone health. J Nutr Elder 27(1–2):3–27
Murphy SP, Barr SI (2007) Food guides reflect similarities and differences in dietary guidance in three countries (Japan, Canada, and the United States). Nutr Rev 65(4):141–148
Park Nicollet Health Source (2009) The activity pyramid. http://www.ncescatalog.com/shopexd.asp?id=74. Accessed 14 Sept 2011
Pomerleau J, Lock K, Knai C, McKee M (2005) Interventions designed to increase adult fruit and vegetable intake can be effective: a systematic review of the literature. J Nutr 135(10):2486–2495
Reinhardt WC, Brevard PB (2002) Integrating the Food Guide Pyramid and Physical Activity Pyramid for positive dietary and physical activity behaviors in adolescents. J Am Diet Assoc 102(Suppl 3):S96–S99
Stehle P, Oberritter H, Büning-Fesel M, Heseker H (2005) Grafische Umsetzung von Ernährungsrichtlinien - traditionelle und neue Ansätze [Graphic Translations of Nutrition Guidelines- Traditional and New Approaches]. Ernährungsumschau 52(4):128–135
Stewart KJ (2005) Physical activity and aging. Ann N Y Acad Sci 1055:193–206
Tinetti ME (2003) Clinical practice. Preventing falls in elderly persons. N Engl J Med 348(1):42–49
Tinetti ME, Baker DI, McAvay G et al (1994) A multifactorial intervention to reduce the risk of falling among elderly people living in the community. N Engl J Med 331(13):821–827
US Department of Agriculture (USDA) (1992) The food guide pyramid. A guide to daily food choices. Home and Garden Bulletin 252:1–2
US Department of Agriculture (USDA) (2009) My pyramid. http://www.mypyramid.gov/index.html. Accessed 17 Sept 2010
Voelcker-Rehage C, Godde B, Staudinger UM (2005) Bewegung, körperliche und geistige Mobilität im Alter [Activity, physical and psychological mobility in old age]. Bundesgesundheitsbl-Gesundheitsforsch-Gesundheitsschutz 49:558–566
Weikert C, Hoffmann K, Dierkes J et al (2005) A homocysteine metabolism-related dietary pattern and the risk of coronary heart disease in two independent german study populations. J Nutr 135(8):1981–1988
WHO (1998) Growing older - staying well. Ageing and physical activity in everyday life. World Health Organization, Geneva
WHO (2006) Physical activity and health in Europe: evidence for action. World Health Organization, Copenhagen
WHO (2009) Global strategy on diet, physical activity and health. http://www.who.int/dietphysicalactivity/pa/en/index.html. Accessed 14 Sept 2011
Williamson JD, Espeland M, Kritchevsky SB et al (2009) Changes in cognitive function in a randomized trial of physical activity: results of the lifestyle interventions and independence for elders pilot study. J Gerontol A Biol Sci Med Sci 64(6):688–694
Acknowledgments
This study was funded by the Federal Ministry of Education and Research (BMBF) in Germany [01 EL 0703]. The information in this document reflects the authors’ view and is provided as is.
Conflict of interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gallois, K.M., Buck, C., Dreas, J.A. et al. Evaluation of an intervention using a self-regulatory counselling aid: pre- and post- intervention results of the OPTIMAHL 60plus study. Int J Public Health 58, 449–458 (2013). https://doi.org/10.1007/s00038-012-0420-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-012-0420-7