
Abstract
Objective
Because public health funds are limited, programs need to be prioritized.
Methods
We used data on 15 risk factors from Italy’s public health surveillance to inform prioritization of programs. We ranked risk factors using a score based on the product of six criteria: deaths attributable to risk factors; prevalence of risk factors; risk factor prevalence trend; disparity based on the ratio of risk factor prevalence between low and high education attainment; level of intervention effectiveness; and cost of the intervention.
Results
We identified seven priorities: physical inactivity; cigarette smoking (current smoking); ever told had hypertension; not having blood pressure screening; ever told had high cholesterol; alcohol (heavy drinking); not eating five fruits and vegetables a day; and not having a fecal occult blood test.
Conclusions
This prioritization method should be used as a tool for planning and decision making.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A prioritization process should be used to help decide how to fund public health programs because of resources constraint (Vilnius and Dandoy 1990). There are approaches to prioritize public health programs that measure burden of disease (Hanlon and Pickett 1979), cost-benefit, or effectiveness ratios (Coffield et al. 2001), whereas other approaches use risk factors directly or indirectly as a basis to estimate disease burden (Weinstein and Stason 1977).
In the past 20 years, with the growing importance of non-transmissible diseases (NTD) and development of NTD risk factors surveillance in the United States (US) and other countries (Mokdad et al. 2003; Baldissera et al. 2011; Moura et al. 2008) planners have begun to use risk factors to set public health priorities (Murray and Lopez 1997).
Nevertheless, there are no published examples of local or regional priority setting that uses the burden methodology; most applications used national or global data (Murray and Lopez 1997). There are several reasons for this gap. First, these methods require complex data and statistical applications (e.g., integral equations and Markov models) not commonly available at public health departments (Murray and Lopez 1997; Muennig et al. 2010). Second, most health surveillance tracks categorical risk factors (e.g., smoking yes/no) and preventive/risk factors in primary (e.g., dietary fat,), secondary (e.g., blood cholesterol screening), or tertiary prevention (e.g., hypercholesterolemia) while the methodology requires interval variables and primary risk factors. Third, although public health guides recommend implementation of effective and low-cost interventions (Zaza et al. 2005), there are few explicit, health economic prioritization methods published (Weinstein and Stason 1977). Furthermore, although addressing health disparities is a critical goal of public health programs and routinely tracked (Healthy People 2010), it has not been included in the published prioritization methods.
Finally, most published prioritization approaches rely on a single criterion, such as attributable burden. Yet, policy makers at the local level prefer priority setting and decision making based on many criteria (Baltussen and Niessen 2006). Thus, public health agencies need a prioritization process that uses risk factor surveillance data directly, acceptable policy criteria, and is simple to understand and apply (Rooney and Thompson 2009; Baldissera et al. 2011).
In this paper, we used data from Italian public health surveillance (Baldissera et al. 2011; ISTAT 2003, 2006) and a modification of the risk factor priority model (Simoes et al. 2006) to inform prioritization of chronic disease programs in Italy.
Methods
Model
There are 15 risk factors being compared for their priority in public health by applying the risk factor priority model in Italy: cigarette smoking (current smoking); alcohol (heavy drinking); physical inactivity (insufficient active and inactive); not eating five fruits and vegetables a day; overweight and obesity (with categories based on a BMI threshold); ever told had diabetes; ever told had hypertension; ever told had high cholesterol; not having blood pressure screening (prior 2 years); not having cholesterol screening (never); not having a mammography (prior 2 years); not having cervical screening (prior 3 years); not having a rectosigmoidoscopy (prior 5 years); not having a fecal occult blood test (FOBT) (prior 5 years); and not using a front or back seat belt. We used these risk and protective factors because of their known contribution to reducing the burden of disease and for their data availability in the Italian risk factor surveillance system.
The risk factor priority model comprises six criteria: severity (deaths attributable to risk factors); magnitude (prevalence of risk factors); urgency (risk factor prevalence trend); health disparity based on one social determinant factor (risk factor prevalence ratios for those having achieved less than high school vs. with a high school education or more); level of effectiveness of interventions to reduce a risk factor (absolute change in the prevalence of the risk factor attributed to a public health intervention); and cost of this intervention (public health resources only). This prioritization model modulates the severity criterion by comprehensively incorporating the other five criteria in terms of a multiplicative final score.
Severity criterion
The severity criterion is estimated by the population attributable mortality in 2007. We used prevalence of risk factors from the following: 2007–2009 Risk Behavior Survey PASSI (Baldissera et al. 2011); Italian Health Status and Use of Health Services Survey—ISTAT 2000 and 2005 (ISTAT 2003, 2006); and the relative risk of one or more diseases associated with a risk factor from peer-reviewed publications (Danaei et al. 2009) to generate population attributable fractions (PAF) estimated for age- and gender-specific subgroups (calculation spreadsheet available by author). Prevalence estimates in PASSI are only available for those aged 18- to 69-year old; thus, for calculations of PAF, the prevalence for the age groups 70–79 years and 80 years or older is assumed to be the same as in the age group 65–69 years. For calculations of PAFs of three risk factors with three or more levels, we used the following formula: PAF = (P0 + P1RR1 + P2RR2 + … + PKRRK) − 1/(P0 + P1RR1 + P2 RR2 + … + PKRRK) (Centers for Disease Control and Prevention 2006, 2007, 2010). The risk factors were: cigarette smoking that has three exposure levels (never smokers, former smokers, current smokers); alcohol that has four exposure levels (abstainers, 0–39 g, 40–59 g, 60+ g [males]; abstainers, 0–19 g, 20–39 g, 40+ g [females]); and physical inactivity that has four exposure levels (highly active, active, insufficient and inactive).
For dichotomous risk factors, we used the following PAF formula: PAF = P(RR − 1)/1 + (RR − 1) (Levin 1953). Then, PAF were multiplied by death counts estimated from 2007 Italy death records (Geodemo Istat.it. Le Tavole di mortalità 2009) for the same ICD-10 codes to generate population attributable deaths (severity criterion): AD = PAF × D; where D is the total deaths from a specific cause. For each AD value, we have estimated a standardized severity score for all 15 factors using the following formula: SevScore = AD/SD (AD); where SD (AD) is the standard deviation of AD.
Other criteria
Calculations of magnitude, urgency, and disparity criteria using prevalence estimates from PASSI 2007–2009 are restricted to ages 18–69 years. For this reason, estimates of prevalence for age group 70 years or older are the same as in age group 65–69 years.
The magnitude criterion is the prevalence of the risk factor in PASSI 2007, by age group, and by sex. A magnitude score was calculated for all 15 risk factors using the following formula: MagScore = P/SD (P); where (P) is the prevalence estimate, and SD (P) is the standard deviation of the risk factor prevalence.
The urgency criterion is the percentage change in prevalence of the risk factor between 2 years of PASSI (2007 and 2009) or ISTAT (2000 and 2005), when PASSI data were unavailable (i.e., only for “ever told had diabetes”). The percentage change score formula used for this criterion is as follows: Δ = P i + 1 − P i/P i, where P is the prevalence and “i” is the year when P is estimated. We used percentage change to create urgency scores in two ways. First, for each risk factor percentage change value, we have estimated an urgency score using the following formula: UrgScore = (1 + Δ)/SD (1 + Δ); where SD (1 + Δ) is the standard deviation of the percentage change in prevalence, plus 1 during the period. Second, we have estimated an urgency score using the following formula: UrgScore = 1 + (Δ)/SD (Δ).
The disparity criterion is the ratio of the prevalence of the risk factor in 2007 among those who did not reach a high school degree by the prevalence of the risk factor among those who reached a high school graduation or more: Disparity = P <HS/P >=HS; where P <HS is the prevalence among those with less than a high school degree, and P >=HS is the prevalence of risk factor for those with a high school or higher degree. For each prevalence value, a disparity score is created for all 15 risk factors using the following formula: DispScore = Disparity/SD (Disparity); where SD (Disparity) is the standard deviation of the disparity ratio.
The effectiveness criterion is estimated as the absolute change in the prevalence of the risk factor attributed to a public health intervention (net effect). Information on the effectiveness of an intervention was derived from a review of the scientific literature from 1980 to 2007. (see “Appendix” for a list of effectiveness values and sources of information.) A standardized intervention effectiveness score was estimated for each value of population reduction in risk factor (PRRF) across all 15 factors using the following formula: Effective Score = PRRF/SD (PRRF); where SD (PRRF) is the standard deviation of the population reduction in risk factor ratio.
The cost criterion is the per capita cost of a public health intervention for the duration of the intervention trial. Information on cost of interventions for each risk factor and its sources derived from literature are provided in “Appendix”. For each value of unit cost, a standardized intervention cost score has been estimated across all 15 factors using the following formula: Cost Score = (1/cost)/SD (1/cost); where SD (1/cost) is the standard deviation of inverse of the cost.
Weighting
We assigned weights to criteria as multipliers of criteria scores in the following way: (a) a weight of 2 for the scores of severity and cost of intervention criteria because of their importance to Italy’s public health and highest relative confidence in their validity; (b) a weight of 1 for the scores of magnitude and disparity criteria to indicate average importance for public health and confidence on their validity; (c) a weight of 0.5 for the scores of urgency (i.e., [0.5 × ((1 + Δ)/(SD (1 + Δ))]) and effectiveness criteria to indicate possible bias as measures of tendency and intervention in effect in Italy; (d) and if the urgency score is negative (i.e., Δ is negative and Δ/SD (Δ) and absolute value is greater than 1 in the formula: [(1 + (Δ)/SD (Δ)], or 1/[(1 + (Δ)/SD (Δ)]), then the value is adjusted by convention to a small, fixed, positive number that takes the values of the inverse of the maximum positive value.
Risk factor priority final score
For each risk factor, the individual scores of the criteria severity, urgency, magnitude, disparity, effectiveness, and cost were multiplied to generate the final Risk Factor Priority score formula as follows: [(Severity Score) × (Urgency score × Magnitude Score × Disparity Score × Effectiveness Score × Cost Score)].
Results
Table 1 shows true, unweight and non-standardized indicator values for all six criteria. Table 2 shows indicator values that have been standardized and Table 3 shows indicator values that have been standardized and weighted, thus providing a more accurate view of the relative difference of criteria across risk factors. There were 261,741 deaths attributable to the 15 risk factors, with a significant number of deaths attributed to the top-ranked risk factors: cigarette smoking, ever told had hypertension, physical inactivity, not having blood pressure screening in the past 2-years, alcohol (heavy drinking) and not eating 5 fruits and vegetables a day (Tables 1, 2, 3).
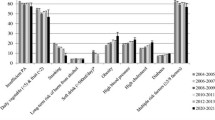
Except for ever told had diabetes with a 5% prevalence, all other 15 risk factors had high prevalence (≥20%), with 73% of the populations estimated to be physically inactive and more than 90% not ever having a rectosigmoidoscopy in prior 5 years, not ever having FOBT in prior 5 years, and not eating 5 fruits and vegetables a day; all top-ranked risk factors for magnitude (Tables 1, 2, 3).
Among top-ranked risk factors for urgency, ever told had diabetes experienced a significant increase in prevalence in 5 years (2%), and the prevalence of not eating 5 fruits and vegetables a day, not having cervical screening in prior 3 years and not having a rectosigmoidoscopy in prior 5 years were flat between 2007 and 2009, while all other risk factors had lower priority with decreased prevalence in this period (Tables 1, 2, 3). There was a marked reduction in the prevalence of alcohol (heavy drinking), cigarette smoking, never having cholesterol screening and ever told had hypertension over the same period.
Diabetes presented the highest disparity score with nearly threefold higher prevalence for persons who had less than a high school education compared to a person with a high school education, followed by ever told had hypertension, not having a mammography in prior 2 years with about 90% higher prevalence rate (Tables 1, 2, 3). Alcohol (heavy drinking), overweight and obesity, ever told had high cholesterol and cigarette smoking all presented disparity but at a lower level.
Most community-based interventions had low (10%) to moderate (50%) effectiveness to reduce risk factor prevalence (Tables 1, 2, 3). The cost of implementing an intervention per person reached varied from a low of $4.31 (US dollar) for promoting physical activity to a high of $550 (US dollar) for mammography programs in the US.
We used natural breaks in the scores for the six criteria and the final Risk Factor Priority score to rank order priorities. Table 4 presents the risk factor priority model final ranking of risk in four ways: (a) model 1 includes the severity criterion score only; (b) model 2, consisting of the product of all six unweight and standardized criteria scores; (c) model 3, consisting of the product of five standardized criteria scores weighted and the rescaled urgency score weighted by constrained maximum values (see “Methods” and Tables 2, 3 footnotes); and (d) model 4, consisting of the product of five standardized criteria scores and the rescaled urgency score, all weighted (see “Methods” and Table 2, 3 footnotes).
Compared to model 1, ranking of the top and bottom priority risk factors in models 2, 3 and 4 was mostly similar. However, significant shifts in ranking were noted after standardization and weighting for overweight and obesity that went from 7th to 9th; not having a FOBT that went from 13th to 8th; and hypercholesterolemia that went from 9th to 5th place.
Discussion
To our knowledge, there were no reported assessments of priorities for public health programs in Italy that used criteria similar to the risk factor priority model. The top six priorities in risk factor reduction for Italy in 2009 on the basis of the severity criterion alone are as follows: cigarette smoking, ever told had hypertension, physical inactivity, not having blood pressure screening, alcohol (heavy drinking), and not eating 5 fruits or vegetables a day. After introduction of the other five priority criteria, hypercholesterolemia and never having had a FOBT join the other six factors among the top eight priorities in the risk factor priority model.
The risk factor priority model modulates the severity criterion (i.e., attributable mortality) by incorporating criteria such as temporal trend of the risk factor, risk factor magnitude, risk factor disparity between groups defined by educational status, level of intervention effectiveness to reduce a risk factor, and the cost of this intervention. In a recent review of priority setting for the health-care field in the developing world (Youngkong et al. 2009), few approaches used quantitative tools or resulted in a rank ordering of interventions as presented in this paper.
Our finding that the top risk factor priorities using this model are mostly influenced by their ranking of the severity criteria should be cautiously interpreted. The severity criterion captures the potential long-term effect of a risk factor on chronic disease, as in the causal relationship between cigarette smoking and lung cancer (i.e., 15–30 years of induction period). Therefore, this measure may over represent the true effect of a risk factor because the factor prevalence and mortality are measured in the present.
The method and data presented in this paper have other limitations. First, the model does not incorporate a political view or the perceptions of stakeholders on priorities as recommended by many (Ryan et al. 2001). Second, our literature review included studies regardless of the time allowed for intervention effect and the appropriateness of the implementation. Third, although estimates of PAFs were calculated within gender or age groups, and utilized RR fully adjusted for confounding, confounding may be still present and cause misestimating (Benichou 2001). Fourth, the urgency criterion is based on only 2 years of prevalence data for all but one risk factor; thus, a true risk factor trend effect on the model is likely unknown. Fifth, because effectiveness and cost estimates used in the model are from U.S. public health programs or studies, they likely misestimate effect and cost of a preventive strategy in Italy. A final limitation is that estimated PAF should be used when the risk factor is causally related to the outcome, and there is consensus that the exposure is amenable to intervention (Rockhill et al. 1998). Though the screening practices used in the risk factor priority model are amenable to public health intervention, their unavailability will not necessarily increase people’s risk of developing or dying of chronic diseases. However, our approach is easy to adapt and apply by local health departments to set priorities for interventions when resources are limited. Indeed, given the uncertainties and the sensitivity of the risk factor priority model to variations within and across criteria, weighting of criteria and sensitivity analysis is recommended. The weighting of criteria scores did not substantially change the top risk factor priorities.
Our finding of the risk factor priorities for chronic disease prevention in Italy has policy implications. In the WHO European region in 2005, 77% of all Disabiliy-Adjusted-Life-Years (DALYs) and 86% of premature deaths are related to non-communicable diseases, of which approximately 73% are caused by cardiovascular disease, cancer, and diabetes (Singh 2008). In addition, rates of death and disability caused by chronic diseases are predicted to continue growing among people in high-income countries (Suhrcke et al. 2007; Mathers and Loncar 2007).
Although tobacco smoking was second priority in the Risk Factor Prioritization model, it is trending down in Italy. In Europe over the past 30 years, the proportion of smokers has dropped to 15%. Conversely, tobacco use is rising in eastern Europe and still remains the leading avoidable cause of death in industrialised nations (Novotny 2008; World Health Organization 2002).
Both hypertension and not having had a blood pressure screening ranked among top priorities in the Risk Factor Prioritization model. It has been reported that men and women in western Europe had the highest systolic blood pressure (SBP) among high-income regions (Danaei et al. 2001). Female SBP decreased in western Europe and Australasia, whereas male SBP fell most in high-income North America, followed by Australasia and western Europe where it decreased by more than 2.0 mm Hg per decade (posterior probabilities >0.98).
Alcohol as measured by heavy drinking causes chronic illnesses, such as alcohol dependence, vascular disease (e.g., hypertension), hepatic cirrhosis, and various cancers and contributes to accidental deaths. The global loss of DALYs attributed to alcohol is 4.7%, whereas the share for eastern Europe is significantly higher at 10.7% (Jamison 2006; Novotny 2008).
Obesity did not rank high in our models. Though almost a third of all people living in Europe are overweight (James et al. 2004; Novotny 2008), a WHO study found that Italy was the only high-income European country in which female BMI decreased from 1980 to 2008, and Italy and Switzerland had one of the smallest increases in male BMI (Finucane et al. 2011).
Hypercholesterolemia ranked 5th among priorities in the adjusted Risk Factor Prioritization models (standardized or weighted). Despite a downward trend of total cholesterol in the high-income regions of Australasia, North America, and western, central, and eastern Europe, serum total cholesterol in 2008 was the highest in the high-income regions of Australasia, North America, and western Europe (Farzadfar et al. 2011).
Despite its low-final ranking in priority, our finding of an upward trend in diabetes in Italy is supported by published reports that suggest that deaths directly attributable to diabetes are predicted to rise approximately 30% in Europe from 2005 to 2030 (World Health Organization 2006).
Our finding of educational disparities in the prevalence of the risk factor is partially supported by other reports. In a study to evaluate inequity in the occurrence of chronic diseases by education status in Europe, researchers identified a higher prevalence of heart disease, stroke, diabetes, some forms of cancer, and hypertension among the lower education group (Dalstra et al. 2005). Another study reported persistent health status disparity by region in Italy (France et al. 2005).
Policy makers can use the risk factor priority model to address different concerns, as exemplified by alcohol in Italy. If the concern is alcohol severity as expressed by attributable mortality, then it ranked moderate-high (i.e., 6th–7th). If there is also interest in the effectiveness and the low cost of public health strategies to reduce alcohol, then it would rank higher as the 4th priority (data not in tables). On the other hand, if only the magnitude of alcohol today (prevalence) and its urgency (i.e., prevalence trend) are a concern then it would rank very low compared to other risk factors. The magnitude and urgency criteria combined provide planners with a look at the future potential of a risk factor severity, thus allowing for addressing it at the present time. A risk factor severity will increase over time if its magnitude and urgency are high, and cost-effective interventions that reduce it are not available or used.
The risk factors priority model is easy to apply since it uses commonly known epidemiologic measures (i.e., prevalence, number of deaths, relative risk, and PAF) and indicators (e.g., prevalence trend). It is also flexible to include other criteria (e.g., DALYs) and risk/preventive factors (e.g., social determinants of health); as well as to focus on a sub-population (e.g., ranking of NTD risk factor in a minority population). Moreover, the use of multiple priority criteria will increase its acceptability. Previous studies on prioritization showed that stakeholders appreciated the flexibility of choosing critical indicators (Baltussen et al. 2006; Phillips et al. 2010). Our methodology will allow cross country comparison based on readily available risk factors surveillance (Coffield et al. 2001).
Public health professionals in Italy could use our model in order to set better priorities or review as to how their activities compared with our findings. Moreover, they could improve the prioritization by collecting and using better data for risk factors and relative risk, as well as applying other methods for estimation of the severity criterion (Bruzzi et al. 1985; Rückinger et al. 2009). Indeed our study should be used to guide health intervention and gather support for action. Finally, the risk factor priority model is a planning tool that should be used together with other approaches in a participatory process of planning (Simoes et al. 2006).
References
Abramson JH, Gofin R, Hopp C, Gofin J, Donchin M, Habib J (1981) Evaluation of a community program for the control of cardiovascular risk factors: the CHAD program in Jerusalem. Isr J Med Sci 17(2–3):201–212
Atri J, Falshaw M, Gregg R, Robson J, Omar RZ, Dixon S (1997) Improving uptake of breast screening in multiethnic populations: a randomized controlled trial using practice reception staff to contact non-attenders. BMJ 315:1356–1359
Aubin M, Vezina L, Fortin JP, Bernard PM (1994) Effectiveness of a program to improve hypertension screening in primary care. Can Med Assoc J 150(4):509–515
Baldissera S, Campostrini S, Binkin N, Minardi V, Minelli G, Ferrante G et al (2011) Features and initial assessment of the Italian Behavioral Risk Factor Surveillance System (PASSI), 2007–2008. Prev Chronic Dis 8:A24. Available from: http://www.cdc.gov/pcd/issues/2011/jan/10_0030.htm. Accessed on 10 Feb 2011
Baltussen R, Niessen L (2006) Priority setting of health interventions: the need for multi-criteria decision analysis. Cost Eff Resour Alloc 4:14
Baltussen R, Stolk E, Chisholm D, Aikins M (2006) Towards a multi-criteria approach for priority setting: an application to Ghana. Health Econ 15:689–696
Baron RC, Rimer BK, Breslow RA, Coates RJ, Kerner J, Melillo S, Habarta N, Kalra GP, Chattopadhyay S, Wilson KM, Lee NC, Mullen PD, Coughlin SS, Briss PA, Task Force on Community Preventive Services (2008) Client-directed interventions to increase community demand for breast, cervical, and colorectal cancer screening a systematic review. Am J Prev Med 35(1S):34–55
Benichou J (2001) A review of adjusted estimators of attributable risk. Stat Methods Med Res 10:195–216
Brownson RC, Smith CA, Pratt M, Mack NE, Jackson-Thompson J, Dean CG, Dabney S, Wilkerson JC (1996) Preventing cardiovascular disease through community-based risk reduction: the Bootheel Heart Health Project. Am J Public Health 86(2):206–213
Bruzzi P, Green SB, Byar DP, Brinton LA, Schairer C (1985) Estimating the population attributable risk for multiple risk factors using case–control data. Am J Epidemiol 122:904–914
Centers for Disease Control and Prevention (2006) Improvement in lipid and glycated hemoglobin control among black adults with diabetes—Raleigh and Greensboro, North Carolina, 1997–2004. MMWR 55(46):1248–1251
Centers for Disease Control and Prevention (2007) Best Practices for Comprehensive Tobacco Control Programs—2007. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health
Centers for Disease Control and Prevention (2010) Smoking-attributable mortality, morbidity, and economic costs (SAMMEC): adult SAMMEC and maternal and child health (MCH) SAMMEC software, 2002. Available at http://www.cdc.gov/tobacco/sammec. Accessed March 20
Chisholm D, Rehm J, van Ommeren M, Monteiro M (2004) Reducing the global burden of hazardous alcohol use: a comparative cost-effectiveness analysis. J Stud Alcohol 65:782–793
Coffield AB, Maciosek MV, McGinnis JM et al (2001) Priorities among recommended clinical preventive services. Am J Prev Med 21:1–9
Dalstra JAA, Kunst AE, Borrell C, Breeze E, Cambois E, Costa G, Geurts JJM, Lahelma E, Van Oyen H, Rasmussen NK, Regidor E, Spadea T, Mackenbach JP (2005) Socioeconomic differences in the prevalence of common chronic diseases: an overview of eight European countries. Int J Epidemiol 34:316–326
Danaei G, Finucane MM, Lin JK, Singh GM, Paciorek CJ, Cowan MJ, Farzadfar F, Stevens GA, Lim SS, Riley LM, Ezzati M (2001) National, regional, and global trends in systolic blood pressure since 1980: systematic analysis of health examination surveys and epidemiological studies with 786 country-years and 5.4 million participants. Lancet 377:568–577
Danaei G, Ding EL, Mozaffarian D, Taylor B, Rehm J et al (2009) The preventable causes of death in the United States: comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med 6(4):e1000058. doi:10.1371/journal.pmed.1000058
Denberg TD, Coombes JM, Byers TE, Marcus AC, Feinberg LE, Steiner JF, Ahnen DJ (2006) Effect of a mailed brochure on appointment-keeping for screening colonoscopy: a randomized trial. Ann Intern Med 145(12):895–900
Dietrich AJ, Tobin JN, Cassells A, Robinson CM, Greene MA, Sox CH, Beach ML, DuHamel KN, Younge RG (2006) Telephone care management to improve cancer screening among low-income women: a randomized, controlled trial. Ann Intern Med 144(8):563–571
Dinh-Zarr TB, Sleet DA, Shults RA, Zaza S, Elder RW, Nichols JL, Thompson RS, Sosin DM, The Task Force on Community Preventive Services (2001) Reviews of evidence regarding interventions to increase the use of safety belts. Am J Prev Med 21(4):48–65
Ekwueme DU, Gardner JG, Subramanian S, Tangka FK, Bapat B, Richardson LC (2008) Cost analysis of the National Breast and Cervical Cancer Early Detection Program: selected states, 2003 to 2004. Cancer 112(3):626–635
Emmelin M, Weinehall L, Stenlund H, Wall S, Dahlgren L (2007) To be seen, confirmed, and involved—a ten year follow-up of perceived health and cardiovascular risk factors in a Swedish community intervention programme. BMC Public Health 7:190–202
Escobedo LG, Chorba TL, Remington PL, Anda RF, Sanderson L, Zaidi AA (1992) The influence of safety belt laws on self-reported safety belt use in the United States. Accid Anal Prev 24:643–653
Farzadfar F, Finucane MM, Danaei G, Pelizzari PM, Cowan MJ, Paciorek CJ, Singh GM, Lin JK, Stevens GA, Riley LM, Ezzati M, On behalf of the Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (2011) National, regional, and global trends in serum total cholesterol since 1980: systematic analysis of health examination surveys and epidemiological studies with 321 country-years and 3·0 million participants. Lancet 377:578–586
Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, Singh GM, Gutierrez HR, Lu Y, Bahalim AN, Farzadfar F, Riley LM, Ezzati M, On behalf of the Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (2011) National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 377:557–567
France G, Taroni F, Donatini A (2005) The Italian health-care system. Health Econ 14:S187–S202
Geodemo Istat.it (2009) Le Tavole di mortalità: http://www.demo.istat.it/unitav/index.html?lingua=ita. Accessed on July 20
Gofin J, Gofin R, Abramson JK, Ban R (1986) Ten-year evaluation of hypertension, overweight, cholesterol, and smoking control: the CHAD program in Jerusalem. Prev Med 15(3):304–312
Hanlon JJ, Pickett G (1979) Public health administration and practice. C.V. Mosby, St. Louis, MO
Healthy People 2010 toolkit: setting health priorities and establishing objectives. Available at: http://www.health.gov/healthypeople/state/toolkit/priorities.htm. Accessed 20 July 2010
Hopkins DP, Husten CG, Fielding JE, Rosenquist JN, Westphal LL (2001) Evidence reviews and recommendations on interventions to reduce tobacco use and exposure to environmental tobacco smoke a summary of selected guidelines. Am J Prev Med 20(2): 67–87
ISTAT (2003) Unit Struttura e dinamica sociale: Health interview survey: Health status and use of health services—Years 1999–2000. ISTAT, Roma
ISTAT Unit Struttura e dinamica sociale (2006) Health interview survey: health status and use of health services—years 2004–2005. Roma
James WPT, Jackson-Leach R, Ni Mhurchu C, Kalamara E, Shayeghi M, Rigby NJ, Nishida C, Rodgers A 2004 Overweight and obesity (high body mass index). In: Ezzati M, Lopez A, Rodgers A, Murray CJL (eds) Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. World Health Organization, Geneva. Available from http://www.who.int/publications/cra. Accessed 10 Dec 2009
Jamison D (2006) Investing in health. In: Jamison D (ed) Disease control priorities in developing countries, 2nd edn. Oxford University Press, New York
Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, Stone EJ, Rajab MW, Corso P (2002) The effectiveness of interventions to increase physical activity a systematic review. Am J Prev Med 22(4S):73–106
King ES, Rimer BK, Seay J, Balshem A, Engstrom PF (1994) Promoting mammography use through progressive interventions: is it effective? Am J Public Health 84:104–106
Koffman DM, Bazzarre T, Mosca L, Redberg R, Schmid T, Wattigney WA (2001) An evaluation of Choose to Move 1999: an American Heart Association physical activity program for women. Arch Intern Med 161(18):2193–2199
Lantz PM, Stencil D, Lippert MT, Jaros L, Eaker ED (1996) J Public Health Manag Pract. Summer 2(3):54–59
Larimer ME, Lee CM, Kilmer JR, Fabiano PM, Stark CB, Geisner IM, Mallett KA, Lostutter TW, Cronce JM, Feeney M, Neighbors C (2007) Personalized mailed feedback for college drinking prevention: a randomized clinical trial. J Consult Clin Psychol 75(2):285–293
Levin ML (1953) The occurrence of lung cancer in man. Acta Unio Int Contra Cancrum 9:531–541
Mandelblatt JS, Schechter CB, Yabroff KB, Lawrence W, Dignam J, Muennig P, Chavez Y, Cullen J, Fahs M (2004) Benefits and costs of interventions to improve breast cancer outcomes in African American women. J Clin Oncol 22:2554–2566
Mathers CD, Loncar D (2007) Updated projections of global mortality and burden of disease, 2002–2030: data sources, methods and results. World Health Organization, Geneva. Available from http://www.who.int/healthinfo/statistics/bodprojections2030/en/index.html. Accessed on 20 July 2010
Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, Marks JS (2003) Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 289:76–79
Moura EC, de Morais Neto OL, Malta DC, de Moura L, da SilvaI NN, BernaI R, Claro RM, Monteiro CA 2008 Vigilância de Fatores de Risco para Doenças Crônicas por Inquérito Telefônico nas capitais dos 26 estados brasileiros e no Distrito Federal (2006). [Surveillance of risk-factors for chronic diseases through telephone interviews in 27 Brazilian cities (2006)]. Rev bras epidemiol [serial online] 11 (Suppl 1):20–37 Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-790X2008000500003&lng=en&nrm=iso. Accessed on January 17, 2011
Muennig P, Fiscella K, Tancredi D, Franks P (2010) The relative health burden of selected social and behavioral risk factors in the United States: implications for policy. Am J Public Health 100:1758–1764
Murray CJ, Lopez AD (1997) Global mortality, disability and the contribution of risk factors. Lancet 349:1436–1442
Myers RE, Turner B, Weinberg D, Hyslop T, Hauck WW, Brigham T, Rothermel T, Grana J, Schlackman N (2004) Impact of a physician-oriented intervention on follow-up in colorectal cancer screening. Prev Med 38(4):375–381
Novotny TE (2008) Preventing chronic disease: everybody’s business. In: Nolte E, Mckee M (eds) Caring for people with chronic conditions: a health system perspective. Open University Press, Maidenhead
Phillips CJ, Fordham R, Marsh K et al (2010) Exploring the role of economics in prioritization in public health: what do stakeholders think? Eur J Public Health 21(5):578–584
Potter JD, Finnegan JR, Guinard J-X, Huerta EE, Kelder SH, Kristal AR, Kumanyika S, Lin R, Motsinger BM, Prendergast FG, Sorensen G, Callahan KM (2000) 5 A Day for Better Health Program Evaluation Report. National Institutes of Health, National Cancer Institute, Bethesda. NIH Publication No. 01-4904. [Feb 10, 2009] Available from: http://dccps.nci.nih.gov/5ad_6_eval.html
REACH (2008) U.S. At-A-Glance, 2008. http://www.cdc.gov/NCCdphp/publications/AAG/pdf/reach.pdf. Accessed on 2 Dec 2009
REACH (2010) At-A-Glance, 2006. http://www.reachforwellnessatlanta.com/Documents/PDF%20of%20CDCs%20REACH2010.pdf. Accessed 2 Dec 2009
Reger-Nash B, Fell P, Spicer D, Fisher BD, Cooper L, Chey T et al (2006) BC walks: replication of a communitywide physical activity campaign. Prev Chronic Dis [serial online] Jul [Dec 15, 2008]. Available from: http://www.cdc.gov/pcd/issues/2006/jul/05_0138.htm
Rockhill B, Newman B, Weinberg C (1998) Use and misuse of population attributable fractions. Am J Public Health 88:15–19
Rooney BL, Thompson JE (2009) The value of a web-based interactive regional health scorecard in setting public health priorities. WMJ 108:403–406
Rückinger S, von Kries R, Toschke AM (2009) An illustration of and programs estimating attributable fractions in large scale surveys considering multiple risk factors. BMC Med Res Methodol 9:7
Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, Napper M, Robb CM (2001) Eliciting public preferences for healthcare: a systematic review of techniques. Health Technol Assess 5:1–186
Sequist TD, Zaslavsky AM, Marshall R, Fletcher RH, Ayanian JZ (2009) Patient and physician reminders to promote colorectal cancer screening: a randomized controlled trial. Arch Intern Med 169(4):364–371
Shults RA, Elder RW, Sleet DA, Nichols JL, Alao MO, Carande-Kulis VG, Zaza S, Sosin DM, Thompson RS, The Task Force on Community Preventive Services (2001) Reviews of evidence regarding interventions to reduce alcohol-impaired driving. Am J Prev Med 21(4S):66–88
Simoes EJ, Land GZ, Metzger R, Mokdad A (2006) Prioritization MICA: a Web-based application to prioritize public health resources. J Public Health Manag Pract 12(2):161–169
Sin JP, St Leger AS (1999) Interventions to increase breast screening uptake: do they make any difference? J Med Screen 6(4):170–181
Singh D (2008) How can chronic disease management programmes operates across care settings and providers? World Health Organization 2008 and World Health Organization, on behalf of the European Observatory on Health Systems and Policies 2008
Stead MJ, Wallis GW, Wheaton ME (1998) Improving uptake in non-attenders of breast screening: selective use of second appointment. J Med Screen 5:69–72
Suhrcke M, Rocco L, McKee M (2007) Health: a vital investment for economic development in eastern Europe and central Asia. WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies, Copenhagen
Trust for America’s Health (2008) Prevention for a healthier America. Trust for America’s Health, Washington (DC). Available from: http://healthyamericans.org/reports/prevention08
Turner KM, Wilson BJ, Gilbert FJ (1994) Improving breast screening uptake: persuading initial non-attenders to attend. J Med Screen 1:199–202
Veerman JL, Barendregt JJ, Mackenbach JP, Brug J (2006) Using epidemiological models to estimate the health effects of diet behaviour change: the example of tailored fruit and vegetable promotion. Public Health Nutr 9(4):415–420
Vilnius D, Dandoy S (1990) A priority rating system for public health programs. Public Health Rep 105:463–470
Vinker S, Nakar S, Rosenberg E, Kitai E (2002) The role of family physicians in increasing annual fecal occult blood test screening coverage: a prospective intervention study. Isr Med Assoc J 4:424–425
Weinstein MC, Stason WB (1977) Foundations of cost-effectiveness analysis for health and medical practices. N Engl J Med 296:716–721
Whitlock EP, Green CA, Polen MR (2004) Behavioral counseling interventions in primary care to reduce risky/harmful alcohol use. Systematic Evidence Review. No. 30. (Prepared by the Oregon Evidence-based Practice Center under Contract No. 290-97-0018). Agency for Healthcare Research and Quality. April 2004, Rockville. Available at: www.ahrq/gov/clinic/serfiles.htm
Williams EMI, Vessey MP (1989) Randomised trial of two strategies offering women mobile screening for breast cancer. BMJ 299:158–159
World Health Organization (2002) The world health report 2002: reducing risks, promoting healthy life. World Health Organization, Geneva
World Health Organization (2006) Health statistics and health information systems: projections of mortality and burden of disease to 2030. World Health Organization, Geneva. Available from: http://www.int/healthinfo/statistics/bodprojections2030/en/index.html. Accessed 20 July 2010
Yabroff KR, O’Malley A, Mangan P, Mandelblatt J (2001) J Am Med Women Assoc. Fall 56(4):166–173
Yabroff KR, Mangan P, Mandelblatt J (2003 ) J Am Board Fam Pract 16(3):188–203
Youngkong S, Kapiriri L, Baltussen R (2009) Setting priorities for health interventions in developing countries: a review of empirical studies. Trop Med Int Health 14:930–939
Zaza S, Briss PA, Harris KW (eds) (2005) The Guide to Community Preventive Services: What Works to Promote Health?. Oxford University Press, NY
Acknowledgments
This study was funded through the Framework Programme SiVeAS (FP 2008-2010) of the National Italian Ministry of Health (Ministero della Salute), under the grant agreement n Reg. n. 5 -Fgl. N. 36 Court of Auditors (Corte dei Conti)—SiVeAS 8M41B and SiVeAS8M41C. The authors are grateful for the valuable input of Kurt Greenlund and David Williamson, and for the administrative support of Sonia Martire.
Conflict of interest
All co-authors have no conflict of interest associated with any part of the study.
Ethical standard
This study complies with the current laws of the country in which it was performed.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
See Table 5.
Rights and permissions
About this article
Cite this article
Simoes, E.J., Mariotti, S., Rossi, A. et al. The Italian health surveillance (SiVeAS) prioritization approach to reduce chronic disease risk factors. Int J Public Health 57, 719–733 (2012). https://doi.org/10.1007/s00038-012-0341-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-012-0341-5