
Abstract
Objectives
We investigated inequalities in self-rated health between immigrants, their descendants, and ethnic Danes and explored mediation by socioeconomic position and interactions between country of origin and socioeconomic position.
Methods
Cross-sectional survey data on self-rated health from 4,985 individuals aged 18–66 years including immigrants from seven non-Western countries, their descendants, and ethnic Danes was linked to registry-based data on education, employment status, and income as indicators of socioeconomic position. Using multiple logistic regression analysis, we estimated the association between country of origin and self-rated health.
Results
Immigrants reported poorer health compared with ethnic Danes [age-adjusted odds ratio (OR) = 2.0–7.3 for men; 2.1–10.5 for women, dependent on country of origin] as well as their descendants (OR = 1.6–3.8 for men; 1.5–2.0 for women). Adjustment for socioeconomic position attenuated this association. Stratified analysis indicated that the effect of socioeconomic position on self-rated health varied across the groups.
Conclusion
Policies addressing inequalities in health between immigrants, their descendants, and ethnic Danes should target underlying socioeconomic inequalities. Further research of the effects of socioeconomic position on health among immigrants and descendants is needed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Inequalities in health among migrants and ethnic minorities pose significant challenges to public health practitioners and policy makers across Europe. Differences in self-rated health between migrants/ethnic minorities and the majority populations have been documented in several European countries (Cooper 2002; Iglesias et al. 2003; Lindstrom et al. 2001; Lorant et al. 2008; Reijneveld 1998; Wiking et al. 2004), but no scientific studies exist on self-rated health of adult immigrants or descendants in Denmark (Nielsen and Krasnik 2010). Self-rated health is a subjective measure of a person’s perceived general health and has proven to be a strong and independent predictor of morbidity and mortality (Idler and Benyamini 1997) and is therefore a widely used measure of overall health status.
Migration to Denmark accelerated in the 1960s when young men from Turkey, Pakistan and the former Yugoslavia immigrated as a response to the need of unskilled labor in Denmark. Throughout the 1980s and 1990s, a substantial number of family reunifications took place parallel to an influx of refugees from the Balkans, Somalia and the Middle East (Østergaard 2007). Today, non-Western immigrants and their descendants constitute 6.6% of the population (Statistics Denmark 2010a). Non-western immigrants are more likely to be unemployed, to earn a low income and to have a lower educational level that ethnic Danes. Descendants compare well to immigrants in this regard but remain disadvantaged compared to ethnic Danes (Statistics Denmark 2009). Evidence on socioeconomic inequalities in health is well-established (Borg and Kristensen 2000; Marmot et al. 1984, 1991) and thus, the effects of immigrant/ethnic minority status and poor socioeconomic conditions constitutes a double burden on health (Lindstrom et al. 2001; Williams et al. 2010). Thus, migrant/ethnic inequalities in health cannot be understood fully without taking socioeconomic disadvantages into consideration (Kawachi et al. 2005).
Socioeconomic position is a multidimensional concept. One of the challenges in relation to migrants/ethnic minorities is how to interpret the complex relationship between immigrant/ethnic minority status and socioeconomic position (Krieger et al. 1997; Stronks and Kunst 2009; Williams et al. 2010). One approach is to conceptualize socioeconomic position as a mediator between country of origin and health. However, many studies treat socioeconomic position as a confounder in a multivariate model. One problem with this approach is that often, only adjusted results are shown. The consequence is that the explanatory role of socioeconomic position is lost and only the adjusted results, “cleaned” for socioeconomic effects, are interpreted (Nazroo 2003). Moreover, socioeconomic position might have different health consequences within different ethnic groups (Stronks and Kunst 2009). Although the importance of testing for statistical interactions has been emphasized elsewhere (Braveman et al. 2005), only few studies do so. There is no consensus on how immigrant/ethnic minority status and socioeconomic position contribute in shaping inequality in health, and in particular on how the two concepts might interact.
This study aims at bridging the gap in the literature by studying the self-rated health of immigrants and descendants in Denmark and by giving explicit attention to the explanatory role of socioeconomic position. We included three indicators of socioeconomic position: family income, education and employment status. These indicators represent different pathways through which socioeconomic position can affect health such as access to material resources, status, prestige and knowledge (Galobardes et al. 2006a). The study’s objectives were to (1) investigate whether inequalities in self-rated health related to immigrant status existed in Denmark; (2) determine the level of mediation by three indicators of socio-economic position; and (3) explore possible interactions between country of origin and socioeconomic position.
Methods
Study design and study population
Data from a cross-sectional national survey in Denmark from 2007 was used. Ethnic Danes, the seven largest non-Western immigrant groups from the former Yugoslavia, Iraq, Iran, Lebanon, Turkey, Pakistan and Somalia were included in the study as well as descendants of first generation with Turkish and Pakistani origins. This definition was taken from Statistics Denmark: ethnic Danes have at least one parent who is born in Denmark and has Danish citizenship, immigrants are born outside Denmark to parents who are both foreign citizens or born in a foreign country and descendants are born in Denmark to parents of whom none is a Danish citizen born in Denmark (Statistics Denmark 2009). Eligible participants were between 18 and 66 years and only immigrants who had resided in Denmark more than 3 years were included in the study. A random sample of 11,450 persons was drawn from the Danish Civil Registration System, which contains a unique record of all Danish residents. Immigrant and descendant groups were over-sampled to ensure a sufficient sample size of each group. The eligible sample after dropout due to death, emigration or research protection consisted of 9,515 individuals. Subsequent dropout was due to the lack of available telephone numbers (N = 2,676), lack of telephone contact (N = 1,317) and refusal of participation after contact was established (N = 569). For this study, the inclusion criteria were a valid response on the question on self-rated health and valid registry-based data on all three indicators of socioeconomic position. A total of 4,985 persons were included, resulting in a response rate of 52.4% of the eligible sample. The response rate was lower among immigrants (32–56%) and descendants (46–55%) than the group of ethnic Danes (73%).
Data collection
The questionnaire was developed through consultations with citizens from the included immigrant groups to ensure cultural and lingual acceptability. The questionnaire was translated into six languages using back-translation. Interviews were conducted by telephone (N = 4,239) or self-administered via the internet (N = 714) in June–August 2007. Survey data were linked to socioeconomic registry data on all survey respondents through the Civil Registration System. Information on employment was retrieved from the IDA database, information on income was obtained from the Danish Tax and Customs Administration (SKAT) and information on education was available from the Population Education Registry (BU) from Statistics Denmark. All registry data stemmed from 2005. Under Danish law, questionnaire surveys, interview studies and registry research require permission from the Danish Data Protection Agency. This permission was obtained.
Variables
Self-rated health was measured by asking: “In general, would you say your health is?” Responses were ‘excellent’, ‘very good’, ‘good’, ‘fair’ or ‘poor’ The variable was dichotomized grouping ‘excellent’, ‘very good’, and ‘good’ as good and ‘fair’ and ‘poor’ as poor. The main independent variable was registry-based country of origin. Age was grouped into four groups: 18–29, 30–39, 40–49 and 50–66 years.
All measures on socioeconomic position were registry-based: Educational level was based on the highest attained level of education. Information on the education of immigrants was obtained from a questionnaire sent annually to all immigrants aged 16–59 who came to Denmark after the age of 15 and who are not enrolled in or have completed an education in Denmark. Statistics Denmark classifies immigrants’ education. These data are subject to some uncertainty as well as missing information (Statistics Denmark 2009). We used the UNESCO International Standard Classification of Education (UNESCO 1997) to categorize educational level into primary (1–9 years), secondary (10–12 years) and tertiary (>13 years) education. We included “unknown” as a separate category in all regression analyses due to a high number of immigrants whose education is unknown. Employment status was grouped into three categories defined by Statistics Denmark: employed, unemployed, and outside the workforce. The employed group comprises employees and self-employed. Unemployment is classified as full unemployment in week 48. The category of people outside the workforce comprises people who are permanently or temporarily withdrawn from the workforce: e.g. pensioners, students and individuals on social welfare payments. Family income was recorded as gross annual family income in 2005 and was categorized into quartiles based on the income distribution of the eligible sample of the study population (N = 9,515).
Statistical analysis
Data were analyzed separately for men and women using multiple logistic regressions to examine the association of country of origin and self-rated health while adjusting for age. Socioeconomic indicators were included stepwise. We tested five different models: (I) crude; (II) age-adjusted; (III) age and education adjusted; (IV) age and employment status adjusted; and (V) age and income adjusted separately for men (a) and women (b). The ethnic Danes constituted the reference group for both sexes. Since it is a priori plausible that the effect on self-rated health of education, employment status, and income may depend on country of origin, all models were tested for interaction between country of origin and socioeconomic indicators. Significant interactions were analyzed further by investigating country of origin stratified for socioeconomic position and socioeconomic position stratified for country of origin (model VI and VII). SPSS 16.0 for Windows was used for the analyses.
Results
Study population
Immigrants and particularly descendants were younger than ethnic Danes, and immigrants had a lower educational level compared to the group of ethnic Danes (Table 1). A higher proportion of all immigrant groups, especially women, were unemployed and outside the workforce compared to the group of ethnic Danes. All immigrant groups were overrepresented in the lowest income quartile. Non-respondents had significantly lower educational level, employment rate and family income than respondents (data not shown).
Self-rated health
Most immigrant groups reported poorer health than ethnic Danes, more markedly for women than men. Descendants reported better health than the ethnic Danes (Table 1). All immigrant groups had an increased chance of reporting poor self-rated health in the crude model and this increased after adjusting for age (Table 2). This was most evident for men from the former Yugoslavia [age-adjusted odds ratio (OR) = 4.8, 95% CI = 3.2–7.4], Iraq (OR = 7.3, 95% CI = 4.9–10.8) and Lebanon (OR = 5.3, 95% CI = 3.5–8.0) and women from the same countries as well as Turkey (OR = 5.4, 95% CI = 3.5–8.1) and Pakistan (OR = 6.2, 95% CI = 4.2–9.2). Turkish descendants had increased chance of reporting poor health after adjusting for age: men (OR = 3.8, 95% CI = 2.1–6.9) and women (OR = 2.0, 95% CI = 1.0–3.8). Descendants of Pakistani origin of both sexes did not differ significantly from ethnic Danes after adjusting for age.
Socioeconomic position as a mediating factor
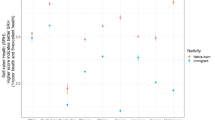
Inclusion of the three indicators of socioeconomic position one-by-one attenuated the association between country of birth and poor self-rated health (Table 2). The greatest effect on the estimates was observed for the groups highlighted above: income-adjusted odds ratios for men from the former Yugoslavia (OR = 3.9, 95% CI = 2.5–5.9), Iraq (OR = 4.5, 95% CI = 3.0–6.9) and Lebanon (OR = 3.3, 95% CI = 2.1–5.1) and women from the former Yugoslavia (OR = 5.2, 95% CI = 3.4–7.9), Iraq (OR = 7.1, 95% CI = 4.6–10.9) and Lebanon (OR = 4.7, 95% CI = 3.0–7.6), Turkey (OR = 4.2, 95% CI = 2.7–6.5) and Pakistan (OR = 4.7, 95% CI = 3.1–7.2). After adjustment for education, employment status, or income, Somalis of both sexes and female descendants of Turkish origin no longer differed significantly from ethnic Danes. However, the elevated risk of poor self-rated health for male descendants of Turkish origin remained after adjusting for employment status (OR = 2.7, 95% CI = 1.5–4.9) and income (OR = 2.8, 95% CI = 1.6–5.1). Figure 1 illustrates the age- and socioeconomic-adjusted estimates for the models without significant interactions from Table 2. Generally, the estimates adjusted for socioeconomic position were similar when comparing the different indicators for each immigrant and descendant group.

Adjusted odds ratios for self-rated health by country of origin for men and women. Denmark (2011): inequality in self-rated health among immigrants, their descendants, and ethnic Danes: examining the role of socioeconomic position
Statistically significant interactions were found between country of origin and education for men and employment status for women. Accordingly, the main effect of country of origin cannot be interpreted directly and is therefore not shown in Table 2, but must be stratified for socioeconomic position. The stratified estimates are shown in Table 3 and Fig. 2. Immigrant men with 10–12 years of education had an increased risk of reporting poor health, particularly men from the former Yugoslavia (OR = 10.0, 95% CI = 5.3–18.9), Iraq (OR = 11.1, 95% CI = 5.7–21.8) and Lebanon (OR = 7.6, 95% CI = 3.7–15.4) compared to ethnic Danish men with 10–12 years of education (model VIa, Table 3; Fig. 2). A similar tendency was seen among men with >13 years of education, but the estimates were lower than among men with 10–12 years of education. Model VIb shows an educational gradient within each immigrant group, but the gradients are similar or smaller in most immigrant groups than among ethnic Danes. However, these were only statistically significant in very few cases. Regarding employment status for women, most immigrant groups had an increased risk of reporting poor self-rated health in all three employment groups (model VIIa, Table 3; Fig. 2), yet, Somalis and descendants with origin from Turkey and Pakistan had none or low increased chance of reporting poor self-rated health. Descendants of Turkish and Pakistani origin showed little or no gradient between the different employment groups (Model VIIb). On the contrary, immigrants from Iraq, Iran, Turkey, Pakistan, Lebanon and Somalia presented differences, which constitute a gradient across employment groups.

Adjusted odds ratios for self-rated health for men by country of origin stratified by education level and for women by country of origin stratified by employment status. Denmark (2011): inequality in self-rated health among immigrants, their descendants, and ethnic Danes: examining the role of socioeconomic position
Discussion
We found considerable inequalities in self-rated health in Denmark after adjusting for age for all immigrant and descendant groups, with the only exception of descendants from Pakistan. Immigrant women in particular reported poor health compared to ethnic Danish women. The risk of poor self-rated health differed: immigrants of both sexes from the former Yugoslavia, Iraq and Lebanon and women from Turkey and Pakistan were most at risk. Socioeconomic position mediated the association between ethnic group and self-rated health. However, large inequalities remained after adjusting for socioeconomic position for most groups except for Somalis and Pakistani descendants of both sexes and female descendants of Turkish origin. Moreover, interactions indicated that the effect of socioeconomic position varied across immigrant and descendant group. A gradient was found in self-rated health within all immigrant groups which was greater for men in the two highest educational strata than in the lowest; and a consistent gradient in self-rated health between the different immigrant and descendant groups among employed women, unemployed as well as women outside the workforce.
The findings of inequalities in self-rated health among immigrants and descendants in Denmark is consistent with other studies from Sweden (Iglesias et al. 2003; Lindstrom et al. 2001; Wiking et al. 2004), Belgium (Lorant et al. 2008), the Netherlands (Reijneveld 1998) and the UK (Cooper 2002). The highest risk was observed among immigrants of both sexes from Iraq, the former Yugoslavia and Lebanon. The women from these groups tended to report poorer health compared to ethnic Danish women than was the case for men. Many refugees from these countries have fled to Denmark, and pre-migration exposures to war and persecution might be possible explanations for the poor health among these groups as well as their poor socioeconomic position. Information on migration status was not available; thus, we were not able to distinguish between refugees, labor migrants or family reunified immigrants. The pattern of self-rated health among descendants of Turkish and Pakistani origin was similar to that of ethnic Danes after adjustment for age and socioeconomic position. This finding is similar to a Swedish study, which found that second generation labor immigrants and refugees did not show increased odds for poor self-rated health compared to the Swedish reference group (Leao et al. 2009). Our finding that immigrant women had higher risk of poor self-rated health than their male counterparts was not seen among descendants. On the contrary, male descendants of Turkish origin stand out in this study as having a high risk of poor self-rated health. Their adverse health might be explained by experienced institutional or interpersonal discrimination (Braveman et al. 2005); or poor ‘acculturation’, which explained part of the association between ethnicity and self-rated health in studies from Sweden. Acculturation was measured as knowledge of Swedish language and experienced discrimination (Wiking et al. 2004) or time in host country and age at migration (Leao et al. 2009). Another key finding was interactions between socioeconomic position and country of origin, which implies that socioeconomic position has different health impacts in different immigrant groups (Stronks and Kunst 2009). Different types of socioeconomic position may be relevant to migrants compared with the majority population (Braveman et al. 2001), and there is a lack of clarity about how socioeconomic position should be measured in migrants (Stronks and Kunst 2009). There was a health gradient for women in all employment groups, which might potentially reflect that employment-related hazards on health are not uniformly distributed amongst the different immigrant and descendant groups compared to ethnic Danes. One possible interpretation of the gradient between immigrant men at different educational levels is that it might not be possible for immigrants to utilize their education in Denmark. This finding favors the Diminishing Returns hypothesis applied in a US-based study, according to which returns on health in terms of income or status from increasing levels of socioeconomic position is lower for minorities than for the majority population and thus, that the health gap between the groups are larger at higher levels of socioeconomic position (Farmer and Ferraro 2005). We did not find a dosis–response relationship between educational level and health gradient across immigrant groups and thus, this hypothesis cannot unambiguously explain this.
Our findings demonstrate that socioeconomic position is an important contributor to inequalities in self-rated health among immigrants and descendants in Denmark. However, inequalities persisted for most groups after adjusting for socioeconomic position, which is supported by existing evidence (Cooper 2002; Lindstrom et al. 2001). Three possible lines of arguments can explain this: First, the conceptualization and measurement of socioeconomic position does not take into account the full complexity of the concept (Krieger et al. 1997). The socioeconomic indicators used in this study contain rough and heterogeneous categories: registration of immigrants’ education obtained outside Denmark is defective; employment status is measured only at one point in time; and the family income variable is not adjusted for family size. This might have underestimated the results as immigrants generally have larger families than ethnic Danes (Statistics Denmark 2009). This might have resulted in residual confounding, and the persistent inequalities might reflect unmeasured aspects of socioeconomic position (Braveman et al. 2005). An alternative approach is to adopt a life course perspective on socioeconomic differentials in health (Galobardes et al. 2006b). This could also further our understanding of the different experiences of migration and ethnic minority status between immigrants and their descendants (Nazroo 2003). Furthermore, it can be argued that conceptualizing socioeconomic position at the individual level does not take adverse effects of living in socially and economically deprived neighborhoods into account (Krieger et al. 1997; Lorant et al. 2008). Poor contextual factors together with poor socioeconomic factors and ethnic minority status might pose a triple burden on the health of immigrants and descendants (Nielsen and Krasnik 2010). The second line of arguments is that migrant and ethnic minority related inequalities in health cannot be reduced to socioeconomic differences (Nazroo 2003; Stronks and Kunst 2009) but must be explained through alternative pathways. Discrimination, institutional as well as interpersonal has been proposed another plausible pathway (Karlsen and Nazroo 2002). The method of adjustment represents the third line of arguments. Braveman et al. (2005) claim that different indicators of socioeconomic position measure different aspects of the concept. Particularly income and education are likely to interact and they should thus be included in the same multivariate model. The three indicators used in this study explained a similar part of the association between country of birth and self-rated health within each group. However, it is possible that the indicators mediated different parts of the socioeconomic pathway and that adjusting for all three and their mutual interactions in the same model would lead us to different conclusions. Moreover, the finding of interactions reveals a complex pattern. Potentially, further interactions might have been found if more accurate and comprehensive measures of socioeconomic position had been applied. This questions the feasibility of adjustment for socioeconomic position and implies that our results must be interpreted with some caution.
The strengths of this study include a large sample size, which allows for comparison of different ethnic groups rather than treating all non-Western minorities as one category. The questionnaire was translated using back-translation, and interviews in six languages other than Danish were offered. Moreover, all measures of socioeconomic position were registry-based and the validity of these registries is generally considered high (Statistics Denmark 2010b). The study gives explicit attention to the role of sex by analyzing data for men and women separately.
Several methodological limitations should also be noted. First, the cross-sectional design of the study leaves open for interpretation the direction of the association between socioeconomic position and self-rated health, and thus, what we conceptualize as mediator and as outcome. Does immigrant status lead to low socioeconomic position which in turn causes poor health or do factors related to migration cause poor health which in turn leads to low socioeconomic position? First, the direction of the association probably goes both ways since being excluded from the workforce is a well-known risk factor for ill-health and on the other hand, adverse health is the reason why some people are outside the workforce. Second, this is an issue of concern when looking at income and employment status rather than education, which is a more stable measure of socioeconomic position over time (Galobardes et al. 2006a). However, this bias is likely to be an issue of concern among ethnic Danes as well; thus, estimating relative differences between the groups has most likely minimized this bias. Third, the validity of using self-rated health across ethnic groups has been contested with the argument that ethnic groups might attach different meaning to the question of self-rated health (Agyemang et al. 2006). On the contrary, Chandola and Jenkinson (2000) found no ethnic differences in the association between self-rated health and other more objective health measures and concluded that the use of self-rated health is valid across ethnic groups. The cross-cultural validity of self-rated health was not assessed in this study population, which implies that our results must be interpreted with some caution. Back-translation of the questionnaires is likely to have secured the best possible translation of the concept of self-rated health, but it remains a possible bias that cultural differences in interpretation of health and illness could have affected the reference point of the question of self-rated health. Fourth, there was a lower response rate among immigrants and descendants compared to ethnic Danes. This tendency has also been observed in other surveys and might potentially be associated with a lower level of trust in authorities and public institutions (Kristiansen et al. 2006). In addition to this, non-respondents had lower socioeconomic position than respondents and both factors constitute possible selection biases that might have lead to underestimation of the results, as we expect the systematic non-participation to be associated to poor self-rated health. Finally, problems with information bias on the socioeconomic indicators as well as inadequate conceptualization have to be considered as discussed above. Family-size adjusted income would have been preferable but unfortunately this variable was not available at the time of this analysis. Finally, acculturation and different acculturation strategies as potential confounders could have helped to shed light on the findings.
This study documents large inequalities in self-rated health among immigrants and descendants in Denmark that are partly mediated through socioeconomic position. Policies aiming at equity in health across ethnic groups will have to take these socioeconomic disparities into account. Health interventions should be specifically targeted the socioeconomically disadvantaged ethnic minority groups and the underlying causes of these inequalities would have to be targeted through social policies. Further research is needed on the mutual effect on socioeconomic position and ethnic minority status on health. This includes exploring possible interactions between different measures of socioeconomic position. The heterogeneity of non-Western immigrants and inter-generational differences between immigrants and their descendants are underscored by this study, as well as the interactional effects of socioeconomic position and immigrant status. Researchers should take these aspects into consideration when studying different health outcomes of migrants and ethnic minorities. Ultimately, the choice of socioeconomic indicator depends on the specific health outcome under study and the proposed theoretical model.
References
Agyemang C, Denktas S, Bruijnzeels M, Foets M (2006) Validity of the single-item question on self-rated health status in first generation Turkish and Moroccans versus native Dutch in the Netherlands. Public Health 120(6):543–550
Borg V, Kristensen TS (2000) Social class and self-rated health: can the gradient be explained by differences in life style or work environment? Soc Sci Med 51(7):1019–1030
Braveman P, Cubbin C, Marchi K, Egerter S, Chavez G (2001) Measuring socioeconomic status/position in studies of racial/ethnic disparities: maternal and infant health. Public Health Rep 116(5):449–463
Braveman PA, Cubbin C, Egerter S, Chideya S, Marchi KS, Metzler M, Posner S (2005) Socioeconomic status in health research: one size does not fit all. JAMA 294(22):2879–2888
Chandola T, Jenkinson C (2000) Validating self-rated health in different ethnic groups. Ethn Health 5(2):151–159
Cooper H (2002) Investigating socio-economic explanations for gender and ethnic inequalities in health. Soc Sci Med 54(5):693–706
Farmer MM, Ferraro KF (2005) Are racial disparities in health conditional on socioeconomic status? Soc Sci Med 60(1):191–204
Galobardes B, Shaw M, Lawlor DA, Lynch JW, Davey SG (2006a) Indicators of socioeconomic position (part 1). J Epidemiol Community Health 60(1):7–12
Galobardes B, Shaw M, Lawlor DA, Lynch JW, Davey SG (2006b) Indicators of socioeconomic position (part 2). J Epidemiol Community Health 60(2):95–101
Idler EL, Benyamini Y (1997) Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav 38(1):21–37
Iglesias E, Robertson E, Johansson SE, Engfeldt P, Sundquist J (2003) Women, international migration and self-reported health. A population-based study of women of reproductive age. Soc Sci Med 56(1):111–124
Karlsen S, Nazroo JY (2002) Relation between racial discrimination social class and health among ethnic minority groups. Am J Public Health 92(4):624–631
Kawachi I, Daniels N, Robinson DE (2005) Health disparities by race and class: why both matter. Health Aff (Millwood) 24(2):343–352
Krieger N, Williams DR, Moss NE (1997) Measuring social class in US public health research: concepts methodologies, and guidelines. Annu Rev Public Health 18:341–378
Kristiansen M, Mygind A, Krasnik A (2006) Health effects of migration. UgeskrLaeger 168(36):3006–3008
Leao TS, Sundquist J, Johansson SE, Sundquist K (2009) The influence of age at migration and length of residence on self-rated health among Swedish immigrants: a cross-sectional study. Ethn Health 14(1):93–105
Lindstrom M, Sundquist J, Ostergren PO (2001) Ethnic differences in self reported health in Malmo in southern Sweden. J Epidemiol Community Health 55(2):97–103
Lorant V, Van OH, Thomas I (2008) Contextual factors and immigrants’ health status: double jeopardy. Health Place 14(4):678–692
Marmot MG, Shipley MJ, Rose G (1984) Inequalities in death-specific explanations of a general pattern? Lancet 1(8384):1003–1006
Marmot MG, Smith GD, Stansfeld S, Patel C, North F, Head J, White I, Brunner E, Feeney A (1991) Health inequalities among British civil servants: the Whitehall II study. Lancet 337(8754):1387–1393
Nazroo JY (2003) The structuring of ethnic inequalities in health: economic position, racial discrimination, and racism. Am J Public Health 93(2):277–284
Nielsen SS, Krasnik A (2010) Poorer self-perceived health among migrants and ethnic minorities versus the majority population in Europe: a systematic review. Int J Public Health 55(5):357–371
Østergaard B (2007) Indvandrerne i Danmarks historie [Immigrants in the history of Denmark]. Syddansk Universitetsforlag, Odense
Reijneveld SA (1998) Reported health lifestyles and use of health care of first generation immigrants in The Netherlands: do socioeconomic factors explain their adverse position? J Epidemiol Community Health 52(5):298–304
Statistics Denmark (2009) [Immigrants in Denmark] Indvandrere i Danmark, Copenhagen, Denmark
Statistics Denmark (2010a) [News from Statistics Denmark: immigrants and descendents as well as foreign citizens April 1 2010]
Statistics Denmark (2010b) [Quality Documentation] Højkvalitetsdokumentation
Stronks K, Kunst AE (2009) The complex interrelationship between ethnic and socio-economic inequalities in health. J Public Health (Oxf) 31(3):324–325
UNESCO (1997) International classification standard of education
Wiking E, Johansson SE, Sundquist J (2004) Ethnicity, acculturation, and self reported health. A population based study among immigrants from Poland, Turkey, and Iran in Sweden. J Epidemiol Community Health 58(7):574–582
Williams DR, Mohammed SA, Leavell J, Collins C (2010) Race, socioeconomic status, and health: complexities, ongoing challenges, and research opportunities. Ann N Y Acad Sci 1186:69–101
Acknowledgments
We acknowledge the Partnership, constituting of a coalition between the municipalities of Copenhagen, Odense, and Aarhus; the Capital Region; Fynen’s Region; Aarhus Region; the National Board of Health; the National Institute of Public Health, University of Southern Denmark; Department of Public Health, University of Copenhagen for access to the data from the survey “Ethnic Minority Health”. Moreover, we are grateful to the “TrygFonden” for funding for this study. Finally, a special thanks to the study participants.
Conflict of interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Additional information
This paper belongs to the call-for-papers “Migrants and ethnic minorities in Europe: new challenges for public health research and practice”.
Rights and permissions
About this article
Cite this article
Dinesen, C., Nielsen, S.S., Mortensen, L.H. et al. Inequality in self-rated health among immigrants, their descendants and ethnic Danes: examining the role of socioeconomic position. Int J Public Health 56, 503–514 (2011). https://doi.org/10.1007/s00038-011-0264-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-011-0264-6