
Abstract
Objective
Heparin-binding protein (HBP) is a potent inducer of increased vascular permeability. The purpose of this study was to examine plasma levels of HBP in patients with shock.
Design
Fifty-three consecutive patients with septic and non-septic shock at a mixed-bed intensive care unit were included, as well as 20 age-matched controls. Patients with local infections but without signs of shock served as infectious controls. Enzyme-linked immunosorbent assay was used to determine plasma levels of HBP.
Results
There were no differences in serum HBP levels between healthy controls and those with local infections, including urinary tract infections, pneumonia and gastroenteritis, without shock. Levels of HBP were higher in patients with non-septic shock and septic shock than healthy controls. However, there was no difference in serum HBP levels between patients with septic shock and those with non-septic shock. Moreover, HBP levels were not different between patients with low and high APACHE II scores. Plasma levels of HBP were similar in surviving and non-surviving patients with shock.
Conclusions
HBP is elevated in patients with shock from septic and non-septic etiologies. Future investigations are required to define the functional role of HBP in patients with shock.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
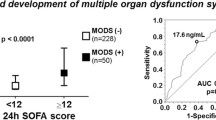
More effective and specific therapies are needed for patients with shock and the high mortality rate in these patients remains a substantial challenge in the health care system. Improved understanding of shock pathophysiology is pivotal for the development of the management of patients with shock [1]. On one hand, neutrophils are recognized as a significant component in the host defense against bacterial invasions. On the other hand, excessive activation of neutrophils causes tissue edema and compromised microvascular perfusion, ultimately leading to organ failure in systemic inflammatory response syndrome (SIRS) and sepsis [2, 3]. Convincing evidence has shown that heparin-binding protein (HBP), also known as azurocidin or cationic antimicrobial peptide (CAP37), an antimicrobial protein stored in neutrophil granules, is a potent inflammatory mediator and may play a functional role in sepsis [4, 5]. HBP is a multifunctional protein exerting numerous pro-inflammatory effects, such as induction of vascular permeability and chemotaxis of monocytes and T-cells [6, 7]. Interestingly, a recent study reported that HBP might be an early biomarker of circulatory failure in septic patients, in whom high levels of HBP preceded development of shock by up to 12 h [8]. Since HBP is thought to participate in increases in vascular permeability, we hypothesized that the role of HBP may extend to patients with systemic inflammation with shock, rather than those with septic shock alone. Plasma levels of HBP in patients with non-septic shock in a mixed group of adult patients have not been examined. Such increases in HBP may open new ways of ameliorating organ damage in patients with systemic inflammation and shock.
The purpose of this study was therefore to investigate whether HBP can discriminate between patients with septic and non-septic shock and whether HBP levels might correlate with acute physiology and chronic health evaluation (APACHE) scores and mortality in patients with shock.
Materials and methods
The Regional Ethical Review Board, Lund, Sweden, approved the study and informed consent was obtained from all patients or their next-of-kin. Patients admitted to the mixed-bed intensive care unit of Skåne University Hospital in Malmö, Sweden between December 2005 and May 2008 were screened for eligibility. For inclusion in this study, patients were over the age of 18, fulfilled the SIRS criteria [9] and exhibited circulatory failure, defined as failure to maintain mean arterial pressure ≥70 mmHg despite adequate fluid resuscitation according to the surviving sepsis campaign algorithm [10]. Exclusion criteria were pregnancy, primary abnormalities of coagulation, fibrinolytic therapy, compromised immunity (i.e. receiving immunosuppressive drugs) or a “Do Not Resuscitate” order. Patients were defined as septic or not based on standard published criteria [11]. 53 consecutive patients were included in the study. All patients were enrolled within 6 h of the diagnosis of shock and blood samples were taken within 10 min after inclusion. Sepsis was defined as a known infection or a suspected infection exhibiting one of the following: leukocytes in a normally sterile body fluid, perforated viscus, radiographic evidence of pneumonia in association with the production of purulent sputum, or a syndrome associated with a high risk of infection and determined at admission. All cultures were reviewed daily during the intensive care unit stay as well as at the end of the study period. APACHE II scores [12] were calculated at admission. All patients were treated according to international guidelines for the management of sepsis and septic shock [10]. No patient received activated protein C. Patients with vasopressor-resistant shock received a low dose of systemic steroids. For comparison, 18 patients with urinary tract infections, pneumonia and gastroenteritis with fever but without signs of shock, and 20 healthy controls were also included for determination of HBP levels in the plasma. Plasma levels of HBP were determined by enzyme-linked immunosorbent assay as described earlier [4, 8]. Based on our previous experience, we calculated a sample size of 18 based on a minimum detectable difference of 10 ± 7 ng/ml between two groups with a power of 0.8 and a sigma of 0.05. Since we expected greater data variability and non-parametric distributions in the sicker patients, we chose to triple the sample size in the shock group. Normality was tested for using the Kolmogorov–Smirnoff test. Data are given as median (range) in the text. Spearman’s rank correlation coefficient was used for correlation between two variables. Kruskal–Wallis one-way ANOVA was used for multiple comparisons. P < 0.05 was considered significant and n indicates the number of patients.
Results
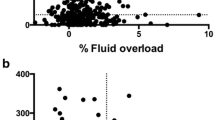
Patients with shock with and without sepsis were similar in terms of age, sex and APACHE II scores in the present study (Table 1). A majority of patients with shock had sepsis (36/53). The etiology of sepsis was varied; some had pre-defined foci and single cultured organisms while others had multiple or undetermined foci and multiple organisms. Gram-positive and Gram-negative organisms were cultured in 15 and 14 patients, respectively, six patients had multiple organisms and one patient had a fungal infection. Many non-septic patients with shock were admitted with pancreatitis (five patients), although the etiology in these patients was also variable and included post-major non-cardiac surgery (five patients), intoxication and multi-organ failure (two patients), and gastrointestinal bleeding and portal hypertension (one patient). In four patients the cause of shock and organ failure were never established, and all cultures of normally sterile fluids were negative. Baseline plasma levels of HBP were 6.3 (5.0–9.7) ng/ml (n = 20) in healthy controls. For comparison, we also measured plasma levels of HBP in urinary tract infections, pneumonia and gastroenteritis. We found no significant difference in HBP levels between healthy controls on one hand and the patients with urinary tract infections, pneumonia or gastroenteritis on the other hand. Plasma levels of HBP in febrile patients with urinary tract infections, pneumonia and gastroenteritis without SIRS were 7.1 (4.4–10.2) ng/ml (n = 8), 7.0 (5.4–10.3) ng/ml (n = 5) and 5.8 (3.7–8.8) ng/ml (n = 5), respectively. In contrast, it was observed that plasma levels of HBP were increased in patients with shock compared to healthy controls (Fig. 1, P < 0.001). Plasma levels of HBP were 24.1 (9.8–125.7) ng/ml (n = 17) and 27.2 (9.0–122.2) ng/ml (n = 36) in patients with non-septic and septic shock, respectively (Fig. 1, P = 0.71). Moreover, we found no significant difference in HBP levels in non-septic and septic patients stratified according to APACHE II scores (Fig. 2a, P = 0.64). The intensive care mortality was 36 and 25% and 6-month mortality was 47 and 25% in patients with non-septic and septic shock, respectively (Table 1). The shock group without sepsis had a higher 6-month mortality rate, although this was not statistically significant (Table 1). In addition, we found that the plasma levels of HBP did not correlate with survival in non-septic and septic patients (Fig. 2b). Systemic leukocyte counts were not significantly different between patients with APACHE II score <20 [9.8 (2.9–19.4) × 109/ml], 20–30 [11.3 (2.9–39.6) × 109/ml] and >30 [12.8 (1.4–53.6) × 109/ml]. We did not find any correlation between HBP levels, on the one hand, and C-reactive protein (r = 0.22, P = 0.11) or plasma levels of interleukin-10 (r = 0.23, P = 0.10) on the other hand in patients with shock.

HBP levels in plasma from healthy controls (n = 20), infectious controls (n = 18) and from septic (n = 36) and non-septic (n = 17) patients with shock. Plasma levels of HBP were significantly higher in both SIRS and sepsis patients compared to healthy and infectious controls (P < 0.001, n = 17–36). Data are median, 10th, 25th, 75th and 90th percentiles

Plasma levels of HBP in healthy controls and patients with shock (SIRS and sepsis) with a different APACHE II scores and b in surviving and non-surviving patients with shock. No significant difference in HBP plasma levels was detected between patients with shock with different APACHE II scores (P = 0.64, n = 20–53) or between surviving and non-surviving patients with shock (P = 0.29, n = 20–53). Data are median, 10th, 25th, 75th and 90th percentiles
Discussion
It is widely held that excessive activation of neutrophils in the circulation constitutes a key component in the pathophysiology of shock. The mechanisms of neutrophil-mediated tissue injury and organ failure in patients with shock remain elusive. Neutrophil-derived HBP has been shown to exert several pro-inflammatory actions that may be of significance in shock [5–7]. Accordingly, in the present study we asked whether HBP might be elevated in patients with shock due to SIRS and sepsis. Indeed, we could document that plasma levels of HBP were significantly enhanced in patients with shock, regardless of whether they suffered from sepsis or not. However, there was no difference in plasma levels of HBP in patients with septic and non-septic shock, suggesting that bacterial infection is not necessary to evoke significant secretion of HBP from neutrophils and that HBP may not be a useful biomarker for patients with suspected septic shock. This notion is supported by in-vitro data showing that not only bacterial products [13] but also non-bacterial cross-linking of β2-integrins on the surface of neutrophils is sufficient to trigger HBP secretion from neutrophils [5]. Moreover, one study revealed that neutrophil activation, determined as an increase in CD11b (Mac-1) on neutrophils, was similar in comparable trauma and sepsis patients [14]. In spite of the fact that HBP is mainly derived from neutrophils [4], we found no statistical relationship between leukocyte counts in the blood on the one hand and plasma levels of HBP on the other hand in patients with shock. Our data did not reveal any correlation between the number of leukocytes in the circulation and disease severity in patients with shock. This observation is in line with a previous study showing that leukocyte count is not a useful marker of intensive care mortality in septic patients [15]. In this context, it should be noted that microbial diagnosis is sometimes complicated in sepsis, which makes it difficult to exclude some overlap between septic and non-septic patients.
Experimental data have shown that HBP is a potent inducer of vascular permeability and leukocyte recruitment [5–7], which are considered to contribute to organ injury in shock [1–3]. However, we did not find any correlation between HBP levels and APACHE II scores. This lack of correlation may either be due to a true absence of relationship or because HBP levels are underestimated in more severe disease. For example, hemodilution due to high fluid administration, leakage into the extravascular space and urine or increased uptake at sites of inflammation may decrease the plasma levels of HBP in patients with more severe disease. Although such factors may cause difficulties in finding a correlation between HBP and disease severity, the relevance of HBP as a potential target in patients with SIRS and sepsis requires further studies. Moreover, a single substance, such as HBP, would most likely respond more promptly to changes in inflammatory activity than the APACHE II score, which is a composite of multiple parameters. In addition, we did not observe any difference in HBP between non-surviving and surviving sepsis patients. These observations are in line with two previous studies reporting that plasma levels of HBP did not correlate with the magnitude of tissue damage in burn patients [16] nor with the frequency of mortality in sepsis patients [17]. In this study, we found that patients with local infections, such as urinary tract infections, pneumonia and gastroenteritis without SIRS did not have higher levels of HBP compared to healthy controls. These findings suggest that systemic inflammation is necessary to stimulate increases in HBP levels in the plasma and HBP may be a common denominator in the pathogenesis of shock rather than being a specific indicator of severe sepsis.
Taken together, these novel findings demonstrate that plasma level of HBP are increased in patients with shock, regardless of whether or not this is due to sepsis. Although the functional role of HBP remains to be determined, our data may pave the way for new therapies to protect against systemic inflammation in patients with shock.
References
Cohen J. The immunopathogenesis of sepsis. Nature. 2002;420:885–91.
Asaduzzaman M, Zhang S, Lavasani S, Wang Y, Thorlacius H. LFA-1 and Mac-1 mediate pulmonary recruitment of neutrophils and tissue damage in abdominal sepsis. Shock. 2008;30:254–9.
Rahman M, Zhang S, Chew M, Ersson A, Jeppsson B, Thorlacius H. Platelet-derived CD40L (CD154) mediates neutrophil upregulation of Mac-1 and recruitment in septic lung injury. Ann Surg. 2009;250:783–90.
Tapper H, Karlsson A, Mörgelin M, Flodgaard H, Herwald H. Secretion of heparin-binding protein from human neutrophils is determined by its localization in azurophilic granules and secretory vesicles. Blood. 2002;99:1785–93.
Gautam N, Olofsson AM, Herwald H, Iversen LF, Lundgren-Akerlund E, Hedqvist P, Arfors KE, Flodgaard H, Lindbom L. Heparin-binding protein (HBP/CAP37): a missing link in neutrophil-evoked alteration of vascular permeability. Nat Med. 2001;7:1123–7.
Soehnlein O, Zernecke A, Eriksson EE, Rothfuchs AG, Pham CT, Herwald H, Bidzhekov K, Rottenberg ME, Weber C, Lindbom L. Neutrophil secretion products pave the way for inflammatory monocytes. Blood. 2008;112:1461–71.
Chertov O, Michiel DF, Xu L, Wang JM, Tani K, Murphy WJ, Longo DL, Taub DD, Oppenheim JJ. Identification of defensin-1, defensin-2, and CAP37/azurocidin as T-cell chemoattractant proteins released from interleukin-8-stimulated neutrophils. J Biol Chem. 1996;271:2935–40.
Linder A, Christensson B, Herwald H, Björck L, Akesson P. Heparin-binding protein: an early marker of circulatory failure in sepsis. Clin Infect Dis. 2009;49:1044–50.
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM consensus conference committee. Chest. 1992;101:1644–55.
Dellinger RP, Carlet JM, Masur H, Gerlach H, Calandra T, Cohen J, Gea-Banacloche J, Keh D, Marshall JC, Parker MM, Ramsay G, Zimmerman JL, Vincent JL, Levy MM. Surviving sepsis campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32:858–73.
Bernard GR, Vincent JL, Laterre PF, LaRosa SP, Dhainaut JF, Lopez-Rodriguez A, Steingrub JS, Garber GE, Helterbrand JD, Ely EW, Fisher CJ Jr. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001;344:699–709.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. Prognosis in acute organ system failure. Ann Surg. 1985;202:685–93.
Påhlman LI, Mörgelin M, Eckert J, Johansson L, Russell W, Riesbeck K, Soehnlein O, Lindbom L, Norrby-Teglund A, Schumann RR, Björck L, Herwald H. Streptococcal M protein: a multipotent and powerful inducer of inflammation. J Immunol. 2006;177:1221–8.
Nakae H, Endo S, Inada K, Takakuwa T, Kasai T. Changes in adhesion molecule levels in sepsis. Res Commun Mol Pathol Pharmacol. 1996;91:329–38.
Silvestre J, Povoa P, Coelho L, Almeida E, Moreira P, Fernandes A, Mealha R, Sabino H. Is CRP a good prognostic marker in septic patients? Int Care Med. 2009;35:909–13.
Johansson J, Lindbom L, Herwald H, Sjöberg F. Neutrophil-derived heparin binding protein––a mediator of increased vascular permeability after burns? Burns. 2009;35:1185–7.
Berkestedt I, Herwald H, Ljunggren L, Nelson A, Bodelsson M. Elevated plasma levels of antimicrobial polypeptides in patients with severe sepsis. J Innate Immun. 2010;2:478–82.
Acknowledgments
This work was supported by grants from the Swedish Medical Research Council (2007-7480 and 2009-4872), Crafoord foundation, Einar and Inga Nilsson foundation, Harald and Greta Jaensson foundation, Greta and Johan Kock foundation, Fröken Agnes Nilsson foundation, Franke and Margareta Bergqvist foundation, Magnus Bergvall foundation, Mossfelt foundation, Nanna Svartz foundation, Ruth and Richard Julin foundation, Svenska Läkaresällskapet, MAS foundations, Scandinavian Society for Anesthesiology and Intensive Care Acta Foundation, Malmö University Hospital and Lund University. None of these funding bodies were involved in the study design, data collection, analysis, manuscript preparation or submission. We thank Monica Heidenholm for excellent technical assistance.
Conflict of interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible Editor: Artur Bauhofer.
Rights and permissions
About this article
Cite this article
Chew, M.S., Linder, A., Santen, S. et al. Increased plasma levels of heparin-binding protein in patients with shock: a prospective, cohort study. Inflamm. Res. 61, 375–379 (2012). https://doi.org/10.1007/s00011-011-0422-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-011-0422-6