
Abstract
Objective
To investigate the influence of oxymatrine (OMT) on Toll-like receptor 4 (TLR-4)/nuclear factor kappa-B (NF-κB)-dependent inflammatory responses and neuronal cell apoptosis after traumatic brain injury (TBI).
Materials and methods
Wistar rats were given an intraperitoneal injection of 60 or 120 mg/kg OMT after TBI once a day till day 5. Rats were killed by decapitation at hours 2, 6 and 12, and days 1, 2, 3 and 5 after TBI. Gene expressions of TLR-4 and NF-κB, concentrations of tumor necrosis factor-alpha (TNF-α), interleukin-1beta (IL-1β) and interleukin-6 (IL-6) as well as the number of apoptotic neuronal cells in traumatic rat brain tissues were determined.
Results
The administration of 120 mg/kg OMT could significantly suppress gene expressions of TLR-4 and NF-κB, lessen concentrations of TNF-α, IL-1β and IL-6, and reduce the number of apoptotic neuronal cells in traumatic rat brain tissues by the Mann–Whitney U test (P < 0.05), but the administration of 60 mg/kg OMT could not (P > 0.05).
Conclusion
OMT may inhibit TLR4/NF-κB-dependent inflammatory responses, and furthermore lessen neuronal cell apoptosis after TBI.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Traumatic brain injury (TBI), a leading cause of death and disability, is the result of an outside force causing mechanical disruption of brain tissue and delayed pathogenic events which collectively exacerbate the injury [1]. Inflammation and apoptosis are involved in the pathological process after TBI. The inflammatory cytokines activate nuclear factor kappa-B (NF-κB) through Toll-like receptor 4 (TLR4)–NF-κB signal transduction pathways, promote target gene activation, such as tumor necrosis factor-alpha (TNF-α), interleukin-1beta (IL-1β) and interleukin-6 (IL-6), and ultimately induce neuronal apoptosis [2–11].
As a potent monosomic alkaloid extracted from traditional Chinese medicinal herbs Sophora flavescens and S. subprostrata, oxymatrine (OMT) was originally used for the treatment of chronic viral hepatitis [12, 13]. Recently, it was reported that OMT could inhibit inflammatory brain injury, weaken cerebral edema, and provide neuroprotection against subsequent cerebral ischemic injury [14–16]. However, there have been few reports on the influence of OMT on TBI. This study investigated the effects of intraperitoneal OMT on gene expression of TLR4 and NF-κB, concentration of TNF-α, IL-1β and IL-6, and the number of apoptotic neuronal cells in traumatic rat brain tissues.
Materials and methods
Animal preparation
A total of 140 male Wistar rats (weight 250–300 g; the Animal Center of the Chinese Academy of Sciences, Shanghai, China) were used in the present study. The rats were housed in temperature- and humidity-controlled animal quarters with a 12-h light/dark cycle. All experimental protocols complied with the Laboratory Animal Care and Use Guidelines of the First Hangzhou Municipal People’s Hospital of Nanjing Medical University.
The rats were anesthetized by intraperitoneal injection of pentobarbital (50 mg/kg). A right parietal craniotomy (diameter 5 mm) was drilled under aseptic conditions 1 mm posterior and 2 mm lateral to the bregma. Trauma was induced by a modification of Feeney’s weight-drop model [17] in which a freefalling weight drops onto the exposed intact cranial dura to produce a standardized parietal contusion. A steel rod (weight 40 g) with a flat end diameter of 4 mm was allowed to fall from a height of 25 cm onto a piston resting on the dura. The piston was allowed to compress the brain tissue a maximum of 5 mm. After this procedure, the rats were returned to their cages and the room temperature kept at 23 ± 1°C. Heart rate, arterial blood pressure and rectal temperature were monitored, and the rectal temperature was kept at 37 ± 0.5°C by physical cooling (ice bag) when required throughout the experiment. The rats in the sham operation groups were anesthetized, and their scalps were cut and sutured, but were not trephinated.
Drug preparation
OMT (98% purity) was purchased from Shanxi Huike Botanical Development Company Limited (Shanxi, China). The fine powder of OMT was prepared as a suspension (40 mg/mL) with distilled water and stored at 4°C.
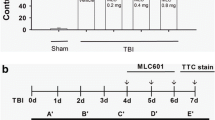
Experimental protocol
Rats were divided into four groups: low and high OMT treatment group, TBI group, and sham operation group. OMT suspension (40 mg/mL) was given to rats in the low and high OMT treatment groups via intraperitoneal injection (60 and 120 mg/kg) after TBI, and then once a day. The rats in the TBI and sham operation groups received an intraperitoneal administration of 1 mL of saline after TBI or procedures, and then once a day. Animals were killed by decapitation under deep pentobarbital anesthesia (80 mg/kg, intraperitoneally) at hours 2, 6 and 12, and days 1, 2, 3 and 5 after TBI (n = 5 for each subgroup). Brains were removed immediately, and the surrounding brain tissue of the injured cortex was dissected on ice as described in the previous study [5]; a portion of the tissue was fixed in 10% buffered formalin, and the remainder was immediately stored at −70°C until analysis.
Reverse transcription polymerase chain reaction (RT-PCR) analysis
Total RNA was extracted with Trizol (Invitrogen) and the density and purity determined. RNA (2 μg) of each sample was used for synthesizing cDNA through inverse transcription; 1 μL of cDNA was used to carry out PCR amplification. Primers were synthesized by Shanghai Sangon Biological Engineering Technology Company Limited. Correctness of the gene order was proved in GenBank. Primers were 5′-GCC GGA AAG TTA TTG TGG TGG T-3′ (forward) and 5′-ATG GGT TTT AGG CGC AGA GTT T-3′ (reverse) for TLR4, 5′-GCG CAT CCA GAC CAA CAA TAA C-3′ (forward) and 5′-GCC GAA GCT GCA TGG ACA CT-3′ (reverse) for NF-κB, and 5′-GCC ATG TAC GTA GCC ATC CA-3′ (forward) and 5′-GAA CCG CTC ATT GCC GAT AG-3′ (reverse) for β-actin. PCR conditions were initial denaturation for 2 min at 95°C, 35 cycles of amplification with denaturation at 95°C for 30 s, annealing at 52°C for 30 s, and extension at 72°C for 40 s, with a final extension at 72 °C for 5 min. RT-PCR products (5 μL) were analyzed by 2% agarose gel electrophoresis. The gray scale of the electrophoresis strip was scanned by an ultraviolet photometry (UVP) gel imaging system. The relative expression of products was represented with TLR4/β-actin and NF-κB/β-actin ratios; data were analyzed with an image analysis system.
Determination of inflammatory cytokines in traumatic brain tissue
The tissues were diluted (40% weight/volume) with 0.01 mol/L phosphate-buffered saline (PBS), pH 7.4, containing a protease inhibitor cocktail (Roche, Indianapolis, IN, USA), and homogenized. The homogenates were then centrifuged at 7,500g for 20 min at 4°C. The levels of TNF-α, IL-1β and IL-6 in the supernatant were determined by enzyme-linked immunosorbent assay using commercial kits (R&D Systems, Minneapolis, MN, USA) in accordance with the manufacturer’s instructions. Results were expressed as picograms per milligram (pg/mg) of brain tissue.
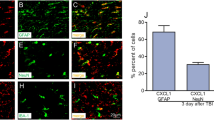
TUNEL staining
The formalin-fixed brain tissues were embedded in paraffin and sectioned at 4 μm with a microtome. The sections were examined for apoptotic cells by the terminal deoxynucleotidyl transferase-mediated dUTP nick end-labeling (TUNEL) method, using an in situ cell death detection kit (ISCDD, Boehringer Mannheim, Germany), according to the manufacturer’s protocol. Briefly, sections were deparaffinized, rehydrated, and washed with distilled water. The tissues were digested with 20 μg/mL proteinase K (Boehringer Mannheim) at room temperature for 15 min. Endogenous peroxidase activity was blocked by incubation in 0.3% hydrogen peroxide/methanol in PBS at 37°C for 30 min. The sections then were incubated with terminal deoxynucleotidyl transferase at 37°C for 60 min to add dioxigenin-conjugated dUTP to the 3′-OH ends of fragmented DNA. Anti-dioxigenin antibody peroxidase was applied to the sections in order to detect the labeled nucleotides. The sections were stained with DAB and counterstained lightly with hematoxylin. The apoptotic cells were identified and counted using light microscopy by an investigator who was blinded to the grouping. The extent of neurological damage was evaluated by the apoptotic index (i.e., the mean number of positive neuronal cells per 100 neuronal cells, based on examination of 1,000 neuronal cells).
Statistical analysis
All data in this study were presented as median (lower quartile, upper quartile). Statistical analysis was performed with SPSS 10.0 software (SPSS Inc., Chicago, USA). All data were analyzed by the Mann–Whitney U test. Significance levels were set at P < 0.05.
Results
In the sham operation group, the rat brain tissues showed normal structure. TBI caused severe pathological brain damage such as inflammation, microglial reaction and neuronal injury. The rat brain tissues in the high-dose OMT treatment group showed less inflammation, microglial reaction and neuronal injury than those in the TBI group, but the inflammation, microglial reaction and neuronal injury of the rat brain tissues in the low-dose OMT treatment group was not obviously lessened.
After TBI, gene expressions of TLR4 and NF-κB, concentrations of TNF-α, IL-1β and IL-6, and numbers of apoptotic neuronal cells in traumatic rat brain tissues increased during the 2-h period immediately, peaked in 1 day, plateaued at day 2, and decreased gradually thereafter, and were substantially higher than those in the sham operation group during the 5-day period (Tables 1, 2, 3, 4, 5, 6).
At hours 2, 6 and 12, and days 1, 2, 3 and 5 after TBI, gene expressions of TLR4 and NF-κB, concentrations of TNF-α, IL-1β and IL-6, and numbers of apoptotic neuronal cells in traumatic rat brain tissues in the low-dose OMT treatment group were lower than those in the TBI group, but these differences did not reach statistical significance (Table 1, 2, 3, 4, 5, 6).
At hours 2 and 6 after TBI, gene expressions of TLR4 and NF-κB, concentrations of TNF-α, IL-1β and IL-6, as well as numbers of apoptotic neuronal cells in traumatic rat brain tissues in the high-dose OMT treatment group were lower than those in the TBI group, but these differences did not reach statistical significance (Tables 1, 2, 3, 4, 5, 6). At hour 12 and days 1, 2, 3 and 5 after TBI, gene expressions of TLR4 and NF-κB, concentrations of TNF-α, IL-1β and IL-6, and numbers of apoptotic neuronal cells in traumatic rat brain tissues in the high-dose OMT treatment group were significantly lower than those in TBI group (Tables 1, 2, 3, 4, 5, 6).
Discussion
TLRs are a family of transmembrane proteins and act as signal transduction molecules [18]. Activation of TLRs recruits downstream signaling proteins and results in transcription of genes encoding inflammation-associated molecules and cytokines. For example, combined with specific ligand, the activation of TLR4, the first mammalian TLR recognized, induces the phosphorylation of inhibitor of kappa-B and dissociates inhibitor of kappa-B from NF-κB. NF-κB then translocates into the nucleus and activates and regulates the transcription of genes related to inflammatory responses such as TNF-α, IL-1β and IL-6 [19, 20]. Accumulating evidence demonstrates that TLR4/NF-κB signaling contributes to inflammatory responses, and therefore induces neuronal apoptosis in TBI [2–11].
OMT has shown a variety of pharmacological actions. It is proven to protect ischemic and reperfusion injury in liver, intestine and heart via anti-inflammation and anti-apoptosis [12, 21, 22]. Recently, several studies have confirmed that OMT protects the brain from ischemic injury by an inhibition of the inflammatory reaction. Liu and collaborators investigated the potential neuroprotective role of oxymatrine in cerebral ischemia and found that OMT reduced infarct volume through a decrease in NF-κB expression [14]. Moreover, it was shown that OMT protected the brain from damage caused by middle cerebral artery occlusion through down-regulation of 12/15-lipoxygenase, phosphorylated p38 mitogen-activated protein kinase and cytosolic phospholipase A2 [15], as well as TLR4, TLR2, myeloid differentiation factor 88 and NF-κB [16]. Our study showed that inflammation, microglial reaction and neuronal injury were obviously lessened, and the levels of gene expression of TLR4 and NF-κB, the concentrations of TNF-α, IL-1β and IL-6, and the number of apoptotic neuronal cells were significantly decreased in traumatic rat brain tissue after an intraperitoneal administration of 120 mg/kg OMT. As expected, the temporal profiles of the expressions of TLR4 and NF-κB were similar to those of the concentrations of TNF-α, IL-1β and IL-6 as well as the number of apoptotic neuronal cells. It was suggested that OMT may ameliorate the inflammation by suppressing the expression of TLR4 and NF-κB in microglial cells, and furthermore reduce neuronal cell apoptosis after TBI.
Conclusion
OMT may inhibit TLR4/NF-κB-dependent inflammatory responses, and furthermore lessen neuronal cell apoptosis after TBI.
References
Gaetz M. The neurophysiology of brain injury. Clin Neurophysiol. 2004;115:4–18.
Hang CH, Chen G, Shi JX, Zhang X, Li JS. Cortical expression of nuclear factor kappaB after human brain contusion. Brain Res. 2006;1109:14–21.
Chen G, Shi J, Jin W, Wang L, Xie W, Sun J, Hang C. Progesterone administration modulates TLRs/NF-kappaB signaling pathway in rat brain after cortical contusion. Ann Clin Lab Sci. 2008;38:65–74.
Chen G, Zhang S, Shi J, Ai J, Qi M, Hang C. Simvastatin reduces secondary brain injury caused by cortical contusion in rats: possible involvement of TLR4/NF-kappaB pathway. Exp Neurol. 2009;216:398–406.
Hang CH, Shi JX, Tian J, Li JS, Wu W, Yin HX. Effect of systemic LPS injection on cortical NF-kappaB activity and inflammatory response following traumatic brain injury in rats. Brain Res. 2004;1026:23–32.
Lu J, Goh SJ, Tng PY, Deng YY, Ling EA, Moochhala S. Systemic inflammatory response following acute traumatic brain injury. Front Biosci. 2009;14:3795–813.
Morganti-Kossmann MC, Rancan M, Otto VI, Stahel PF, Kossmann T. Role of cerebral inflammation after traumatic brain injury: a revisited concept. Shock. 2001;16:165–77.
Bermpohl D, You Z, Lo EH, Kim HH, Whalen MJ. TNF alpha and Fas mediate tissue damage and functional outcome after traumatic brain injury in mice. J Cereb Blood Flow Metab. 2007;27:1806–18.
Raghupathi R. Cell death mechanisms following traumatic brain injury. Brain Pathol. 2004;14:215–22.
Raghupathi R, Graham DI, McIntosh TK. Apoptosis after traumatic brain injury. J Neurotrauma. 2000;17:927–38.
Wong J, Hoe NW, Zhiwei F, Ng I. Apoptosis and traumatic brain injury. Neurocrit Care. 2005;3:177–82.
Xiang X, Wang G, Cai X, Li Y. Effect of oxymatrine on murine fulminant hepatitis and hepatocyte apoptosis. Chin Med J. 2002;115:593–6.
Zeng Z, Wang GJ, Si CW. Basic and clinical study of oxymatrine on HBV infection. J Gastroenterol Hepatol. 1999;14:S295–7.
Liu Y, Zhang XJ, Yang CH, Fan HG. Oxymatrine protects rat brains against permanent focal ischemia and downregulates NF-kappaB expression. Brain Res. 2009;1268:174–80.
Cui L, Zhang X, Yang R, Wang L, Liu L, Li M, Du W. Neuroprotection and underlying mechanisms of oxymatrine in cerebral ischemia of rats. Neurol Res. 2010; doi:10.1179/016164110X12759951866876.
Fan H, Li L, Zhang X, Liu Y, Yang C, Yang Y, Yin J. Oxymatrine downregulates TLR4, TLR2, MyD88, and NF-kappaB and protects rat brains against focal ischemia. Mediators Inflamm. 2009; doi:10.1155/2009/704706.
Feeney DM, Boyeson MG, Linn RT, Murray HM, Dail WG. Responses to cortical injury: I. Methodology and local effects of contusions in the rat. Brain Res. 1981;211:67–77.
Aderem A, Ulevitch RJ. Toll-like receptors in the induction of the innate immune response. Nature. 2000;406:782–7.
Akira S, Takeda K, Kaisho T. Toll-like receptors: critical proteins linking innate and acquired immunity. Nat Immunol. 2001;2:675–80.
Anderson KV. Toll signaling pathways in the innate immune response. Curr Opin Immunol. 2000;12:13–9.
Hong-Li S, Lei L, Lei S, Dan Z, De-Li D, Guo-Fen Q, Yan L, Wen-Feng C, Bao-Feng Y. Cardioprotective effects and underlying mechanisms of oxymatrine against ischemic myocardial injuries of rats. Phytother Res. 2008;22:985–9.
Zhao J, Yu S, Tong L, Zhang F, Jiang X, Pan S, Jiang H, Sun X. Oxymatrine attenuates intestinal ischemia/reperfusion injury in rats. Surg Today. 2008;38:931–7.
Acknowledgments
This work is financially supported by the Traditional Chinese Medicine Department of Zhejiang Province, No. 2010ZA101.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible Editor: Artur Bauhofer.
X.-Q. Dong and W.-H. Yu contributed equally.
Rights and permissions
About this article
Cite this article
Dong, XQ., Yu, WH., Hu, YY. et al. Oxymatrine reduces neuronal cell apoptosis by inhibiting Toll-like receptor 4/nuclear factor kappa-B-dependent inflammatory responses in traumatic rat brain injury. Inflamm. Res. 60, 533–539 (2011). https://doi.org/10.1007/s00011-010-0300-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-010-0300-7