
Abstract
Background: Operations for patients with colorectal cancer are based on traditions established by historical experience. Radioimmunoguided surgery (RIGS) provides new information that challenges these traditions.
Methods: Thirty-two patients with primary colorectal cancer underwent RIGS after being injected with anti-TAG-72 murine monoclonal antibody CC49 labeled with iodine-125. Sixteen of the patients had all gross tumor and RIGS-positive tissue removed (RIGS-negative group), and 16 had only traditional extirpation of the tumor because RIGS-positive tissue was too diffuse (RIGS-positive group).
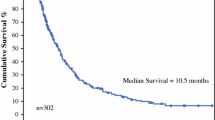
Results: In the 16 patients having all RIGS-positive tissue removed, five had traditional regional en bloc resections and 11 had additional extraregional tissues resected. Identification of extraregional disease added two liver resections and 25 lymphadenectomies: 10 of the gastrohepatic ligament, five celiac axis, six retroperitoneal, and four iliac. With a median follow-up of 37 months, survival in the RIGS-negative group is 100%. In 14 of 16 patients (87.5%) there is no evidence of disease. In the RIGS-positive group, follow-up shows 14 of 16 patients are dead and two are alive with disease (p<0.0001).
Conclusion: These results suggest that RIGS identifies patterns of disease dissemination different from those identified by traditional staging techniques. Removal of additional RIGS-positive tissues in nontraditional areas may improve survival.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Cohen AM, Minsky BO, Schilsky RL. Colon cancer. In: DeVita V Jr, Hellman S, Rosenberg SA, eds.Cancer: principles and practice of oncology. 4th ed. Philadelphia: JB Lippincott, 1993:929–77.
Miles WE. A method of performing abdominoperineal resection for carcinoma of the rectum and of the terminal portion of the pelvic colon.Lancet 1908;2:1812.
Jamieson JK, Dobson JF. The lymphatics of the colon: with special reference to the operative treatment of cancer of the colon.Ann Surg 1909;50:1077–90.
Rouviere H.Anatomy of the human lymphatic system [translated by MJ Tobias]. Ann Arbor: Edward Brothers, 1909;188–92.
Moynihan BGA. Cancer of the sigmoid colon and rectum.Surg Gynecol Obstet 1908;6:463.
Beahrs OH, Henson DE, Hutter RVP, Kennedy BJ.Manual for staging of cancer. 4th ed. Philadelphia: JB Lippincott, 1992.
Enker WE, Laffer UT, Block GE. Enhanced survival of patients with colon and rectal cancer is based upon wide anatomical resection.Ann Surg 1979;190:350–60.
Gardner B. Five year survival after extended resection for colon cancer.J Surg Oncol 1987;34:258–61.
Wangensteen OH, Lewis PJ, Tongen LA. The “second look” in cancer surgery.Lancet 1951;71:303.
Steele G. The surgical oncologist as a key translator of basic biology to patients with gastrointestinal cancer: asking the right questions.Ann Surg 1994;1:262–9.
Author information
Authors and Affiliations
Additional information
All authors of this article are paid consulting fees by Neoprobe Corporation, Dublin, Ohio. Neoprobe is the supplier of the CC49 monoclonal antibody and the Neoprobe 1000 instrument and funds studies with the RIGS technology. In addition, Dr. Martin is a cofounder of Neoprobe.
Rights and permissions
About this article
Cite this article
Bertsch, D.J., Burak, W.E., Young, D.C. et al. Radioimmunoguided surgery for colorectal cancer. Annals of Surgical Oncology 3, 310–316 (1996). https://doi.org/10.1007/BF02306288
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02306288