
Summary
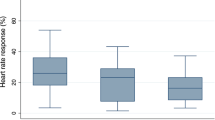
Several studies have shown that coronary vasodilator reserve is impaired in some patients with chest pain and angiographically normal coronary arteries. In a subgroup of these patients, who additionally show ST depression on the electrocardiogram during exercise and are generally labelled as having Syndrome X, the impairment of coronary flow reserve is associated with metabolic and functional signs consistent with an increased sympathetic drive. The aim of the present investigation was to ascertain whether the impairment of coronary vasodilator reserve in patients with Syndrome X is due to adrenergically mediated vasoconstriction of coronary microcirculation. Myocardial blood flow (MBF), at baseline and following intravenous infusion of dipyridamole (0.56 mg/kg over 4 minutes), was measured by means of13N-ammonia and dynamic positron emission tomography in 10 females (mean age 52±8 years) with a chest pain history, ST-segment depression during exercise, and angiographically normal coronaries. The first MBF study was performed while the patients were off therapy; a repeat MBF study was performed following 1 week of treatment with the alpha-1 blocker doxazosin (2 mg/day). Off therapy MBF was 1.13±0.25 ml/min/g at baseline and increased to 2.35±0.66 ml/min/g following dipyridamole. Coronary vasodilator reserve (dipyridamole/baseline MBF) was 2.18±0.56. During treatment with doxazosin, baseline MBF was not different from the control value (1.25±0.50 ml/min/g), while added dipyridamole significantly increased MBF to 3.52±1.20 ml/min/g (p<0.01 vs. off therapy). Coronary vasodilator reserve was significantly increased (2.91±0.92, p<0.01 vs. control value) by doxazosin. This study indicates that alpha-1 adrenoceptors might play a role in the reduction of coronary reserve in patients with Syndrome X. Further clinical studies are needed to ascertain the efficacy of alpha-1 blockers for the treatment of such patients.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Opherk D, Zebe H, Weihe E, et al. Reduced coronary dilatory capacity and ultrastructural changes of the myocardium in patients with angina pectoris but normal coronary arteriograms.Circulation 1981;63:817–825.
Cannon RO, Epstein SE. “Microvascular angina” as a cause of chest pain with angiographically normal coronary arteries.Am J Cardiol 1988;61:1338–1343.
Epstein SE, Cannon RO. Site of increased resistance to coronary flow in patients with angina pectoris and normal epicardial coronary arteries.J Am Coll Cardiol 1986;8:459–461.
Camici PG, Marraccini P, Lorenzoni R, et al. Coronary hemodynamics and myocardial metabolism in patients with Syndrome X: Response to pacing stress.J Am Coll Cardiol 1991;17:1461–1470.
Chilian WM, Eastman CL, Layne SM, Marcus ML. Small vessel phenomena in the coronary microcirculation: Phasic intramyocardial perfusion and coronary microvascular dynamics.Prog Cardiovasc Dis 1988;31:17–38.
Heusch G. Alpha adrenergic mechanisms in myocardial ischemia.Circulation 1990;81:1–13.
Bellina RC, Parodi O, Camici PG, et al. Simultaneous in vitro and in vivo validation of13N-ammonia for the assessment of regional myocardial blood flow.J Nucl Med 1990;31:1335–1343.
Camici PG, Chiriatti G, Lorenzoni R, et al. Coronary vasodilation is impaired in both hypertrophied and nonhypertrophied myocardium of patients with hypertrophic cardiomyopathy: A study with nitrogen-13 ammonia and positron emission tomography.J Am Coll Cardiol 1991;17:879–886.
Vaaburg W, Kamphuis JAA, Beerling-van der Molen HB, et al. An improved method for the cyclotron production of13N-labeled ammonia.Int J Amm Rad Isot 1975;26:316–318.
Spinks TJ, Guzzardi R, Bellina CR. Performance characteristics of a whole body positron tomograph.J Nucl Med 1988;29:1833–1841.
Bergmann SR, Herrero P, Markham J, Weinheimer CJ, Walsh MN. Noninvasive quantitation of myocardial blood flow in human subjects with oxygen-15-labeled water and positron emission tomography.J Am Coll Cardiol 1989;14:639–652.
Araujo LI, Lammertsma AA, Rhodes CG, et al. Noninvasive quantification of regional myocardial blood flow in coronary artery disease with oxygen-15-labeled carbon dioxide inhalation and positron emission tomography.Circulation 1990;83:875–885.
White CW, Wilson RF, Marcus ML. Methods of measuring myocardial blood flow in humans.Prog Cardiovasc Dis 1988;31:79–94.
Chilian WM, Layne SM, Easthman CL, Marcus ML. Heterogeneous microvascular coronary alpha-adrenergic vasoconstriction.Circ Res 1989;64:376–388.
Murray RA, Vatner SF. Alpha-adrenoceptor attenuation of the coronary vascular response to severe exercise in the conscious dog.Circ Res 1979;45:654–660.
Bache RJ, Homans DC, Dai XZ. Adrenergic vasoconstriction limits coronary blood flow during exercise in hypertrophied left ventricle.Am J Physiol 1991;260:H1489-H1494.
Hodgson JM, Cohen MD, Szentpetery S, Thames MD. Effects of regional alpha- and beta-blockade on resting and hyperemic coronary blood flow in conscious, unstressed humans.Circulation 1989;79:797–809.
Berry JJ, Baker JA, Pieper KS, Hanson MW, Hoffman JM, Coleman RE: The effect of metabolic milieu on cardiac PET imaging using fluorine-18-deoxyglucose and nitrogen-13-ammonia in normal volunteers.J Nucl Med 1991;32:1518–1525.
Geltman EM, Henes CG, Senneff MJ, Sobel BE, Bergmann SR: Increased myocardial perfusion at rest and diminished perfusion reserve in patients with angina and angiographically normal coronary arteries.J Am Coll Cardiol 1990;16:586–595.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Camici, P.G., Marraccini, P., Gistri, R. et al. Adrenergically mediated coronary vasoconstriction in patients with Syndrome X. Cardiovasc Drug Ther 8, 221–226 (1994). https://doi.org/10.1007/BF00877330
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00877330