
Objective: To estimate the risk of cesarean delivery due to excess prepregnancy body mass index (BMI) in a multistate, US population-based sample. Methods: We analyzed data from the population-based Pregnancy Risk Assessment Monitoring System (PRAMS) on 24,423 nulliparous women with single, term infants delivered between 1998 and 2000 in 19 states. We calculated BMI from self-reported weight and height. We assessed interactions between prepregnancy BMI and other risk factors. We estimated weighted relative risks and 95% confidence intervals for the association between prepregnancy BMI and cesarean section from multiple logistic regression models adjusting for demographic and medical risk factors from the PRAMS questionnaire or birth certificates. Results: The incidence of cesarean delivery increased with increased prepregnancy BMI, from 14.3% (0.8 standard error (SE)) for lean women (BMI < 19.8) to 42.6% (2.0 SE) for very obese women (BMI ≥ 35). The risk of cesarean section differed by presence of any medical, labor and/or delivery complication. Among women with any complication, the estimated adjusted RR for cesarean delivery was 1.1 (95% confidence interval (CI) 1.0–1.2) among overweight women, 1.3 (95% CI 1.1–1.4) among obese women, and 1.4 (95% CI 1.2–1.6) among very obese women compared with normal weight women. Among women without any complications, the estimated adjusted RR was 1.4 (95% CI 1.0–1.8) among overweight women, 1.5 (95% CI 1.1–2.1) among obese women, and 3.1 (95% CI 2.3–4.8) among very obese women. Conclusion: Excess prepregnancy weight increases the risk of cesarean delivery among nulliparous women giving birth to single, term infants, especially among very obese women without any complications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
In 1996, the US cesarean delivery rate began to rise, ending a decline that began in 1989 (1). Between 1996 and 2002, the overall cesarean delivery rate increased 25%, from 20.7 to 26.1%, and the primary cesarean section rate increased 23%, from 14.6 to 18.0% (1). Obesity among US women is also on the rise. During the decade of the 1990s, the percentage of US women who were obese increased 32%, from 25.9 to 34.0% (2). While the increasing rate in cesarean sections reflects changes in many areas, including demographics, physician practices, and maternal choice (1), it also may be influenced by changes in women's prepregnancy weight.
Studies have reported an increased risk of cesarean delivery in women who are obese. Studies confined to clinic-based samples have found up to 4 times greater odds of delivery by cesarean section among obese women than among normal or lean women (3–5), or a positive linear association between prepregnancy BMI and cesarean delivery (6, 7). Three population-based studies, two in Sweden and another in a perinatal region of New York State, found similar results (8–10). Obese women are not only at increased risk of cesarean delivery, but they are also at increased risk of infection and other complications from the surgery compared to nonobese women (11).
The biological pathway through which obesity affects the labor process is not well understood, although dystocia due to increases in pelvic soft tissue has been proposed (4, 9). A study of women in a middle-class private practice found obese women (BMI > 30) were 6 times more likely to have a cesarean section due to cephalopelvic disproportion/failure to progress than nonobese women (4), and another study found morbidly obese women had 2.6 greater odds of experiencing failure to progress than nonobese women (12). While no difference has been found in the length of the second stage of labor, obese women are more likely to have a decreased dilation rate, and a longer active phase of labor and to require oxytocin augmentation than normal weight women (13, 14). Another pathway in which obesity could affect the risk of cesarean delivery is by increasing the risk of diabetes or hypertension, which in turn, increases the risk of cesarean delivery.
The purpose of this study was to estimate the risk of cesarean delivery by level of prepregnancy body mass index (BMI) in a large multistate, US population-based sample and to assess potential interactions with other risk factors for cesarean delivery to better understand the mechanisms through which obesity increases the risk of cesarean delivery.
MATERIALS AND METHODS
We analyzed data from the Pregnancy Risk Assessment Monitoring System (PRAMS), which was established in 1988 to provide state-specific surveillance of maternal attitudes and experiences before, during, and shortly after pregnancy. Currently, 32 states conduct PRAMS surveillance. Our study used data from 19 states that had annual response rates of 70% or higher (Alabama 1998–2000, Alaska 1998–2000, Arkansas 1998–2000, Colorado 1998–2000, Florida 1998–2000, Hawaii 2000, Illinois 1998–2000, Louisiana 1998–2000, Maine 1998–2000, Nebraska 2000, New Mexico 1999–2000, New York State/excluding New York City 1998–2000, North Carolina 1998–2000, Ohio 1999–2000, Oklahoma 1998–2000, South Carolina 1998–2000, Utah 1999–2000, Washington State 1998–2000, and West Virginia 1998–2000). The overall response rate was 75%, and the state's individual response rates ranged from 70 to 80%.
Each state used a similar methodology for conducting PRAMS. Every month, a stratified systematic sample of 100–200 new mothers was selected from birth certificates. Stratification variables were determined by each state, many of which chose birth weight. Each mother was mailed a 14-page questionnaire 1–3 months after delivery. If the mother failed to respond, a second, and if needed, a third questionnaire was mailed to her. If the mother did not respond to the questionnaires, attempts were made to conduct an interview over the telephone. Each mother's questionnaire was linked to her child's birth certificate, and the final data set included information from both the questionnaire and the birth certificate. The data were weighted to adjust for survey design, noncoverage, and nonresponse. PRAMS was approved by the CDC Institutional Review Board.
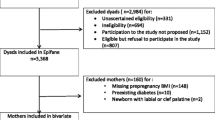
The analysis was limited to nulliparous women with singleton, term (gestation ≥37 weeks) births. A total of 26,682 women were eligible for the study. Women with missing information on the independent variable, prepregnancy BMI (n = 1874, 7.0%), and/or the dependent variable, cesarean delivery (n = 403, 1.5%), were excluded from the analysis (total exclusions (some had missing information on both) n = 2259, 8.4%). The final sample included 24,423 women.
The data source of the variables was either the birth certificate or the PRAMS questionnaire. Cesarean delivery was reported on the birth certificate. No information was available on whether the cesarean delivery was elective or an emergency. Information used to calculate prepregnancy BMI (maternal weight in kilograms/height in m2) was self-reported by the mother on the PRAMS questionnaire. We used the Institute of Medicine definitions of lean (BMI < 19.8), normal (BMI 19.8–26.0), overweight (BMI 26.1–29.0), and obese (BMI > 29) (15). We created a category for very obese (BMI ≥ 35).
Several confounders were considered based on a review of the literature: age, education, race, marital status, Medicaid recipient, maternal height, weight gain during pregnancy, infant birth weight, gestational age, diabetes (preexisting or gestational), hypertension during pregnancy, and complications of labor and/or delivery (3–9). Age, education, race, marital status, complications of labor and/or delivery, weight gain during pregnancy, infant birth weight and gestational age were taken from the birth certificate. Medicaid recipient was reported by the woman on the PRAMS questionnaire. Complications of labor and/or delivery is a composite variable taken from a check box on the birth certificate, “No complications of labor and/or delivery.” If it is checked, it indicates that a woman did not experience any of the following complications: fever, meconium (moderate or heavy), premature rupture of membranes, abruptio placenta, placenta previa, other excessive bleeding, seizures during labor, precipitous labor, breech/malpresentation, cord prolapse, anesthetic complication, fetal distress, dysfunctional labor, prolonged labor (more than 20 h) and cephalopelvic disproportion. Two variables, diabetes and hypertension, were available on the PRAMS questionnaire and the birth certificate. A positive response on the birth certificate or the PRAMS questionnaire was coded as a positive response for diabetes or hypertension, respectively.
We examined the frequency of cesarean delivery among women in five prepregnancy BMI groups: lean, normal, overweight, obese, and very obese. Software for SUrvey DAta ANalysis (SUDAAN) was used to calculate the standard errors so that they reflected selection and response probabilities for the survey design (16). We assessed interactions between prepregnancy BMI and several variables including maternal age, maternal height, gestational weight gain, infant birth weight ≥4000 g, state of residence, maternal race, complications of labor and/or delivery, hypertension and diabetes. Interaction terms were entered into the multivariable model one at a time and were considered statistically significant at p < .01. Then, adjusting for potential confounders, we constructed a multivariable logistic regression model to estimate the association between prepregnancy BMI and delivery by cesarean section. The final model was evaluated for goodness of fit using the Hosmer–Lemeshow Goodness-of-Fit Test (17). Because the outcome variable was not rare, the adjusted odds ratios would have overestimated the magnitude of the association between prepregnancy BMI and cesarean delivery. Therefore, we used the method developed by Zhang and Yu to calculate an estimated adjusted relative risk (18), and the Bootstrap method with 1000 loops to calculate 95% confidence intervals for the adjusted relative risks (SAS version 8.2) (19).
A comparison of demographic variables between women with and without missing information on prepregnancy BMI and/or cesarean delivery found that women with missing information were more likely to be younger, black, a Medicaid recipient, not married, of short stature, and to have experienced a labor and/or delivery complication. No differences were found in diabetes, hypertension, or infant birth weight.
RESULTS
Overall, 22.0% of nulliparous women giving birth to a single, term infant had a cesarean section (Table I). Almost one quarter of the women in the sample were either overweight (10.3%), obese (8.7%), or very obese (5.5%). The majority of women were 20 years of age or older, had at least 12 years of education, were married, and were white. Almost 40% were Medicaid recipients.
The frequency of cesarean delivery increased with increased prepregnancy BMI, from 14.3% (0.8 SE) among lean women to 42.6% (2.0 SE) among very obese women (Table II). This increasing cesarean delivery rate by increasing prepregnancy BMI was consistent within each stratum of demographic, obstetrical, and infant variables.
Demographic variables associated with higher rates of cesarean delivery in the univariate analysis included older age compared to younger age, higher education completed compared to lower, and not being a Medicaid recipient compared to being one. Obstetrical and infant variables associated with higher rates of cesarean delivery included maternal height <62 inches, complications of labor and/or delivery, infant birth weight <2500 g or ≥4000 g, gestational age >40 weeks, diabetes (preexisting or gestational), and hypertension during pregnancy.
We found no significant interactions with prepregnancy BMI and maternal age, maternal height, infant birth weight ≥4000 g, maternal weight gain or state of residence. The association between prepregnancy BMI and cesarean delivery was modified by the “other race” category (p < .03), but not by black or white race. Because other race comprises less than 5% of the sample and represents a heterogeneous group, this interaction was ignored for the analyses and race was considered a potential confounder. Complications of labor and/or delivery significantly interacted with prepregnancy BMI and cesarean delivery (p < .001). This variable is a composite of various factors that may be on the causal pathway between obesity and cesarean delivery. Because diabetes and hypertension also may be on the causal pathway, we added women with either of these risk factors to the group with labor and/or delivery complications and tested for an interaction with prepregnancy BMI and cesarean delivery. It was statisticallysignificant at p < .001. The Hosmer–Lemeshow Goodness-of-Fit Test for the model with the interaction suggested the model fit the data, Chi-square 11.6, p < .16. We, therefore, present all subsequent analyses stratified by these two groups of women: those with complications and those without any complications.
The unadjusted relative risk for cesarean delivery was greatest for very obese women without any complications compared to normal weight women without complications (RR 3.5, 95% 2.7–4.5) (Table III). Very obese women with complications had 1.4 times the risk of cesarean delivery (95% CI 1.3–1.6) compared to normal weight women with complications. After adjusting for covariates, the association between prepregnancy BMI and cesarean delivery remained for women with and without complications, but, again, the risk was greatest among very obese women without complications compared to normal weight women without complications (adjusted estimated RR 3.1, 95% CI 2.3–4.8) (Table IV). For both groups of women, education, marital status, and Medicaid benefits were not associated with cesarean delivery when adjusting for all other variables in the model and thus were not retained in either final model.
DISCUSSION
Our results confirm previous studies' findings that nulliparous women giving birth to single, term infants who are overweight or obese are at increased risk of cesarean delivery (3–7). However, we found this increased risk was not consistent among women with and without complications. Among women with complications, the risk of cesarean delivery increased slightly as prepregnancy BMI increased. Among women without complications, the risk greatly increased among very obese women. This finding suggests that, when other risk factors for cesarean section exist, increasing prepregnancy BMI contributes a slight additional risk compared to that for normal weight women. Without other risk factors, being very obese contributes greatly to the risk compared to that of normal weight women. The magnitude of this increased risk among very obese women without complications may be caused by the increased volume of soft tissue. Subtle labor complications unaccounted for in our data may also explain the difference. For example, obese women labor longer during the active phase and have a decreased cervical dilation rate, which may influence physicians' decisions regarding cesarean delivery (13, 14). Unfortunately, we did not have information on the number of cesarean sections that occurred after the onset of labor. While other studies have controlled for complications (3, 5–7, 9), the findings of our study suggest that women with and without complications should be analyzed separately. In addition, our findings suggest that obesity not only increases the risk of certain complications during pregnancy that lead to increased risk of cesarean delivery, but it also independently increases the risk, especially among very obese women.
A strength of this study is that we had a sufficient sample size to explore potential interactions and to create a prepregnancy BMI group for very obese women. In addition, the measure of association we used, an estimated relative risk instead of an odds ratio, improves upon previous studies that may have overestimated the association between obesity and cesarean delivery. Finally, the 19 states represented in this PRAMS sample accounted for 37% of all US births in 2000 (20).
The study, however, is limited by self-reported prepregnancy weight which may be inaccurate. One study found that underweight women tended to overestimate their prepregnancy weight (21), and another study found that overweight women tended to underestimate their prepregnancy weight (22). If these reporting biases occurred in the PRAMS data, the associations between obesity and cesarean section would be underestimated. Using data from birth certificates is another limitation of this study and having a composite variable for all complications of labor and/or delivery limited our ability to assess complications individually. Birth certificates have been found to reliably report cesarean delivery and celphalopelvic disproportion (23, 24); however, reporting of labor and delivery complications is less complete (23). Because we stratified on this variable, the effect of underreporting complications would result in an underestimated risk of cesarean delivery among overweight or obese women without any complications. Two additional considerations relate to the sample. The PRAMS response rate was 75%. The data were weighted for nonresponse, which assumes that responders and nonresponders of similar demographic characteristics report the same information. We have no reason to believe that this assumption is invalid for prepregnancy BMI. In addition, of women who did respond to PRAMS, 8.4% were missing information on prepregnancy BMI or cesarean delivery. Less than 10% of the sample was excluded for missing data, therefore, the results of this study are unlikely to be affected by these exclusions.
In this study, obese women were more likely to have a cesarean delivery. Why this increase is much greater among very obese women without complications needs further study. Because obese women are much more likely to experience infections and other complications from cesarean delivery than nonobese women, prevention of cesarean delivery is especially needed for this group. Given that the antecedents of obesity begin in childhood, prevention efforts need to begin then and continue through the reproductive years.
REFERENCES
Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Munson ML. Births: Final Data for 2002. National Vital Statistics Reports. Hyattsville, MD: National Center for Health Statistics, 2003, Vol. 52, No. 10.
Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999–2000. JAMA 2002;288:1723–1727.
Kaiser PS, Kirby RS. Obesity as a risk factor for cesarean in a low-risk population. Obstet Gynecol 2001;97:39–43.
Young TK, Woodmansee B. Factors that are associated with cesarean delivery in a large private practice: The importance of prepregnancy body mass index and weight gain. Am J Obstet Gynecol 2002;187:312–320.
Jensen DM, Damm P, Sorensen B, Molsted-Pedersen L, Westergaard JG, Ovesen P, et al. Pregnancy outcome and prepregnancy body mass index in 2459 glucose-tolerant Danish women. Am J Obstet Gynecol 2003;189:239–244.
Witter FR, Caufield LE, Stoltzfus RJ. Influence of maternal anthropometric status and birth weight on the risk of cesarean delivery. Obstet Gynecol 1995;85:947–951.
Brost BC, Goldenberg RL, Mercer BM, Iams JD, Meis PJ, Moawad AH, et al. The Preterm Prediction Study: Association of cesarean section with increases in maternal weight and body mass index. Am J Obstet Gynecol 1997;177:333–341.
Cnattingius R, Cnattinggius S, Notzon FC. Obstacles to reducing cesarean rates in a low-cesarean setting: The effect of maternal age, height, and weight. Obstet Gynecol 1998;92:501–506.
Crane SS, Wojtowycz MA, Dye TD, Aubry RH, Artal R. Association between prepregnancy obesity and the risk of cesarean delivery. Obstet Gynecol 1997;89:213–216.
Cedergren MI. Maternal morbid obesity and the risk of adverse pregnancy outcome. Obstet Gynecol 2004;103:219–224.
Perlow JH, Morgan MA. Massive maternal obesity and perioperative cesarean morbidity. Am J Obstet Gynecol 1994;170:560–565.
Bianco AT, Smilen SW, Davis Y, Lopez A, Lapinski R, Lockwood CJ. Pregnancy outcome and weight gain recommendations for the morbidly obese woman. Obstet Gynecol 1998;91:97–102.
Nuthalapaty FS, Rouse DJ, Owen J. The association of maternal weight with cesarean risk, labor duration, and cervical dilation rate during labor induction. Obstet Gynecol 2004;103:452–456.
Buhimschi CS, Buhimschi I, Malinow AM, Weiner CP. Intrauterine pressure during the second stage of labor in obese women. Obstet Gynecol 2004;103:225–230.
Institute of Medicine. Nutrition during pregnancy. Part I, Weight Gain. Washington, DC: National Academy Press, 1990.
SUDAAN, Release 8.0 [Computer Software], Research, Triangle Park (NC): Research Triangle Institute, 1991.
Hosmer DW, Lemeshow S. Applied Logistic Regression, New York, NY: Wiley, 1989.
Zhang J, Yu KF. What's the relative risk? A method for correcting the odds ratio in cohort studies of common outcomes. JAMA 1998;280:1690–1691.
Efron B, Tibshirani R. An Introduction to the Bootstrap. New York, NY: Chapman & Hall, 1993.
Martin JA, Hamilton BE, Ventura SJ, Menacker F, Park M. Births: Final Data for 2000. National Vital Statistics Reports. Hyattsville, MD: National Center for Health Statistics, 2002, Vol. 50, No. 5.
Lederman SA, Paxton A. Maternal reporting of prepregnancy weight and birth outcome: Consistency and completeness compared with the clinical record. Matern Child Health J 1998;2(2):123–126.
Stevens-Simon C, Roghmann KJ, McAnarney ER. Relationship of self-reported prepregnant weight and weight gain during pregnancy to maternal body habitus and age. J Am Diet Assoc 1992;92:85–87.
DiGiuseppe DL, Aron DC, Random L, Harper DL, Rosenthal GE. Reliability of birth certificate data: A multi-hospital comparison to medical records information. Matern Child Health J 2002;6(3):169–179.
Dobie SA, Baldwin L, Rosenblatt RA, Fordyce MA, Andrilla CH, Hart LG. How well do birth certificates describe the pregnancies they report? The Washington State experience with low-risk pregnancies. Matern Child Health J 1998;2:145–154.
ACKNOWLEDGMENTS
Data from the Pregnancy Risk Assessment Monitoring System (PRAMS) included in this study are collected at the state level by the following state collaborators and their staff: Alabama-Rhonda Stephens, MPH; Alaska-Kathy Perham-Hester, MS, MPH; Arkansas-Gina Redford, MAP; Colorado-Alyson Shupe, PhD; Florida-Helen Marshall; Hawaii-Limin Song, MPH, CHES; Illinois-Theresa Sandidge, MA; Louisiana-Dionka Pierce; Maine-Martha Henson; Nebraska-Jennifer Severe-Oforah, PhD; New Mexico-Ssu Weng, MD, MPH; New York State-Anne Radigan-Garcia; North Carolina-Paul Buescher, PhD; Ohio-Amy Davis; Oklahoma-Dick Lorenz, MS; South Carolina-Mary Kate Powell; Utah-Lois Bloebaum; Washington-Linda Lohdefinck; West Virginia-Melissa Baker, MA; CDC PRAMS Team, Applied Sciences Branch, Division of Reproductive Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dietz, P.M., Callaghan, W.M., Morrow, B. et al. Population-Based Assessment of the Risk of Primary Cesarean Delivery Due to Excess Prepregnancy Weight Among Nulliparous Women Delivering Term Infants. Matern Child Health J 9, 237–244 (2005). https://doi.org/10.1007/s10995-005-0003-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-005-0003-9