
Abstract
The aims of the study were to compare the change in the Wisconsin Stone Quality of Life (WISQOL) score in patients who underwent retrograde intrarenal surgery (RIRS) single-use ureteroscope or extracorporeal shock wave lithotripsy (ESWL) with a calculation of quality-adjusted life-years (QALYs). 158 patients treated with urinary stone disease were randomly divided into 80 patients in the validation and 78 patients in the intervention arm. Patients in the intervention arm were randomly divided into the RIRS or the ESWL group. Linguistic validation of the WISQOL into the Slovak language was performed using a standardised multistep process. Discriminant validity was assessed by comparing stone-forming patients to an additional 34 healthy individuals. Patients were asked to fill in the WISQOL before and in the 24th week after the intervention. The QALYs were calculated by the formula QALY = weight factor (WF) x time period after intervention. The Cronbach’s α of the WISQOL was 0.94, the Pearson’s coefficient for test–retest reliability was 0.91, and the discriminant validity confirmed a higher score for healthy individuals (p < 0.001). The median WISQOL score changed from 45.5 to 95.5 vs. 33.9 to 87.1 in the RIRS and ESWL groups, respectively (p < 0.001). Patients from the RIRS group had a good possibility of reaching 19.727 QALYs gained during life expectancy compared to 15.780 for the ESWL group (p < 0.001). RIRS single-use ureteroscope is significantly superior to ESWL in reaching more QALYs gained during life expectancy. The WISQOL Slovak version is valid, reliable and strictly specific for stone-forming patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Urolithiasis has major impact on patient health-related quality of life (HRQOL). Understanding this, there is a need for a disease-specific HRQOL testing tool in stone-forming patients [1]. Penniston et al. developed the Wisconsin Stone-Quality of Life Questionnaire (WISQOL) in 2017 [2]. The WISQOL consists of four domains including social impact, emotional impact, disease-specific symptoms and vitality and has been translated and validated in a number of countries worldwide [3, 4]. It proved to be a useful instrument to test HRQOL in stone patients in daily clinical practice. The quality-adjusted life-years (QALYs) consider the quantitative and qualitative aspects of life that are affected by health interventions. QALY is a mathematical result of life expectancy rates and the quality of remaining years of life. Time is a very important factor in determining QALYs. One year spent in perfect health equals 1 and a year spent in worse health counts less than 1 QALY. It all depends on the value of current quality of life. Death is considered equivalent to 0, however, some health conditions are considered worse than death and have negative scores [5].
Among active intervention options in stone patients, extracorporeal shockwave lithotripsy (ESWL) and retrograde intrarenal surgery (RIRS) are the most common. Both methods are recommended for proximal stones up to 20 mm as the first-choice treatment with a good long-term stone-free rate (SFR) [6, 7]. However, there is lack of studies assessing the impact of ESWL and RIRS on the HRQOL of patients using a disease-specific questionnaire.
The aim of this study was to compare the change in WISQOL score in patients who underwent RIRS or ESWL 24 weeks after the intervention with a calculation of quality-adjusted life-years (QALYs).
Materials and methods
In total, 158 patients treated with stone disease at our department from January 2018 to June 2019 agreed to take part in this study. Inclusion criteria were a stone burden less than 20 mm of less than 1000 HU according to a native CT scan, unilateral stones localised in the pyeloureteral junction, renal pelvis, patients without previous intervention and an after-intervention follow-up of at least 24 weeks. Exclusion criteria were benign prostatic hyperplasia (BPH), active inflammation of the urinary tract, chronic inflammation of the lower urinary tract, pelvic pain syndrome, urinary incontinence, overactive bladder syndrome, lower urinary tract dysfunction, neurological and psychiatric diseases, pregnancy for female patients, genitourinary malignancies and major chronic diseases. Patients were randomly divided into two arms: 80 patients were enrolled in the validation part of the study and 78 patients were enrolled in the intervention part of the study (Fig. 1). Based on a test strength of 0.80 and an alpha of 0.05 (type I error), a sample of 31 patients in the RIRS group and 31 patients in the ESWL group was required. We expected a dropout rate of 20%, so we included a total of 78 patients. According to the sample selection, we expected a 50% increase in QALYs after the intervention.

Enrolment diagram
Questionnaire validation and psychometric testing
Linguistic validation of the WISQOL in the Slovak language was performed using a standardised multistep process [8]. The tool was translated from the original English language to Slovak by two independent native Slovak-speaking professional English translators. A consensus meeting was held with the translators and urologists. The first draft of the Slovak WISQOL was created. After a pilot study on five patients, a back-translation was performed. Two independent translators with English as their native language and Slovak as their first foreign language performed the back-translation. Thereafter, another consensus meeting with the authors of original WISQOL was held. Finally, the Slovak version of the WISQOL was established for further psychometric testing.
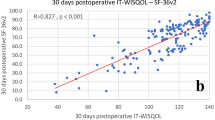
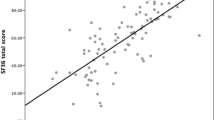
In the next step, patients in the validation arm self-administered the questionnaire. They were asked to do it again in 2 weeks with no intervention during this time period. Domain scores of the questionnaire were calculated according to the original scoring guide. The WISQOL consists of 28 items which are divided into four domains (Domain 1: Social impact; Domain 2: Emotional impact; Domain 3: Stone-related symptom impact; Domain 4: Impact on vitality). A five-point Likert scale was used to assess responses. The maximum score for the instrument is 140 (28 × 5), a higher score correlates to a higher health-related quality of life. A linear transformation was performed to calculate the responses ranging from 0 (the lowest quality of life) to 100 (the highest quality of life) according to the formula adjusted to each domain or total score. The internal consistency of WISQOL was tested using Cronbach’s α coefficient. Test–retest reliability was calculated using Pearson’s coefficient. Discriminant validity was assessed by comparing stone-forming patients to an additional 34 healthy individuals who had no history of urinary stone disease or any major chronic diseases and reported no related symptoms.
Intervention and QALYs calculation
A randomized controlled trial with a 1:1 allocation compared the effect of RIRS and ESWL treatment. The computer generated odd (RIRS) and even numbers (ESWL) for 78 patients in the intervention part of the study. The patients were randomised to the RIRS group (39 patients) or the ESWL group (39 patients) by the odd/even rule (Fig. 1). All the stones were located inside the kidney collecting system during each procedure. The number of procedures required to achieve a stone-free rate (SFR) with stone fragments ˂1 mm and complication rates were recorded for each method. Kidney, ureter, bladder (KUB) plain film radiography was performed the next day after each procedure and in 4 weeks. Native CT scan was performed in the 24th week after each procedure. All the ureteroscopies were performed using disposable flexible scopes. All the patients received antibiotic prophylaxis. Patients were followed-up and in the 24th week after the intervention were asked to fill in the WISQOL questionnaire again.
The main outcome measure was QALYs calculated according to the formula QALY = WF × time period after intervention (during 168 days, 1 year, life expectancy). The weight factor (WF) used for QALY calculation was based on WISQOL score reported by patients and calculated by linear transformation of the score achieved, ranging from 0.0 to 1.0. The weight factor (WF) for QALYs calculation was done by formula: WF = linear-transformed of total score/100. The life expectancy of patients was based on national mortality rate statistics [9].
The study was approved by the local ethics committee (EK UNM 47/2020). All patients were fully informed about the purpose of the study and provided signed written informed consent. The Mann–Whitney U test, Wilcoxon signed-rank test and chi-squared test were used to calculate the results. The non-parametric distribution was calculated as the median, 25th and 75th percentiles. The final comparison was made using ETA squared. All the calculations were processed using IBM SPSS Statistics for Macintosh, version 25.0 with statistically significant values indicated by p < 0.05.
Results
Out of the 80 patients enrolled in validation arm of the study, 52 (65%, median age 59.0 years; interquartile range IR 50.3–66.8) successfully filled test and retest part of the questionnaire with interval of 2 weeks. The total Cronbach’s α for the whole questionnaire was 0.94. Cronbach’s α and Pearson’s coefficient for the social impact domain, emotional impact domain, disease-specific symptoms and vitality domain were 0.92, 0.92, 0.82, 0.89 and 0.93, 0.76, 0.83, 0.89, respectively. Pearson’s coefficient for test–retest reliability of the whole questionnaire was 0.91. Discriminant validity was shown as patients with stone disease scored lower on most questions and for the total score than 34 healthy individuals (median age 63.5 years; IR 55.8–71.0) with p < 0.001. The total median score for the stone formers was 91.0 (IR 75.0–101.3) and 134.0 (IR 127.5–138.0) for the healthy individuals.
In the intervention part of the study, 66 out of 78 patients (84.6%) successfully fulfilled the conditions (follow-up of at least 24 weeks after the intervention with completion of the questionnaire in the 24th week, Table 1). Intrarenal stent was inserted before the intervention in 46.9% of patients in the ESWL group and 73.5% of patients for the RIRS group with statistical significance at p < 0.05.
For the ESWL group to achieve the given SFR, 59.4% patients required one procedure, 31.3% patients required two procedures and 9.4% patients required three or more procedures. For the RIRS group, 20.6% patients required two procedures and the rest of the patients (79.4%) needed only one procedure to achieve the given SFR. There was no statistically significant difference in the retreatment rate between the groups. Fifty percent of the patients in the ESWL group and 67.6% patients in the RIRS group were left with a stent at least 1 week after the intervention without a significant difference between the groups. Only one patient was stented after the ESWL in addition to 15 patients who were pre-stented. All the stents were removed 1 week after each procedure and thus this did not affect the resulting changes in quality of life in the group of patients after 24 weeks. In the ESWL group, one patient developed a renal hematoma and one patient suffered from post-intervention kidney inflammation. There were no recorded complications in the RIRS group.
After the intervention, the total WISQOL score median was 95.5 for the RIRS group and 87.1 for the ESWL group with a statistically significant difference. The WISQOL revealed statistically significant differences with patients benefitting RIRS over ESWL in all domains (Tables 2, 3). The after-intervention median QALYs for the period of 1 year were 0.955 for the RIRS group and 0.871 for the EWSL group with a statistically significant difference. Before the treatment, QALYs for the patients in the RIRS group were 10.216 (men vs women; 9.750 vs 11.825) and for the patients in the ESWL group were 7.595 (men vs women; 6.943 vs 7.796) without a statistically significant difference. After the treatment, patients from the RIRS group had a good possibility of reaching 19.727 QALYs (men vs women; 16.893 vs 25.317) during life expectancy compared to 15.780 (men vs women; 16.607 vs 14.139) for the ESWL group with a statistically significant difference (Table 3). Patients in the RIRS group received greater increases in QALYs than in the ESWL group (9.511 versus 8.185 QALYs).
Discussion
Stone disease is one of the most common urological diseases with an increasing rate of incidence [10, 11]. Interestingly, HRQOL in stone-forming patients is evaluated mostly using general questionnaires [12]. However, patients suffering from urolithiasis have several specific problems with a direct impact on their quality of life. The need for a disease-specific instrument was fulfilled by Penniston et al. with the development of the WISQOL. The 28-item four-domain questionnaire assesses all of the main hardships experienced by patients with stones. In our study, we chose to validate the WISQOL and use it for further testing.
HRQOL testing is still a novelty for many patients and clinicians. In the validation part of the study, patients were requested to fill in two copies of the WISQOL within a 2-week period. Many patients were willing to complete just one copy, which was the main reason for the high drop-out rate in this part of the study. Despite this, the results showed excellent internal consistency and reliability of the Slovak version of the WISQOL. With knowledge of the original WISQOL validation process [2], we also decided to assess the discriminant validity of the questionnaire using the WISQOL score of 34 healthy individuals examined at our department for preventive care. The results showed the excellent discriminant validity of the questionnaire.
In recent years, improvement in laser techniques and the introduction of single-use disposable flexible ureteroscopes have made RIRS the preferred option for both clinicians and patients. Several studies have compared RIRS with ESWL in adults suffering from stone disease [13,14,15]. However, most recent data show the same long-term results for the two methods and a lower price for ESWL [6]. To our knowledge, there has been no previous study comparing the HRQOL outcomes of these two methods using a stone disease-specific HRQOL-testing tool.
We decided to compare these two methods in the intervention part of the study using the WISQOL questionnaire. We randomised our patients to each intervention and asked them to fill in the WISQOL in before the intervention and 24 weeks after the intervention. After each intervention, we evaluated basic outcomes firstly and WISQOL with QALYs secondly.
Interestingly, the retreatment rates of the RIRS and ESWL groups required to achieve SFR did not show statistical significance in our study. This may be a result of a good indication and a novel lithotripter. Out of all patients, only two in the ESWL group suffered from minor to moderately severe complications. Following the usual routine at our department, the pre-stenting rate was high. Pre-stenting before ESWL (50% of patients) was high with the knowledge that stenting does not benefit stone-free rate and can induce lower urinary tract symptoms [16]. However, the final effect of the procedure overall was good, as stated above. The RIRS group compared to the ESWL had statistically significantly more frequent stent placement before the intervention. We see a future challenge in improving the indication for stent placement.
The next step was the WISQOL score comparison and QALY calculation. The better results for the RIRS group came as a surprise. The RIRS group was superior in the most calculations over ESWL. Trying to understand these results, we analysed the domains of the WISQOL questionnaire. Complete restoration of quality of life occurred mainly in the RIRS group in social, stone-related symptom and vitality impact after 24 weeks of follow-up. The emotional impact has not completely improved, which may indicate partial concern for recurrence of the disease in the future. The emotional and stone-related symptom impact have not completely improved in the ESWL group. This indicates greater concerns about the future diseases and repeated surgical interventions. However, all the ESWL procedures were performed using a modern lithotripter and patients were well-informed of this fact. Regardless, health insurance companies offer patients full reimbursement for both methods in Slovakia.
The strength of this study is the usage of the WISQOL as a well-validated disease-specific HRQOL assessing instrument. Proper randomisation of patients with no significant difference between the RIRS and ESWL groups before the intervention is the second strength. The third strength of our study is the calculation of QALYs we performed.
The limitations of the study are the loss of patients and low adherence of patients to questionnaire administration. The high pre-stenting rate in the RIRS and ESWL groups is the third limitation of our study.
Conclusion
According to the stone-disease-specific WISQOL questionnaire, RIRS single-use ureteroscope is significantly superior to ESWL with more QALYs during life expectancy. The Slovak version of WISQOL is valid, reliable and strictly specific for stone-forming patients. Several large studies testing HRQOL in stone patients are currently in progress worldwide. Hopefully, these results will bring more insight into the comparison of HRQOL of patients after RIRS and ESWL.
Change history
06 February 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00240-020-01235-1
References
New F, Somani BK (2016) A complete world literature review of quality of life (QOL) in patients with kidney stone disease (KSD). Curr Urol Rep 17(12):88
Penniston KL, Antonelli JA, Viprakasit DP, Averch TD, Sivalingam S, Sur RL, Pais VM Jr, Chew BH, Bird VG, Nakada SY (2017) Validation and reliability of the Wisconsin stone quality of life questionnaire. J Urol 197(5):1280–1288
Atalay HA, Ulker V, Canat L, Murat O, Can O, Penniston KL (2018) Validation of the Turkish version of the Wisconsin stone-quality of life questionnaire. Turk J Urol 45(2):118–123
Basulto-Martínez M, Olvera-Posada D, Velueta-Martínez IA, Méndez-Probst C, Flores-Tapia JP, Penniston K, Guerrero-Putz MD, Heinze A (2020) Quality of life in patients with kidney stones: translation and validation of the Spanish Wisconsin Stone Quality of Life Questionnaire. Urolithiasis 48(5):419–424
Marseille E, Larson B, Kazi DS, Kahn JG, Rosen S (2015) Thresholds for the cost-effectiveness of interventions: alternative approaches. Bull World Health Organ 93(2):118–124
Alken P (2018) Intracorporeal lithotripsy. Urolithiasis 46(1):19–29
Geraghty RM, Jones P, Herrmann TRW, Aboumarzouk O, Somani BK (2018) Ureteroscopy is more cost effective than shock wave lithotripsy for stone treatment: systematic review and meta-analysis. World J Urol 36(11):1783–1793
Hutchinson A, Bentzen N, König-Zahn C (1996) Cross-cultural health outcome assessment: a user’s guide. European Research Group on Health Outcomes, Ruinen
Statistical Office of the Slovak Republic (2020) Statistiky—Demografia a socialne statistiky—Obyvatelstvo a migracia—Ukazovatele—Tabulky zivota—Zdrave roky zivota podla EU SILC, 2005–2018 (in Slovak language). http://datacube.statistics.sk/#!/view/sk/VBD_SLOVSTAT/om2021rs/v_om2021rs_00_00_00_sk Accessed 14 Mar 2020
Hesse A, Brändle E, Wilbert D, Köhrmann KU, Alken P (2003) Study on the prevalence and incidence of urolithiasis in Germany comparing the years 1979 vs. 2000. Eur Urol 44(6):709–713
Stamatelou KK, Francis ME, Jones CA, Nyberg LM, Curhan GC (2003) Time trends in reported prevalence of kidney stones in the United States: 1976–1994. Kidney Int 63(5):1817–1823
Angell J, Bryant M, Tu H, Goodman M, Pattaras J, Ogan K (2012) Association of depression and urolithiasis. Urology 79(3):518–525
El-Nahas AR, Ibrahim HM, Youssef RF, Sheir KZ (2012) Flexible ureterorenoscopy versus extracorporeal shock wave lithotripsy for treatment of lower pole stones of 10–20 mm. BJU Int 110(6):898–902
Fankhauser ChD, Hermanns T, Lieger L, Diethelm O, Umbehr M, Luginbuhl T, Sulser T, Muntener M, Poyet C (2018) Extracorporeal shock wave lithotripsy versus flexible ureterorenoscopy in the treatment of untreated renal calculi. Clin Kidney J 11(3):364–369
Desai M, Sun Y, Buchholz N, Fuller A, Matsuda T, Matlaga B, Miller N, Bolton D, Alomar M, Ganpule A (2017) Treatment selection for urolithiasis: percutaneous nephrolithotomy, ureteroscopy, shock wave lithotripsy, and active monitoring. World J Urol 35(9):1395–1399
Shen P, Jiang M, Yang J, Li X, Li Y, Wei W, Dai Y, Zeng H, Wang J (2011) Use of ureteral stent in extracorporeal shock wave lithotripsy for upper urinary calculi: a systematic review and meta-analysis. J Urol 186(4):1328–1335
Author information
Authors and Affiliations
Contributions
JS: ideas; project development; responsible for validation of the questionnaire and progression of the study; data collection; data analysis; manuscript writing and approving the final version; IS: data collection; progression of the study; supervision; manuscript editing and approving the final version; VSv: responsible for validation of the questionnaire; data analysis; manuscript editing and approving the final version; VSt: responsible for progression of the study; manuscript editing and approving the final version; JL: responsible for progression of the study; supervision; manuscript editing and approving the final version. All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by JS, IS, VS, VS and JL. The first draft of the manuscript was written by JS and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical approval
The study was approved by the ethics committee of University Hospital Martin under the protocol number EK UNM 47/2020. Informed consent was obtained from all individual participants included in the study. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: Given name and family name were changed.
Rights and permissions
About this article

Cite this article
Svihra, J., Sopilko, I., Svihrova, V. et al. Is health-related quality of life of patients after single-use flexible ureteroscopy superior to extracorporeal shock wave lithotripsy? A randomised prospective study. Urolithiasis 49, 73–79 (2021). https://doi.org/10.1007/s00240-020-01224-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-020-01224-4