
Abstract
Purpose
Systematically search and analyse the results of surgical and non-surgical treatments for insertional Achilles tendinopathy.
Methods
A structured systematic review of the literature was performed to identify surgical and non-surgical therapeutic studies reporting on ten or more adults with insertional Achilles tendinopathy. MEDLINE, CINAHL, EMBASE (Classic) and the Cochrane database of controlled trials (1945–March 2011) were searched. The Coleman methodology score was used to assess the quality of included articles, and these were analysed with an emphasis on change in pain score, patient satisfaction and complication rate.
Results
Of 451 reviewed abstracts, 14 trials met our inclusion criteria evaluating 452 procedures in 433 patients. Five surgical techniques were evaluated; all had a good patient satisfaction (avg. 89 %). The complication ratio differed substantially between techniques. Two studies analysed injections showing significant decrease in visual analogue scale (VAS). Eccentric exercises showed a significant decrease in VAS, but a large group of patients was unsatisfied. Extracorporeal shockwave therapy (ESWT) was superior to both wait-and-see and an eccentric training regime. One study evaluated laser CO2, TECAR and cryoultrasound, all with significant decrease in VAS.
Conclusions
Despite differences in outcome and complication ratio, the patient satisfaction is high in all surgical studies. It is not possible to draw conclusions regarding the best surgical treatment for insertional Achilles tendinopathy. ESWT seems effective in patients with non-calcified insertional Achilles tendinopathy. Although both eccentric exercises resulted in a decrease in VAS score, full range of motion eccentric exercises shows a low patient satisfaction compared to floor level exercises and other conservative treatment modalities.
Level of evidence
III.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Much has been published on the treatment for (midportion/non-insertional) Achilles tendinopathy and retrocalcaneal bursitis [11, 16, 23, 27, 29, 38, 39, 43, 46]. There is a tendency to prescribe known effective treatment for (midportion/non-insertional) Achilles tendinopathy or retrocalcaneal bursitis to patients with insertional Achilles tendinopathy [3, 17, 22, 28, 34, 36, 52]. Insertional Achilles tendinopathy however is a distinct clinical entity from midportion/non-insertional Achilles tendinopathy or retrocalcaneal bursitis [8, 21, 35, 45, 50, 52]. Aetiology, injury mechanism, treatment and rehabilitation differ between these pathologies [34, 48]. The ‘extrapolation’ is in part due to the confusing terminology of Achilles tendon pathology [7, 13, 25]. Different pathologies have been compared under the name of insertion tendinosis/pathy of the Achilles tendon [2, 17, 40]. Moreover, the confusing terminology aids in the current complicated overview of data for the treatment for insertional Achilles tendinopathy [2, 30, 34, 38, 41]. A recent terminology on Achilles tendon pathologies was proposed to simplify the current terminology and hereby aid the clinical practice, both in diagnostics and treatment [50]. The current treatment for insertional Achilles tendinopathy varies substantially; several surgical and non-surgical treatments have been described, but there is no consensus on the most effective management [5, 6, 10, 24, 42]. One previous study concluded there is a consensus that non-surgical intervention is preferred prior to surgical intervention for insertional Achilles tendinopathy [24]. However, it has not been studied which treatment is the most effective non-surgical intervention or which is the most effective surgical intervention. The purpose of this systematic review is to analyse the effectiveness of different available surgical and/or non-surgical treatment modalities for insertional Achilles tendinopathy.
Materials and methods
The definition of insertional Achilles tendinopathy, retrocalcaneal bursitis and midportion Achilles tendinopathy for this systematic review was based on the recently proposed terminology on AT pathology [50] (Table 1).
Primary outcome measures
-
Change of numeric pain score [e.g. visual analogue scale (VAS)]
-
Patient satisfaction
Secondary outcome measures
-
Complication rate
-
Coleman methodology score
-
Intervention
-
Diagnostic method
-
Other outcome data
Inclusion criteria
Studies reporting on the outcome of treatment for insertional Achilles tendinopathy were eligible for this systematic review. A pain scale, overall patient satisfaction or American orthopaedic foot and ankle (AOFAS)-Hindfoot scale score had to be reported. Review and expert opinion papers were excluded. There were no language barriers.
Exclusion criteria
Studies on the treatment for Achilles midportion tendinopathy or unspecified Achilles tendinopathies were excluded. Studies combining the results of insertional and non-insertional Achilles tendinopathy were also excluded if the results of insertional Achilles tendinopathy could not be analysed separately. All studies on pathology located at or around the Achilles tendon insertion but not diagnosed as insertional Achilles tendinopathy (e.g. retrocalcaneal bursitis) were excluded. Studies were excluded if scaled data of pain (e.g. VAS) or patient satisfaction was not provided. Studies reporting on <10 patients were excluded.
Study population
Adults (>18 years) with diagnosed insertional Achilles tendinopathy were eligible. Adults with non-insertional or non-specified problems of the Achilles tendon insertion were excluded.
Search strategy
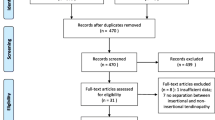
An extensive MEDLINE, EMBASE (Classic) and CINAHL search (1945–March 2011) was performed using the following terms: (((((insertion OR insertional OR enthesis OR attachment) AND (enthesitis OR enthesopathy OR tendinopathy OR tendinosis OR tendinoses OR tendinitis OR tendinitides OR tendinopathies OR tendonitis OR tendonitides OR tenosynovitis) AND achilles)) OR ((tendon OR tendons OR tendo) AND (enthesis OR attachment OR insertion OR insertional) AND achilles AND (spur OR spurs OR calcification OR calcif*)))) In addition, the Cochrane Database of Clinical and Randomized Controlled Trials were searched using the search term ‘Achilles’. After combining the results and removing duplicates of these searches, a total of 451 papers were retrieved. Based on title, abstract and study design, 393 articles were excluded. Exclusion was based on study design (105 articles), papers unrelated to the Achilles tendon (172), related to the Achilles tendon but unrelated to insertional Achilles tendinopathy (33 articles related to midportion tendinopathy, 83 articles related to Achilles tendon rupture) (Fig. 1). The full text of the remaining 58 articles was obtained. A review of references of full text articles obtained 15 new articles. A total of 73 full text articles were reviewed. 59 articles were excluded based on full text, resulting in the inclusion of 14 articles for this review (Table 3) [10, 12–14, 20, 22, 26, 31, 32, 37, 42, 44, 51, 53].

Search strategy
Data collection and study selection
Two reviewers independently assessed all studies. These two reviewers identified all titles, assessed the abstracts independently and excluded the irrelevant articles. Any remaining difference between reviewers was settled by discussion. Authors of the included studies were contacted by e-mail or phone to retrieve any necessary additional data (Tables 3, 5).
Data extraction
The two reviewers independently extracted data for the aforementioned outcome using a data extraction form. Differences were settled by discussion. Complications were divided in minor and major (Table 2).
Statistical analysis and quality assessment
Data are presented as weighted means and summed percentages. In addition, all included studies were measured according the Coleman methodology score (CMS) for tendinopathies of the Achilles tendon (Appendix 1) [47]. This score was created to assess the quality of studies evaluating the surgical outcome for Achilles tendinopathies [47]. The scale consists of two parts, with a highest possible score of 100. To simplify the quality comparison of surgical and non-surgical studies, the ‘description of surgical procedure given’ was interpreted as ‘description of procedure given’ in non-surgical studies. In addition, as there is no post-operative rehabilitation in non-surgical studies, a maximum score was granted to non-surgical studies for “description of post-operative rehabilitation”. The authors of the score stated that an increase in CMS would show a decrease in effectiveness of the evaluated treatment [47]. It was also described that an increase in CMS had a positive linear correlation with an increase in year of publication [47]. The Spearman correlation coefficient (ρ) is calculated for both hypotheses.
Results
Results are divided in a surgical and a non-surgical group. The non-surgical group is subdivided in four groups.
Population characteristics
The total number of patients with insertional Achilles tendinopathy in the 14 included studies was 433; 452 tendons were treated. Overall, the weighted mean age of 12 studies was 49 years (range 18–83), 51 % male and 49 % female (two studies did not report patient characteristics). The subgroup surgical treatment had a weighted mean age of 54 (range 18–83) years (one study did not report on patient characteristics). The non-surgically treated subgroup consisted of 50 % male and 50 % female with a weighted mean age of 44 (range 21–80) years (one study did not report on patient characteristics).
Surgical treatment
Six studies, covering five operative techniques and a total of 200 patients with 211 tendons (procedures), were evaluated (Tables 3, 4) [12, 20, 31, 33, 51, 53]. The weighted mean age of surgically treated patients was 54 (range 47–57). The male–female ratio was 6:5 (55:45 %). Five studies reported on patient satisfaction, all showed a relative good outcome regarding patient satisfaction with 163 out of 183 patients (89 %) reporting an excellent or good satisfaction (Table 4) [12, 31, 32, 51, 53]. A total of 52 complications (23 %) were documented; including seven major complications (3.1 %) (Table 4). Subjective pain scales and other questionnaires were not regularly used (Tables 3, 5).
Non-surgical treatment
Injections
Two studies evaluated different types of injections [37, 44]. In a retrospective analysis, Ryan et al. [44] included 22 patients treated with ultrasound (US)-guided hyperosmolar dextrose (20 mg/mL) injections. A mean of 5 injections were given. The mean VAS on daily activity decreased with 4.1 points (p = 0.001) (on a 10-point VAS scale) at follow-up (28.6 months). The authors did not report on patient satisfaction. Ohberg et al. [37] prospectively analysed 11 patients, who were treated with polidocanol injections until symptoms dissolved (up to five injections). The mean VAS showed a decrease of 5.9 at 8 months follow-up, and 8 out of 11 (73 %) patients were satisfied with the outcome (Table 5).
Eccentric training
Four studies evaluated the treatment for eccentric exercises [13, 22, 26, 42]. A total of 92 patients with 100 painful tendons were studied. A 12-week daily eccentric treatment regime was used in every study. There were some differences in treatment protocol; three studies evaluated full range eccentric exercises (below the step), whereas the other evaluated floor level eccentric exercises (providing less stress on the Achilles’ insertion); in addition, there where some difference between ‘number of daily sets’ and ‘number of repetitions’. All four studies used a numerical pain scale; three studies documented the patient satisfaction of the received treatment [13, 22, 42]. When combining the results, an overall decline on a 10-point scale was 2.7 points (weighted mean). All studies combined, and the patient satisfaction showed a large group of unsatisfied patients: of 83 patients only 35 (42 %) were either ‘extremely satisfied’ or ‘satisfied’ (Table 5). Subdividing the full range of motion eccentric group from the floor level eccentric exercises, a noticeable difference was found. The VAS for full range of motion decreased with a weighed mean of 2.0 points, whereas in the floor level, group is decreased with 3.9 points. In addition, 18 of 27 (67 %) were satisfied in the floor level group, in the full range of motion only 17 of 56 (30 %) were satisfied (Table 5).
Extracorporeal shockwave therapy
Two studies tested the effect of extracorporeal shockwave therapy (ESWT) for insertional Achilles tendinopathy, one prospective study and one randomized controlled trial [14, 42]. Furia et al. [14] prospectively compared an ESWT group to a matched control group receiving non-specified ‘traditional treatment’. A mean decrease in VAS of four points was measured after 12 months; 29 out of 35 (83 %) patients were satisfied with ESWT. The control group (n = 33) showed a significantly less decrease in VAS and patient satisfaction. Rompe et al. [42] compared ESWT with an eccentric training regime in a RCT, 25 patients received ESWT. The VAS decrease was 5.1 points at final follow-up, 16 (64 %) patients were satisfied with their treatment. Overall, 49 out of 64 (77 %) were satisfied after ESWT (Table 5).
Others
One study evaluated three different non-surgical treatment modalities: Costantino et al. [10] compared laser CO2 with TECAR and cryoultrasound. Five patients were included in each group. Every intervention showed a significant decrease in VAS score at follow-up. All five patients in the cryoultrasound group were very satisfied; in the TECAR group, two were very satisfied and three were satisfied; in the laser CO2 group, all five were satisfied (Table 5).
Methodological quality
All included studies were measured according to the CMS for tendinopathies of the AT [47]. The mean CMS was 58 (range 36–78) (Table 4). The surgical studies scored a mean CMS of 52 (range 36–67), all non-surgical studies scored a mean CMS of 62 (range 44–78). We did not find a significant (p < 0.05) correlation between the CMS and effectiveness of the evaluated treatment (Fig. 2). In addition, the authors of the CMS stated there is a positive linear correlation between the date of publications and the CMS [47]. We found a significant positive linear correlation of 0.71 (p = 0.02) (Fig. 3).

Relationship between CMS and reported success rate (non-significant difference)

Relationship between CMS and year of publication ρ = 0.71 (significant difference, p = 0.02)
Discussion
The most important findings of this study are the outcome differences between ESWT, full range of motion eccentric exercises, floor level eccentric exercises, and furthermore the overall good outcome after surgical treatment in case of persisting complaints. One previous systematic review was performed regarding insertional Achilles tendinopathy, this included 11 articles and outlined the current used treatments; however, no outcome data were provided [24]. Despite the overlap, we believe that this systematic review adds methodological quality and incorporates recently published data to provide the best currently available evidence. Regardless of the strict inclusion criteria, our systematic review reports on 14 articles and specifically emphasizes the patient satisfaction and change in pain scores. Herewith, we aimed to provide an overview of the effectiveness for every available treatment for insertional Achilles tendinopathy. Kearney et al. [24] concluded that non-surgical treatment is preferred prior to surgical treatment. In addition, they concluded that non-surgical treatment favoured eccentric training and ESWT [24]. The results of the current review however showed a large group of unsatisfied patients after eccentric training compared to other non-surgical treatment [12, 13, 22, 42] (Table 4). The reason of this difference in interpretation of almost equal data is unsure. Kearney et al. did not include multiple studies which were included in this review. In addition, their (primary) outcome measures were not clearly stated. The primary outcomes of the current study are patient satisfaction and change in pain scale. Hence, the primary outcomes variance may cause the interpretation differences. As eccentric training has a substantial effect on the decrease of pain, this may be interpreted as effective; Kearney et al. may have based their conclusion hereupon regardless of the patient satisfaction. The included studies used a wide range of outcomes with little consistency between studies (Tables 3, 5). Evaluation and comparison are therefore difficult. As data are presented as weighted means and summed percentages, the results should be interpreted with caution. The most frequent used outcome was a numerical pain scale, often a 11-point scale but also a 7-point or no numerical scale was used. In addition, the AOFAS, VISA-A, Roles & Maudsley score and different patient satisfaction measurement methods were used. The CMS was used to assess the methodological quality of included articles. The CMS was first designed to assess the quality of patella tendinopathy, later it was modified by Tallon et al. to assess the quality of surgical studies on Achilles tendinopathy [9, 47]. Out of a maximum score of 100 point, the mean CMS for included studies was 58 (range 36–78). As stated, the maximum score of ten points was granted for ‘description of post-operative rehabilitation’ to non-surgical studies. This simplified the comparison of relative outcome in quality between surgical and non-surgical studies. It also implicates that the absolute mean overall score of non-surgical studies would be biased by the used treatment as these studies start with a CMS of ten points. All included surgical studies however scored ten points for ‘description of post-operative rehabilitation’.
Surgical treatment
A total of six studies evaluated the outcome of surgical treatment for insertional Achilles tendinopathy [12, 20, 31, 32, 51, 53]. The evaluated studies described five different operative techniques (Table 4). None of the included surgical techniques were minimally invasive. All minimal invasive surgical studies were excluded due to unclear terminology, minimal invasive studies focused on retrocalcaneal bursitis instead of insertional Achilles tendinopathy [29, 49]. Three studies used a medial incision: two a midline or central incision and one a lateral incision. All techniques involved resection of the posterosuperior calcaneal prominence, retrocalcaneal bursa and intratendinous calcifications. All studies detached the AT partially or in total, reinserted the AT with bone anchors or performed augmentation (plantaris tendon or FHL). Despite the (minor) differences in surgical technique, there were large differences in complication rate. One study reported no major and only 7.5 % minor complications [12]. Others reported 23 % major and 59 % overall complications [32]. Although the difference in complication rate was evident, there was almost no difference in patient satisfaction (Table 5). Outcome on pain scores (e.g. VAS) was scarcely reported [12, 53]. Based on the included studies, it is not possible to draw any conclusions regarding the best surgical technique for insertional Achilles tendinopathy.
Non-surgical treatment
Injections
Two studies evaluated medicinal injections as a minimal invasive treatment [37, 44]. Sclerosing polidocanol was injected as well as hyperosmolar dextrose. As the included study with sclerosing polidocanol is only a pilot, with hitherto no subsequent study, the positive outcome should be considered with care. Hyperosmolar dextrose injections for tendinopathies have been studied rarely, albeit the positive results raise expectations, clinical use should be with caution.
Eccentric exercises
Four studies evaluated the outcome of eccentric exercises for insertional Achilles tendinopathy [13, 22, 26, 42]. There were some important differences between treatment protocols; most notably, the difference between full range of motion exercises and floor level exercises. Evaluating the separate results an important difference was found: good outcomes for floor level exercises compared to insufficient results of full range of motion studies (Table 5). All studies used a 12-week training protocol with painful exercises 2 or 3 times daily, with up to three sets of 10–15 repetitions each. However, all studies had a relative short follow-up as the longest was 4 months. Despite the good outcome for midportion Achilles tendinopathy with full range of motion eccentric exercises, and in contrast with the statement of a previous systematic review, full range eccentric training may not be the first treatment of choice for insertional Achilles tendinopathy as the patient satisfaction is unfavourable compared to other conservative treatment modalities for insertional Achilles tendinopathy [24]. 70 % of all patients were unsatisfied after a 12-week full range eccentric training regime (Table 5). Although evaluated in only one study, the results of floor level eccentric exercises are much more promising: 67 % per cent satisfied after floor level compared to 30 % satisfied after full range exercises. The focus of eccentric treatment should therefore be on floor level exercises.
Extracorporeal shockwave therapy
One prospective study and one randomized controlled trial evaluated ESWT for insertional Achilles tendinopathy [14, 42]. The same study group performed both studies. A low-to-medium energy ESWT was given without the use of anaesthesia. The RCT and prospective study both showed good results. A decrease in subjective pain scale (−4.8) and high patient satisfaction were found (Table 5). For the prospective study, it should be noted that the patient selection was biased on insurance claim and the control group received not more than a wait-and-see protocol, the outcome may therefore be affected by placebo effect.
Others
One study evaluated Laser CO2 with TECAR and cryoultrasound [10]. All showed significant decrease on a VAS. Although the results seem promising, the study included only 15 patients with insertional problems, the three different groups consisted of merely five patients. No other studies evaluated the outcome of these treatments; additional evidence is a necessity as the current evidence is too weak to draw conclusions or to provide a clinical treatment advice.
Calcifications versus no calcifications
Nine of 14 studies reported on the presence of a bony disorder, located at the insertion of the AT into the calcaneus, in every case [12, 15, 20, 22, 26, 31, 37, 42, 53]. Four of six studies evaluating surgery for insertional Achilles tendinopathy reported on bony disorders [12, 20, 30, 53]. In addition, the diagnostic method was based on imaging in 12 studies, and this was unclear in two other studies (Table 3). This is important, as the outcome of a treatment could be different in patients with bony pathology compared to a group without bony pathology. Hence, imaging is essential in the diagnoses and thus treatment for insertional Achilles tendinopathy. Future research should differentiate between and/or compare treatments in a group with bony disorder and a group without bony disorder.
Study limitations and clinical relevance
The most important limitation of this study is the low level of evidence of included studies and the substantial risk of bias herein. Only one randomized controlled trial could be included; most studies were prospective or retrospective in design. Another important limitation is the terminological confusion surrounding Achilles tendon pathology [18, 19, 30, 38, 50]. This systematic review used strict inclusion criteria to define insertional Achilles tendinopathy; as a result, studies may be excluded based on the used terminology. As insertional Achilles tendinopathy differs from other chronic Achilles tendon pathology, the results of this analysis are largely dependent on the proper diagnosis and terminology of the included studies [30, 31, 35, 45, 50, 52]. Although all studies reported that the diagnosis was based on clinical findings and different imaging techniques, patient’ symptoms may have been based on other pathology instead of insertional Achilles tendinopathy (e.g. retrocalcaneal bursitis). Finally, insertional Achilles tendinopathy may occur together with retrocalcaneal bursitis, if patients have this combination and are treated for one or the other a minimal effect of intervention can be expected [1]. A comparison between these entities after surgical intervention was made by Watson [52]; he found different results between these pathologies in spite of the same surgical intervention, hereby reemphasizing the difference between these pathologies.
Despite the generally low level of quality of available studies, the outcome is of clinical importance [4]. This study is the first to evaluate the effectiveness of non-surgical and surgical interventions for insertional Achilles tendinopathy based on patient satisfaction, pain and complication rates. In addition, it points at the clear distinction (in outcome) between the currently used eccentric exercises protocols for insertional Achilles tendinopathy; finally, it shows the importance of differentiation between calcified and non-calcified insertional Achilles tendinopathy.
Conclusion
It was found that there are numerous treatment modalities, non-surgical and surgical, for insertional Achilles tendinopathy. Regarding non-surgical treatment, although both showed a decrease in VAS score, a substantial difference was found between the outcome of full range eccentric exercises and floor level exercises in insertional Achilles tendinopathy; full range of motion exercises resulted in a low patient satisfaction compared to floor level exercises or other treatment modalities. The results of floor level eccentric exercises are promising but currently evaluated by only one study. ESWT, although based on only two studies, appears effective in patients with non-calcified insertional Achilles tendinopathy. Evaluation by other study groups would substantially strengthen the current positive position of ESWT. Different surgical techniques are used to treat insertional Achilles tendinopathy. There are some differences in outcome, mainly regarding complication rate. Despite these differences, the patient satisfaction is relatively high in all surgical studies. Based on the available studies, it is not possible to draw any conclusion regarding the best surgical technique for insertional Achilles tendinopathy. Finally, it is evident that more high level evidence studies are necessary to be more conclusive regarding the best available treatment. Future studies should focus on clearly stating the exact studied pathology (bony involvement/not) and use validated outcome measures.
References
Aaron DL, Patel A, Kayiaros S, Calfee R (2011) Four common types of bursitis: diagnosis and management. J Am Acad Orthop Surg 19:359–367
Aronow MS (2005) Posterior heel pain (retrocalcaneal bursitis, insertional and noninsertional Achilles tendinopathy). Clin Podiatr Med Surg 22:19–43
Astrom M, Westlin N (1992) No effect of piroxicam on achilles tendinopathy. A randomized study of 70 patients. Acta Orthop Scand 63:631–634
Bhandari M, Montori VM, Devereaux PJ, Wilczynski NL, Morgan D, Haynes RB (2004) Doubling the impact: publication of systematic review articles in orthopaedic journals. J Bone Joint Surg Am 86-A:1012–1016
Calder JD, Saxby TS (2003) Surgical treatment of insertional Achilles tendinosis. Foot Ankle Int 24:119–121
Carmont MR, Maffulli N (2007) Management of insertional Achilles tendinopathy through a Cincinnati incision. BMC Musculoskelet Disord 8:82
Chiara VM, Guzzini M, Ferretti A (2003) Operative treatment of chronic Achilles tendinopathy. Int Orthop 27:307–310
Clain MR, Baxter DE (1992) Achilles tendinitis. Foot Ankle 13:482–487
Coleman BD, Khan KM, Maffulli N, Cook JL, Wark JD (2000) Studies of surgical outcome after patellar tendinopathy: clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 10:2–11
Costantino C, Pogliacomi F, Vaienti E (2005) Cryoultrasound therapy and tendonitis in athletes: a comparative evaluation versus laser CO2 and t.e.ca.r. therapy. Acta Biomed 76:37–41
de Vos RJ, Weir A, van Schie HT, Bierma-Zeinstra SM, Verhaar JA, Weinans H, Tol JL (2010) Platelet-rich plasma injection for chronic Achilles tendinopathy: a randomized controlled trial. JAMA 303:144–149
Elias I, Raikin SM, Besser MP, Nazarian LN (2009) Outcomes of chronic insertional Achilles tendinosis using FHL autograft through single incision. Foot Ankle Int 30:197–204
Fahlstrom M, Jonsson P, Lorentzon R, Alfredson H (2003) Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc 11:327–333
Furia JP (2005) Extracorporeal shockwave therapy in the treatment of chronic insertional Achilles tendinopathy. Orthopade 34:571–578
Furia JP (2006) High-energy extracorporeal shock wave therapy as a treatment for insertional Achilles tendinopathy. Am J Sports Med 34:733–740
Furia JP (2008) High-energy extracorporeal shock wave therapy as a treatment for chronic noninsertional Achilles tendinopathy. Am J Sports Med 36:502–508
Gerken AP, McGarvey W, Baxter DE (1996) Insertional Achilles tendinitis. Foot Ankle Clin 1:237–248
Harris CA, Peduto AJ (2006) Achilles tendon imaging. Australas Radiol 50:513–525
Jerosch J, Schunck J, Sokkar SH (2007) Endoscopic calcaneoplasty (ECP) as a surgical treatment of Haglund’s syndrome. Knee Surg Sports Traumatol Arthrosc 15:927–934
Johnson KW, Zalavras C, Thordarson DB (2006) Surgical management of insertional calcific achilles tendinosis with a central tendon splitting approach. Foot Ankle Int 27:245–250
Jones DC, James SL (1984) Partial calcaneal ostectomy for retrocalcaneal bursitis. Am J Sports Med 12:72–73
Jonsson P, Alfredson H, Sunding K, Fahlstrom M, Cook J (2008) New regimen for eccentric calf-muscle training in patients with chronic insertional Achilles tendinopathy: results of a pilot study. Br J Sports Med 42:746–749
Kane TP, Ismail M, Calder JD (2008) Topical glyceryl trinitrate and noninsertional Achilles tendinopathy: a clinical and cellular investigation. Am J Sports Med 36:1160–1163
Kearney R, Costa ML (2010) Insertional achilles tendinopathy management: a systematic review. Foot Ankle Int 31:689–694
Kirkup J (1988) Mythology and History. In: Helal B, Wilson D (eds) The foot. Churchill Livingstone, Philadelphia, pp 1–8
Knobloch K (2007) Eccentric training in Achilles tendinopathy: is it harmful to tendon microcirculation? Br J Sports Med 41:e2
Knobloch K, Grasemann R, Spies M, Vogt PM (2008) Midportion achilles tendon microcirculation after intermittent combined cryotherapy and compression compared with cryotherapy alone: a randomized trial. Am J Sports Med 36:2128–2138
Leach RE, DiIorio E, Harney RA (1983) Pathologic hindfoot conditions in the athlete. Clin Orthop Relat Res 177:116–121
Leitze Z, Sella EJ, Aversa JM (2003) Endoscopic decompression of the retrocalcaneal space. J Bone Joint Surg Am 85:1488–1496
Maffulli N, Khan KM, Puddu G (1998) Overuse tendon conditions: time to change a confusing terminology. Arthroscopy 14:840–843
Maffulli N, Testa V, Capasso G, Sullo A (2004) Calcific insertional Achilles tendinopathy: reattachment with bone anchors. Am J Sports Med 32:174–182
McGarvey WC, Palumbo RC, Baxter DE, Leibman BD (2002) Insertional Achilles tendinosis: surgical treatment through a central tendon splitting approach. Foot Ankle Int 23:19–25
McLauchlan GJ, Handoll HH (2001) Interventions for treating acute and chronic Achilles tendinitis. Cochrane Database Syst Rev 10(8):CD000232
Morelli V, James E (2004) Achilles tendonopathy and tendon rupture: conservative versus surgical management. Prim Care 31:1039–1054
Myerson MS, McGarvey W (1999) Disorders of the Achilles tendon insertion and Achilles tendinitis. Instr Course Lect 48:211–218
Norregaard J, Larsen CC, Bieler T, Langberg H (2007) Eccentric exercise in treatment of Achilles tendinopathy. Scand J Med Sci Sports 17:133–138
Ohberg L, Alfredson H (2003) Sclerosing therapy in chronic Achilles tendon insertional pain-results of a pilot study. Knee Surg Sports Traumatol Arthrosc 11:339–343
Paavola M, Jarvinen TA (2005) Paratendinopathy. Foot Ankle Clin 10:279–292
Petersen W, Welp R, Rosenbaum D (2007) Chronic Achilles tendinopathy: a prospective randomized study comparing the therapeutic effect of eccentric training, the AirHeel brace, and a combination of both. Am J Sports Med 35:1659–1667
Philippot R, Wegrzyn J, Grosclaude S, Besse JL (2010) Repair of insertional achilles tendinosis with a bone-quadriceps tendon graft. Foot Ankle Int 31:802–806
Puddu G, Ippolito E, Postacchini F (1976) A classification of Achilles tendon disease. Am J Sports Med 4:145–150
Rompe JD, Furia J, Maffulli N (2008) Eccentric loading compared with shock wave treatment for chronic insertional achilles tendinopathy. A randomized, controlled trial. J Bone Joint Surg Am 90:52–61
Rompe JD, Furia J, Maffulli N (2009) Eccentric loading versus eccentric loading plus shock-wave treatment for midportion achilles tendinopathy: a randomized controlled trial. Am J Sports Med 37:463–470
Ryan M, Wong A, Taunton J (2010) Favorable outcomes after sonographically guided intratendinous injection of hyperosmolar dextrose for chronic insertional and midportion achilles tendinosis. AJR Am J Roentgenol 194:1047–1053
Schepsis AA, Jones H, Haas AL (2002) Achilles tendon disorders in athletes. Am J Sports Med 30:287–305
Stergioulas A, Stergioula M, Aarskog R, Lopes-Martins RA, Bjordal JM (2008) Effects of low-level laser therapy and eccentric exercises in the treatment of recreational athletes with chronic achilles tendinopathy. Am J Sports Med 36:881–887
Tallon C, Coleman BD, Khan KM, Maffulli N (2001) Outcome of surgery for chronic Achilles tendinopathy. A critical review. Am J Sports Med 29:315–320
Thomas JL, Christensen JC, Kravitz SR, Mendicino RW, Schuberth JM, Vanore JV, Weil LS Sr, Zlotoff HJ, Bouche R, Baker J (2010) The diagnosis and treatment of heel pain: a clinical practice guideline-revision 2010. J Foot Ankle Surg 49:S1–S19
van Dijk CN, van Dyk GE, Scholten PE, Kort NP (2001) Endoscopic calcaneoplasty. Am J Sports Med 29:185–189
van Dijk CN, van Sterkenburg MN, Wiegerinck JI, Karlsson J, Maffulli N (2011) Terminology for Achilles tendon related disorders. Knee Surg Sports Traumatol Arthrosc 19(5):835–841
Wagner E, Gould JS, Kneidel M, Fleisig GS, Fowler R (2006) Technique and results of Achilles tendon detachment and reconstruction for insertional Achilles tendinosis. Foot Ankle Int 27:677–684
Watson AD, Anderson RB, Davis WH (2000) Comparison of results of retrocalcaneal decompression for retrocalcaneal bursitis and insertional achilles tendinosis with calcific spur. Foot Ankle Int 21:638–642
Yodlowski ML, Scheller AD Jr, Minos L (2002) Surgical treatment of Achilles tendinitis by decompression of the retrocalcaneal bursa and the superior calcaneal tuberosity. Am J Sports Med 30:318–321
Conflict of interest
No financial or material support was received.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wiegerinck, J.I., Kerkhoffs, G.M., van Sterkenburg, M.N. et al. Treatment for insertional Achilles tendinopathy: a systematic review. Knee Surg Sports Traumatol Arthrosc 21, 1345–1355 (2013). https://doi.org/10.1007/s00167-012-2219-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-012-2219-8