
Abstract
Background
There are an estimated 40,000 to 90,000 injection opiate users in Canada. The social, economic and health consequences of opiate addiction have been well documented. However, there are no data on the self-perceived health status of opiate users in Canada. Therefore, the goal of this research is to gain an understanding of the selfperceived health status of opiate users by comparing the health-related quality of life of opiate users to chronic disease populations and to the general population.
Methods
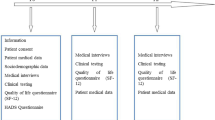
The SF-36 was administered to a nonrandom sample of 143 opiate users entering low-threshold methadone treatment. Two sample t-tests were performed to assess statistical differences, at a 5% level of significance, between population scores across SF-36 dimensions.
Results
Opiate users perceived both their mental and physical health as worse than the general population and individuals with minor and serious medical problems, but comparable to those with diagnosed psychiatric illnesses.
Conclusions
Methadone treatment services should incorporate both primary care and psychiatric care into their programs, or at the very least secure appropriate referral mechanisms to ancillary services to ensure that the health concerns of opiate users are dealt with in the context of their treatment program.
Résumé
Contexte
Selon les estimations, il y aurait entre 40 000 et 90 000 utilisateurs d’opiacés injectables au Canada. Les conséquences sociales, économiques et sanitaires des toxicomanies opiacées sont bien documentées, mais il n’existe aucune donnée sur l’état de santé autoperçu des utilisateurs d’opiacés au Canada. Nous avons donc cherché à comprendre l’état de santé autoperçu des utilisateurs d’opiacés en comparant leur qualité de vie (du point de vue de la santé) à celle de personnes atteintes de maladies chroniques et de la population générale.
Méthode
Nous avons administré le questionnaire SF-36 à un échantillon non aléatoire de 143 utilisateurs d’opiacés qui entreprenaient un traitement à la méthadone à seuil bas. Nous avons ensuite exécuté deux tests t modèles afin d’évaluer l’écart statistique, à un seuil de signification de 5 %, entre les notes obtenues par les segments démographiques selon les volets du questionnaire.
Résultats
L’état de santé mentale et physique perçu par les utilisateurs d’opiacés était pire que dans la population générale et pire que chez les personnes atteintes de problèmes de santé mineurs ou graves, mais il était comparable à l’état de santé perçu des personnes ayant un diagnostic de maladie psychiatrique.
Conclusions
Les services de traitement à la méthadone devraient intégrer à la fois des soins primaires et psychiatriques dans leurs programmes, ou à tout le moins des mécanismes d’aiguillage appropriés vers des services complémentaires, pour que l’on s’occupe des préoccupations de santé des utilisateurs d’opiacés dans le cadre de leur traitement.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Fischer B, Gliksman L, Rehm J, Daniel N, Medved W. Comparing opiate users in methadone treatment with untreated opiate users: Results of a follow-up study with a Toronto opiate user cohort. Can J Public Health 1999;90(5):299–303.
Single E, Robson L, Xie X, Rehm J. The economic costs of alcohol, tobacco and illicit drugs in Canada, 1992. Addiction 1998;93(7):991–1006.
Ralston GE, Wilson P. Methadone programs: The costs and benefits to society and the individual. Pharmacoeconomics 1996;10(4):321–26.
Anonymous. Effective medical treatment of opiate addiction. National Consensus Development Panel on Effective Medical Treatment of Opiate Addiction. JAMA 1998;280(22):1936–43.
Ward J, Hall W, Mattick RP. Role of maintenance treatment in opioid dependence. The Lancet 1999;353(9148):221–26.
Ryan CF, White JM. Health status at entry to methadone maintenance treatment using the SF36 health survey questionnaire. Addiction 1996;91(1):39–46.
Stein MD, Mulvey KP, Plough A, Samet JH. The functioning and well being of persons who seek treatment for drug and alcohol use. J Substance Abuse 1998;10:75–84.
Schlenk EA, Erlen JA, Jacob- Dunbar J, McDowell J, Engberg S, Sereika SM, et al. Health-related quality of life in chronic disorders: A comparison across studies using the MOS SF-36. Quality Life Res 1998;7:57–65.
Centers for Disease Control and Prevention. Measuring Healthy Days. Atlanta, GA: CDC, November 2000.
Hartgers C, van den Hoek A, Krijnen P, Coutinho RA. HIV prevalence and risk behaviour among injecting drug users who participate in ‘Low-Threshold’ methadone programs in Amsterdam. Am J Public Health 1992;82(4):547–51.
van Ameijden EJ, Langendam MW, Coutinho RA. Dose-effect relationship between overdose mortality and prescribed methadone dosage in low-threshold maintenance programs. Addictive Behav 1999;24(4):559–63.
Finch E, Groves I, Feinmann C, Farmer R. A low-threshold methadone stabilisation programme description and first stage evaluation. Addiction Res 1995;3(1):63–71.
Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992;30:473–83.
Ware JE, Snow KK, Kosinski M. SF36 Health Survey: Manual and Interpretation Guide. Lincoln, RI: QualityMetric Incorporated, 1993, 2000.
Ware JE, Kosinski M, Keller SD. SF36 Physical and Mental Health Summary Scales: A User’s Manual. Boston, MA: Health Assessment Lab, 1994.
Hopman WM, Towheed T, Anastassiades T, Tenenhouse A, Poliquin S, Berger C, et al. Canadian Normative Data for the SF36 Health Survey. CMAJ 2000;163(3):265–71.
McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care 1993;31(3):247–63.
Birrell FN, Hassell AB, Jones PW, Dawes PT. How does the Short Form 36 Health Questionnaire (SF36) in Rheumatoid Arthritis (RA) relate to RA Outcomes measures and SF-36 Population Values? A cross-sectional study. Clinical Rheumatology 2000;19:195–99.
Heyland DK, Hopman W, Coo H, Tanmer J, McColl MA. Long-term health-related quality of life in survivors of sepsis. Short Form 36: A valid and reliable measure of health-related quality of life. Crit Care Med 2000;28(11):3599–605.
Madalinska JB, Essink- Bot ML, de Koing HJ, Wim J, van der Mass PJ, Schroder FH. Healthrelated quality of life effects of radical prostatectomy and primary radiotherapy for screen detected or clinically diagnosed localized prostate cancer. J Clin Oncology 2001;19(6):1619–28.
Singer MA, Hopman WM, MacKenzie TA. Physical functioning and mental health in patients with chronic medical conditions. Q Life Res 1999;8:687–91.
Wiebe S, Matijevic S, Eliasziw M, Derry PA. Clinically important change in quality of life in epilepsy. J Neurology, Neurosurgery, Psychiatry 2002;73(2):116–20.
Rothman KJ. Modern Epidemiology. Boston: Little Brown and Company, 1986.
Rounsaville BJ, Weissman MM, Kleber H, Wilber C. Heterogeneity of psychiatric diagnosis in treated opiate addicts. Arch Gen Psychiatry 1982;39:161–68.
Brands J, Brands B, Marsh D. The expansion of methadone prescribing in Ontario, 1996–1998. Addiction Res 2000;8(5):485–96.
Author information
Authors and Affiliations
Corresponding author
Additional information
Acknowledgements: This study was originally funded by National Health Research and Development Program (NHRDP) grant no. 6606-06-2000, with continued support from the Canadian Institute for Health Research (CIHR) grant HHP-50150. Dr. Millson is supported by a Scientist Award from the Ontario HIV Treatment Network (OHTN). We gratefully acknowledge the methadone programme staff for their assistance with recruitment, and the study participants for their time and effort in being part of this study.
Rights and permissions
About this article
Cite this article
Millson, P.E., Challacombe, L., Villeneuve, P.J. et al. Self-perceived Health Among Canadian Opiate Users. Can J Public Health 95, 99–103 (2004). https://doi.org/10.1007/BF03405775
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03405775