
Abstract
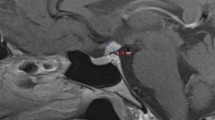
Lymphocytic hypophysitis is classically defined as an inflammatory disorder confined to adenohypophysis. However, it has recently been indicated that infundibuloneurohypophysitis underlies some subsets of central diabetes insipidus (DI). Therefore, lymphocytic hypophysitis can be considered a syndrome including disorders of both the anterior pituitary (lymphocytic adenohypophysitis) and the posterior pituitary (lymphocytic infundibuloneurohypophysitis). We describe a 77-yr-old woman with lymphocytic hypophysitis presenting with headache, diplopia, general malaise and appetite loss. Head magnetic resonance imaging (MRI) demonstrated pituitary swelling and dura mater thickening on the dorsum sella. Endocrinological investigations revealed both anterior and posterior pituitary dysfunction associated with primary hypothyroidism due to Hashimoto’s thyroiditis. Headache and diplopia spontaneously disappeared, and anterior pituitary dysfunction, general malaise and appetite loss improved after taking 10 mg hydrocortisone daily, although ACTH hyposecretion persisted. Pituitary swelling was thereafter reduced but the dura mater thickening persisted. We suggest that this case may represent a variant of lymphocytic hypophysitis in which chronic inflammatory process involves both the anterior and the posterior pituitary gland, infundibulum, dura mater on the dorsum sella and cavernous sinus. Regarding expanding features of lymphocytic hypophysitis, it may be considered a syndrome including heterogeneous disorders, of which the pathogenesis remains to be elucidated.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Goudie R.B., Pinkerton P.H. Anterior hypophysitis and Hashimoto’s disease in a young woman. J. Path. Bact. 1962, 83: 584–585.
Cosman F., Post K.D., Holub D.A., Wardlaw S.L. Lymphocytic hypophysitis: report of 3 new cases and review of the literature. Medicine 1989, 68: 240–256.
Imura H., Nakao K., Shimatsu A., Ogawa Y., Sando T., Fujisawa I., Yamabe, H. Lymphocytic infundibuloneurohypophysitis as a cause of diabetes insipidus. N. Engl. J. Med. 1993, 329: 683–689.
Koshiyama H., Sato H., Yorita S., Koh T., Kanatsuna T., Nishimura K., Hayakawa K., Takahashi J., Hashimoto N. Lymphocytic hypophysitis presenting with diabetes insipidus. Endocr. J. 1994, 41: 93–97.
Abe T., Matsumoto K., Sanno N., Osamura Y. Lymphocytic hypophysitis: case report. Neurosurgery 1995, 36: 1016–1019.
Nussbaum C.E., Okawara S., Jakobs L.S. Lymphocytic hypophysitis with involvement of the cavernous sinus and hypothalamus. Neurosurgery 1991, 28: 440–444.
Thodou E., Asa S.L., Kontogeorgos G., Kovacs K., Horvath E., Ezzat S. Clinical case seminar: lymphocytic hypophysitis: clinicopathoplogical findings. J. Clin. Endocrinol. Metab. 1995, 80: 2302–2311.
Li J.Y., Lai P.H., Lam H.C., Lu L.Y., Cheng H.H., Lee J.K., Lo Y.K. Hypertrophic cranial pachymeningitis and lymphocytic hypophysitis in Sjögren’s syndrome. Neurology 1999, 52: 420–423.
Koshiyama H., Koh T, Shimatsu A., Nakao K. The effect of steroid therapy on broad type of lymphocytic hypophysitis. Proc 77th Meeting of the Endocrine Society, Washington, DC, 1995, p. 486.
Supler M.L., Mickle J.P. Lymphocytic hypophysitis: report of a case in a man with cavernous sinus involvement. Surg. Neurol. 1992, 37: 472–476.
Ikeda J., Kuratsu J., Miura M., Kai Y., Ushio Y. Lymphocytic adenohypophysitis accompanying occlusion of bilateral internal carotid arteries. Neurol. Med. Chir. (Tokyo) 1990, 30: 346–349.
Honegger J., Fahlbusch R., Bornemann A., Hensen J., Buchfelder M., Müller M., Nomikos P. Lymphocytic and granulomatous hypophysitis: experience with nine cases. Neurosurgery 1997, 40: 713–273.
Hama S., Arita K., Kurisu K., Sumida M., Kurihara K. Parasellar chronic inflammatory disease presenting Tolosa-Hunt syndrome, hypopituitarism and diabetes insipidus: a case report. Endocr. J. 1996, 43: 503–510.
Hida C., Yamamoto T., Endo K., Tanno Y., Saito T., Tsukamoto T. Inflammatory involvement of the hypophysitis in Tolosa-Hunt syndrome. Intern. Med. 1995, 34: 1093–1096.
Olmos P.R., Falko J.M., Rea G.L., Boesel C.P., Chakeres D.W., McGhee D.B. Fibrosing pseudotumor of the sella and parasellar area producing hypopituitarism and multiple cranial nerve palsies. Neurosurgery 1993, 32: 1015–1021.
Scanarini M., D’Avella D., Rotilio A., Kitromilis N., Mingrino S. Giant-cell granulomatous hypophysitis: a distinct clinicopathological entity. J. Neurosurg. 1989, 71: 681–686.
Ahmed S.R., Aiello D.P., Page R., Hopper K., Towfighi J., Santen R.J. Necrotizing infundibulo-hypophysitis: a unique syndrome of diabetes insipidus and hypopituitarism. J. Clin. Endocrinol. Metab. 1993, 76: 1499–1504.
Bevans J.S., Othman S., Lazarus J.H., Parkes A.B., Hall R. Reversible adenocorticotropin deficiency due to probable autoimmune hypophysitis in a woman with postpartum thyroiditis. J. Clin. Endocrinol. Metab. 1992, 74: 548–552.
Hashimoto K., Takao T., Makino S. Lymphocytic adenohypophysitis and lymphocytic infundibuloneurohypophysitis. Endocr. J. 1997, 44: 1–10.
Jensen M.D., Handwerger B.S., Scheithauer B.W., Carpenter P.C., Mirakian R., Banks P.M. Lymphocytic hypophysitis with isolated corticotropin deficiency. Ann. Intern. Med. 1986, 105: 200–203.
Komatsu M., Kondo T., Yamauchi K., Yokokawa N., Ichikawa K., Ishihara M., Aizawa T., Yamada T., Imai Y., Tanaka K., Taniguchi K., Watanabe T., Takahashi Y. Antipituitary antibodies in patients with the primary empty sella syndrome. J. Clin. Endocrinol. Metab. 1988, 67: 633–638.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Nakamura, Y., Okada, H., Wada, Y. et al. Lymphocytic hypophysitis: Its expanding features. J Endocrinol Invest 24, 262–267 (2001). https://doi.org/10.1007/BF03343856
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03343856