
Abstract
Substantial advances have accrued over the last decade in the identification of the processes that contribute to lymphatic vascular development in health and disease. Identification of distinct regulatory milestones, from a variety of genetic models, has led to a stepwise chronology of lymphatic development. Several molecular species have been identified as important tissue biomarkers of lymphatic development and function. At present, vascular endothelial growth-factor receptor (VEGFR)-3/VEGF-C/VEGF-D signaling has proven useful in the identification of clinical lymphatic metastatic potential and the assessment of cancer prognosis. Similar biomarkers, to be utilized as surrogates for the assessment of inherited and acquired diseases of the lymphatic circulation, are actively sought, and will represent a signal advance in biomedical investigation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1. The Lymphatic System
As an adjunct to the closed blood circulatory system, the lymphatic vasculature maintains fluid and colloid homeostasis through an extensive network of open-ended vessels distributed throughout the body. Circulatory dynamics require that fluid and macromolecules exit the blood capillary lumen into the interstitial space; a substantial fraction of this extravasated extracellular fluid must return to the central circulation as the protein-rich fluid known as lymph. Driven by pressure gradients that emanate from the concerted action of musculoskeletal movement, respiration, smooth muscle contraction, and one-way valves, lymph is drawn from interstitial tissue spaces into an increasingly larger hierarchy of lymphatic vessels, ultimately reaching the venous circulation by way of the thoracic duct. Both anatomically and functionally, the lymphatic system participates in important physiological functions, including immune surveillance, and the absorption and transport of dietary fats. Moreover, the lymphatic vasculature constitutes the conduit system in which circulating dendritic cells and lymphocytes traverse the body, monitoring tissues for microbial intrusion and forming the sites of antigen presentation and recognition in sentinel and regional lymph nodes, thereby comprising the infrastructure of acquired immunity.[1,2]
1.1 Lymphatic Anatomy
Lymphatic capillaries arborize as superficial plexuses lined with a single layer of unfenestrated lymphatic endothelial cells (LECs). Unlike blood vessels, LECs lack a continuous basement membrane, allowing lymph to follow osmotic and colloid gradients at overlapping cell junctions.[3] Fibrillin-containing filaments anchor the lymphatic capillaries to the interstitium, thereby facilitating the opening of LEC junctions at times of increased interstitial pressure.[4] Fluid, macromolecules, and cells passively flow into the capillary lumen and travel to collecting lymph vessels deeper within the dermal layers. These larger lymphatics actively propel lymph through the contraction of their vascular smooth muscle, aided by the presence of intraluminal unidirectional valves. These collecting lymphatics coalesce to create vessels of increasing caliber, culminating in the formation of the cisterna chyli and thoracic duct.
1.2 Lymphatic Dysfunction
Given the central role of the lymphatic system in circulatory, metabolic, and immune-related homeostasis, it is not surprising that lymphatic vascular dysfunction can manifest within various predictable sequelae, ranging from impaired immune responses[5] and metabolic status[6] to the appearance of a debilitating and disfiguring form of regional swelling known as lymphedema.[7] It is somewhat paradoxical that, historically, the central physiological and pathological importance of the lymphatic system has not stimulated a proportional degree of scientific exploration into the basis of lymphatic health and disease. As a consequence, the diagnosis and treatment of patients with lymphatic diseases has relied chiefly upon empirically derived insights, often with limited success.
More recently, however, scientific investigation of the lymphatic vasculature has benefited specifically from more focused scientific attention to the pathophysiology of cancer metastasis.[8–11] Tissue cultures of blood vascular endothelial cells and lymphatic endothelial cells derived from human skin have been characterized, allowing cell-based in vitro studies.[12–15] Moreover, animal models of lymphatic disease, unavailable until quite recently,[16] have been realized for distinct forms of congenital and acquired lymphedema[17–19] [table I]. The availability of suitable disease-specific animal models, along with a growing comprehension of lymphatic biology[10,20,21] and the more recent identification of lymphatic-specific biomarkers,[22,23] ensure the requisite insight and investigative tools to permit in-depth investigation and putative therapies of the broad array of lymphatic diseases.

Genetic mouse models of lymphatic disease (reproduced from Cueni and Detmar,[24] with permission from Macmillan Publishers Ltd)
1.3 Lymphatic Development
Although the lymphatic vasculature has been anatomically recognized for centuries[42] and its embryonic origins proposed more than one hundred years ago,[43] it is only recently that the development of the mammalian lymphatic system has been elucidated with convincing evidence. Identification of distinct regulatory milestones, from a variety of genetic models, has led to a stepwise chronology of lymphatic development. The non-disjunct physiological progression of lymphangiogenesis can be generalized into four distinct stages: (i) lymphatic competence; (ii) lymphatic commitment; (iii) lymphatic specification; and (iv) lymphatic vessel coalescence and maturation. Endothelial cells of embryonic veins are believed to be the source of lymphatic progenitors that develop under the coordinated influence of lymphatic-specific signals.[44] All endothelial cells of the cardinal vein possess the ability or competence to develop along the lymphatic-fate continuum, but the passive existence of the hemovasculature alone is not sufficient to induce lymphangiogenesis,[44] revealing a distinctive developmental divergence governing the lymphatic and blood vasculature lineages. Comparative microarray analyses of adult blood vascular endothelial cell (BEC)- and LEC-restricted transcriptomes have revealed that ≈98% of all genes identified are expressed at statistically indistinguishable levels within the two cell types.[15,45] Differences, however, do exist and these features have been recently reviewed.[21,24]
1.3.1 Competence
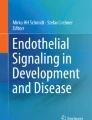
LEC competence represents the first step in the process of lymphatic commitment, within which all endothelial cells of the embryonic cardinal vein display an independent ability to respond to the (as yet, unidentified) initiating and instructive factor(s) of lymphatic development (figure 1). This process is initiated by mouse embyronic day 9–9.5.[44] The priming of LECs to initiate lymphatic development is likely dependent on a form of molecular signaling that is distinct from that found in blood vascular development, given the secondary but independent appearance of lymphatic vessels after blood vascular vasculogenesis is initiated. At present, LEC competence is defined by the surrogate expression of lymphatic vessel endothelial hyaluronan receptor-1 (LYVE1) and vascular endothelial growth factor receptor-3 (VEGFR3; also known as Flt-4).[24] Nevertheless, lymphatic competence is a dynamic state, encompassing events limited to the venous vascular endothelium and distinct from the biology of arterial endothelium. While the physiological functions of the VEGFR3 receptor and its pro-angiogenic vascular endothelial growth factor (VEGF) family of ligands have benefited from intense investigation, the function of the LYVE1 receptor remains largely enigmatic, even though its identification as a lymphatic-specific cellular marker constituted a seminal advance in the study of lymphatic vascular biology.[46]

Model for differentiation of the murine lymphatic vasculature. The figure summarizes a proposed four-step model for the formation of the lymphatic vasculature (reproduced from Oliver,[44] with permission from Macmillan Publishers Ltd). D6 = B-chemokine receptor D6; E = embryonic day; LEC = lymphatic endothelial cell; LYVE1 = lymphatic vessel endothelial hyaluronan receptor 1; Net = ETS-domain protein ELK3; NRP2 = neuropilin 2; PROX1 = prospero-related homeobox 1; SLC = secondary lymphoid chemokine; VEGF-C = vascular endothelial growth factor C; VEGFR3 = vascular endothelial growth-factor receptor 3.
LYVE1 was initially cloned as a homolog of CD44.[47,48] CD44 serves as a transmembrane glycoprotein receptor for the extracellular matrix glycosaminoglycan, hyaluronan, but binds other molecules, including osteopontin, collagens, and matrix metalloproteinases that participate in a variety of cellular processes, including lymphocyte migration and activation, hematopoiesis, and tumor metastasis.[49] Although LYVE1 has been shown to be closely associated with the lymphatic vasculature throughout development and maturity, the precise function of the receptor remains unknown, beyond its presumed involvement in the process of hyaluronan metabolism.[46] The primary receptor for hyaluronic acid, CD44 is known to facilitate cell migration by the removal of pericellular matrix surrounding fibroblast and epithelial cells, and the suppression of intercellular adhesion in processes of wound healing, inflammation, and tumor progression.[21,50] Hence, LYVE1, beyond its utility as a lymphatic endothelial marker, may potentially play an active role in both pathologic and physiologic lymphangiogenesis, through its ability to transport hyaluronic acid across the lymphatic vessel wall. The recent characterization of phenotypically normal LYVE1−/− knockout mice, which possess no overt structural or functional lymphatic or immunological abnormality, suggests that LYVE1 does not exclusively control lymphatic development or integrity but, rather, that it exerts an influence of a much more restricted or compensated scope.[20,51]
LYVE1 is expressed early on BECs, during lymphatic competence.[35] Throughout development, and with few exceptions (most notably macrophages and hepatic sinusoidal blood capillaries after birth), LYVE1 is associated exclusively with vessel and lymph node endothelia to terminal differentiation,[47,52] except for the collecting lymphatic vessels of the mature vasculature where LYVE1 is downregulated.[27] Nearly exclusive localization to lymphatic endothelium, and technical manipulability, confers LYVE1 the ability to serve as a valuable molecular and histochemical marker. Identification of this marker has permitted much more detailed study of the lymphatic vasculature where, previously, discrimination from blood vessels was difficult or impossible.[44,53] Prior methods of lymphatic vascular identification were limited to histological assessment of gross lymphatic-specific features, such as their endoluminal valves and lack of basement membrane, clearly limited by imprecision and lack of resolution.
Prior to the identification of the LYVE1, substantial investigative effort was centered on the VEGFR3 receptor, given the functional importance of the VEGF family of ligands and the relevant receptor expressed on the lymphatic endothelium.
VEGF is a key regulator of the endothelial cell functions required for vasculogenesis and for physiological and pathological angiogenesis.[54,55] The VEGF family includes seven members: VEGF-A, VEGF-B, VEGF-C, VEGF-D, VEGF-E, VEGF-F and placental growth factor (PlGF), and three receptors, VEGFR1 (also known as Fms-like tyrosine kinase, Flt-1), VEGFR2 (also known as fetal liver kinase, Flk-1), and VEGFR3 (Flt-4).[56] Of these, VEGF-C and VEGF-D and their cognate receptor, VEGFR3, represent the first and best studied of the lymphatic-specific signaling mechanisms.[57–62]
In contrast to LYVE1, VEGFR3 is broadly expressed on both early blood and lymphatic vessel endothelium, and plays a critical role in the development of both lineages of vasculature.[63] Targeted gene inactivation of VEGFR3 results in early cardiovascular collapse, demonstrating the development of the hemovasculature before the lymphatic system and, hence, precludes the ability to study the resulting dysfunction of lymphatic vessels.[40] In time, VEGFR3 expression becomes limited to LECs as expression is downregulated in BECs and, by the arrival of vascular maturity, VEGFR3 is largely restricted to the lymphatic endothelium,[57,64] further supporting the venous origin of the lymphatic system. However, VEGFR3 expression has also been detected on proliferating blood capillaries associated with tumor neovascularization or within wound granulation tissue;[60,65] thus, VEGFR3 alone may not possess sufficient specificity to serve as a lymphatic vascular marker, particularly under nonhomeostatic conditions. The identified ligands for VEGFR3, VEGF-C, and VEGF-D, have been characterized as pro-lymphangiogenic factors in a number of models of varying developmental and postnatal stages,[38,56,58,66–68] and with respect to both therapeutic potential[18,69,70] and cancer metastasis.[71] In conjunction with VEGF-C and VEGF-D, the angiopoietin signaling system participates in the formation of both blood and lymphatic vessels. Although considered antagonists with respect to angiogenesis,[72,73] angiopoietin 1 (ANG1) and angiopoietin 2 (ANG2) cooperatively induce lymphangiogenesis as an agonist of the endothelial-specific receptor tyrosine kinase TIE2.[26,73–75] Such signaling is responsible for lymphatic remodeling following differentiation, forming functionally mature lymphatics through lymphangiogenesis. Podoplanin (PDPN), also known as T 1α, is an integral glycoprotein found in the plasma membrane of podocytes and co-localizes with VEGFR3 in early lymphatic structures by mouse embryonic day 11 in a number of tissues.[76] Unlike VEGFR3, however, T1α/podoplanin is not expressed either on adult hemovascular endothelium or tumor vasculature.[77]
1.3.2 Commitment
Lymphatic commitment is marked developmentally and functionally by the expression of prospero-related homeobox 1 (PROX1), a nuclear transcription factor that, unlike LYVE1 and VEGFR3, is expressed exclusively in cells of committed lymphatic lineage.[35] The PROX1-positive subpopulation of venous endothelial cells wholly constitutes the progenitors of the mature lymphatic system, arrayed in a polarized fashion along the cardinal vein.[64] The mechanism of this differential and ordered expression remains unknown; nevertheless, PROX1 is clearly necessary and sufficient for lymphatic commitment. The molecular milieu in which PROX1 operates is also not known; both the downstream initiating and regulatory factors and the other upstream requisite or supplemental events have yet to be identified. PROX1−/− knockout mice proceed to bud LECs from the cardinal vein but fail to commit to the lymphatic lineage and, subsequently, fail to express later lymphatic-specific markers including LYVE1, instead retaining blood vascular markers.[64] PROX1 thus shifts commitment of venous endothelial cells from a default blood vascular fate to that of lymphatic lineage.[53,64,78] Consistent with these impressions in mice, overexpression of PROX1 in tissue culture induces expression of lymphatic-specific genes. Hemovascular-specific genes in venous endothelial cells are reciprocally suppressed, while the expression of the lymphatic endothelial cell markers, podoplanin and VEGFR3, is upregulated.[79]
1.3.3 Specification and Maturation
A committed LEC eventually achieves complete autonomy from the local microenvironment of the cardinal vein and migrates peripherally during the lymphatic specification stage, even if adoptively isolated in culture.[13] As the LEC attains a higher level of differentiation, additional lymphatic-specific markers are expressed, while those that reflect putative blood vascular lineage are increasingly suppressed.[64] Developing LECs bud from the parental cardinal vein on mouse embryonic day 10.5, independently of further PROX1 influence, as the first morphologically concerted event of lymphangiogenesis.[53] Other factors, such as neuropilin-2 (NRP2), a mediator in the VEGFR-VEGF signaling pathways,[80,81] and T1α/podoplanin, a cell-surface glycoprotein,[34,77] are expressed by LECs as budding and migration seed the periphery throughout the embryo for the formation of nascent lymphatic structures known as primary lymphatic sacs. From these blind-ended constructs of specified LECs, secondary budding and migration characterize the final stage of lymphatic development. As these near terminally differentiated cells bud, they form capillaries in a centrifugal fashion to form lymphatic vasculature around tissues and organs.[24]
Maturation of LECs into differentiated lymphatic vessels establishes the foundation of the lymphatic vasculature by mouse embryonic day 14.5,[82] which continues to organize until the first few days of postnatal life.[24] Additional lymphatic markers, such as desmoplakin and β-chemokine receptor D6, continue to be expressed in this late stage of terminal differentiation, and are thought to be among the last markers expressed. The mature lymphatic network shortly after birth expresses the complete profile of lymphatic markers found in adulthood.[44]
2. Secondary Lymphangiogenesis
The role of secondary lymphangiogenesis, beyond embryonic development, has not been well studied, except in the context of tumor biology. Lymphangiogenesis likely occurs in parallel with angiogenesis in the setting of wound healing and inflammation in a similar, transient fashion.[65] The growth of these lymphatics occurs de novo, originating from pre-existing lymphatic capillaries. Recent studies suggest that circulating lymphatic progenitor cells may, as well, play an important mechanistic role in secondary lymphangiogenesis.[83] The new vascular structures form in close proximity to, but separately from, blood vessels.[65,84] In diseases of known inflammatory etiology, such as psoriasis, as well as in chronic states of inflammation,[85] lesions exhibit exuberant changes of lymphangiogenesis. Whether these newly formed lymphatic vessels are functionally significant with persistence or resolution of chronic inflammation is not known.[24]
Much of the recent progress in understanding the process of lymphatic development has been made with respect to tumor biology, where metastatic spread through the lymphatic system is a prominent area of clinical interest. Dissemination of metastatic tumor cells to draining lymph nodes and seeding of secondary sites of tumorigenesis is a not uncommon phenomenon in many cancers. Staging of such spread confers substantial implication in patient prognosis.
Cancerous cells have classically been believed to gain access to the lymphatic circulation passively, invading local lymphatics randomly as the tumor expands. Recent evidence suggests a more active natural history of lymphangiogenic induction and metastatic transformation through tumor-mediated upregulation of both VEGFR3 and VEGF-C expression and signaling.[71,86,87] Blocking VEGFR3 suppresses cancerous spread.[88] Conversely, inhibition of lymphangiogenesis in transgenic mice expressing soluble VEGFR3 produces an acquired lymphedema phenotype.[89] Taken together, these observations suggest a central role for VEGFR3/VEGF-C signaling in proliferative lymphangiogenesis during tumor metastasis. Direct evidence has been adduced for cancers of the breast,[71] cervix,[90] pancreas,[86] prostate,[91] and others[3] (table II). Tumor-mediated expression of the primary VEGFR3 ligands, VEGF-C and VEGF-D, correlates with progression to metastasis, lending further support for the recruitment of lymphangiogenesis by aggressive tumors.[8] VEGF-C induces expression of the VEGFR3 receptor, leading to paracrine lymphangiogenic responses.[68]

Lymphatic features of human cancer and metastasis (reproduced from Ji,[21] with permission)
A number of clinical studies underscore the prognostic value of VEGF-C, VEGF-D, and VEGFR3 expression profiles and resultant lymphatic hyperplasia with regard to tumor progression,[92] regional lymph node metastasis,[91] patient survival,[93] and mortality.[94] The utility of VEGF-C/D and VEGFR3, individually and as a panel of biomarkers for pre-cancerous and cancerous staging, warrants further study. Pre-existing lymphatic vessels seem unaffected morphologically and functionally by prolonged VEGFR3 blockade. Systemic administration of an anti-VEGFR3 antibody may, thus, reduce tumor-associated lymphangiogenesis and cancer metastasis without affecting homeostatic lymphatic flow.[88,95,96] VEGF-A has been found to mediate tumor-induced proliferation of VEGFR2-positive lymphatic vessels prior to metastasis,[97] perhaps representing an anticipatory component of sentinel lymph node lymphangiogenesis and cancerous spread. This possible mechanism of increased metastatic potential has been extended recently to VEGF-C-expressing tumors,[98] and likewise presents an attractive target of intervention.
Despite the existence of circulating CD34+ endothelial progenitor cells (EPCs) into maturity,[99,100] the contribution of such a nidus of angiogenesis is controversial. Likewise, lymphatic endothelial progenitors have been discovered in the mature circulation but the degree to which they mediate secondary lymphangiogenesis in cancer is not yet understood. Incorporation of bone marrow-derived progenitor cells during cancer-associated lymphatic formation has not yet been documented,[96] although such association has been observed in other settings of lymphangiogenesis.[101,102]
3. Primary Lymphedema
The primary lymphedemas are developmental disorders in which the lymphatic vasculature fails to achieve a homeostatic capacity for fluid transport. These uncommon diseases most commonly arise at or following puberty in so-called Meige disease,[103] or hereditary lymphedema praecox. Lymphedema present at birth, or hereditary congenital lymphedema, carries the eponym of Milroy disease.[104] This autosomal-dominant inherited disorder is characterized, in many of the patient cohorts, by mutations in the VEGFR3 domain.[17,41,105] A murine model of Milroy disease, typified by a heterozygous inactivating mutation of the tyrosine kinase domain of VEGFR3, and poorly functional lymphatics, has been utilized to demonstrate a potential for curative gene therapy.[28] These so-called Chy mice (named for their propensity to develop chylous ascites) have hypoplastic lymphatic vessels. Ascites develops soon after birth, mirroring the disease of patients harboring the same mutation. Induction of functional lymphatic vessels in Chy mice has been observed through the overexpression of VEGFR3 ligands, supporting the sufficiency of VEGF-C/D signaling to promote lymphangiogenesis.[28] In the Chy animal model, lymphatic insufficiency and edema precedes dermal expansion and fibrosis[28] without apparent effect on the hemovascular system.[89]
Additional animal models have helped to identify possible genetic mechanisms to explain the presentation of primary lymphedema. Forkhead box C2 (FOXC2)−/−-knockout mice[106] reproduce the causative and physiological genetic defect of the lymphedema-distichiasis syndrome, a hereditary lymphedema characterized by the presence of distichiasis at birth and the onset of bilateral lower limb lymphedema by, or following, puberty.[107] In contrast to Milroy disease, where lymphatic hypoplasia predominates, lymphedema-distichiasis syndrome is characterized by normal or hyperplastic lymphatic vessels, suggesting that FOXC2 participates in the functional integrity of lymphatic vessels, with a less prominent developmental role. Indeed, FOXC2 is a critical transcription factor in pathways of metabolism, perhaps linking lymphatic dysfunction to insulin resistance.
A role for the transcription factor SOX18 (sex determining region Y-related high mobility group box 18) was recently identified in recessive and dominant forms of the rare hypotrichosis-lymphedema-telangiectasia syndrome,[41] characterized by the distinctive presentation of childhood hypotrichosis and lymphedema with telangiectasia or vascular nevi on the palmar surfaces.
T1α/PDPN−/− knockout mice also exhibit congenital lymphedema, with profoundly lymphedematous limbs at birth. Comparative anatomical and histological analysis between wild-type, heterozygote, and knockout animals reveals graded hyperplasticity of lymphatic vessels but the near-absence of lymphatic capillary and plexus formation.[82] Consistent with observed expression of T1α/podoplanin during developmental lymphatic speciation in vivo, T1α/podoplanin appears to be responsible for outlining the superficial capillary beds that anastomose with deeper lymphatic networks in the subcutaneous tissues.[82] Absence of T1α/podoplanin, therefore, facilitates the development of nascent lymphatics that are dysplastic, lacking the functional patterning and capacity of wild-type lymphatic vasculature. For the developmental disorders of lymphatic insufficiency, known etiological characteristics can be employed, such as the absence of VEGFR3 or PROX1, as biomarkers. Identification of more desirable, positively expressed circulating surrogates, however, remains elusive.
4. Secondary Lymphedema
Secondary lymphedema is a consequence of lymphatic stasis acquired through a variety of insinuating insults, a spectrum that includes, trauma, infection, surgery, radiation damage, and malignancy.[7] Perhaps the most important causes are iatrogenic, a not uncommon result of cancer therapeutics that entail regional lymph node dissection and irradiation. With regard to breast cancer alone, up to one-third of breast cancer survivors develop post-treatment lymphatic dysfunction.[108]
A number of homeostatic and pathological processes underlie the clinical picture of lymphedema. In the setting of osmotic and hydrostatic gradients maintained by the blood vasculature, disruption of lymphatic transport impairs the clearance of interstitial fluid and macromolecules. Stagnation of protein-rich lymph fluid within the local interstitium elevates tissue colloid pressure, thereby promoting further edematous fluid accumulation. Local ischemia ensues, and the affected tissues are primed for the persistent and progressive inflammatory changes that characterize chronic lymph insufficiency.[109] Hypercellularity of the lymphedematous tissue is primarily organized by fibroblasts, adipocytes, and keratinocytes, followed by infiltration of inflammatory cells, particularly polymorphonuclear neutrophils.[7,110,111] Macrophages and other mononuclear cells are recruited to the lymphedematous tissues, typifying an unrelenting inflammatory cascade that causes profound changes in dermal and subcutaneous architecture.[7,18,110–112] Subsequent tissue expansion and fibrotic changes, with matrix degeneration and concomitant adipose deposition, quickly ensue.[7] Gross tissue-level alterations present as chronic and debilitating swelling and pain of entire limbs, without a known cure or pharmacologic intervention.[7] The edema, initially pliable, with some lability, progresses to a rough and dense fibrotic mass of irreversible consequence.
Current treatments for lymphedema do not address the underlying pathophysiology and, thus, provide only modest delays in the establishment of end-stage sequelae, such as disfigurement and loss of function. Psychological distress often accompanies the physical features of lymphedema, further complicating management.[7,113–116] At present, the standard of care comprises compression therapy and manual massage to temporarily relieve the edema burden of affected limbs, but such physiotherapeutic intervention, while supportive, cannot prevent the natural progression of the disease.[7,107,117] The secondary development of co-morbidities, such as depression and chronic, recurring infection,[7] is common, underscoring the physiological importance of the lymphatic system; these complicating features must be actively recognized, diagnosed, and treated.
The biological attributes of experimentally induced lymphedema have been studied in the extremities and internal organs of various animals; until recently, the observations have been under-representative of our clinical understanding of lymphedema.[16,118–121] In animal models, ablation of the lymphatic vessels results in lymphedema amenable to therapeutic lymphangiogenesis; both direct administration of recombinant VEGF-C and plasmid-mediated gene therapy of VEGF-C demonstrated the ability to ameliorate the established pathology of acquired lymphedema.[70,122] Mouse models afford several advantages; in particular, the ready availability of tools to assess and manipulate murine genetics facilitates disease characterization with far greater clarity and power. Disruption of the lymphatic vasculature in a model of surgically induced lymph stasis of the murine tail displays marked acute inflammatory processes in the absence of a confounding inflammatory stimulus. Most recently, growth factor-mediated therapeutic lymphangiogenesis has been demonstrated in a murine tail model of acquired lymphedema.[122] Nevertheless, the hope for effective therapeutic lymphangiogenesis continues to inspire continued development for relevant models of acquired lymphatic insufficiency, notably towards reproducing the chronic state of the human disease.
5. Conclusions
The morphological, histochemical, and molecular changes observed in settings of lymphatic insufficiency have not, as yet, yielded a reliable circulating biomarker. Separation of the specific and direct tissue effects of lymph stasis from those resulting secondarily and indirectly must be accomplished. The expression of the anti-inflammatory cytokine interleukin-10, for example, is likely a physiological response to the inflammatory cascade initiated by lymph stasis, and not a part of the primary disease process. The role of wound repair mechanisms and activation of immune effectors is less certain and requires further experimentation to evaluate its relation to lymphatic vascular insufficiency. Microarray analysis of normal and lymphedematous animals reveals several hundred significant differences in gene expression which, when categorized by physiological function, include known pathways of acute inflammation, fibrosis, wound healing, angiogenesis, adipogenesis, activation of the Wnt pathway and complement system, cytoskeletal organization, and oxidative stress.[18] Certainly, the identification of these putative mediators requires further substantiation.
Recently characterized models of lymphatic development in the Xenopus laevis tadpole[123] and the zebra fish Danio rerio[124] may provide a means of efficiently screening candidates of functional and pathological importance. Insofar as the models may parallel the biology of human lymphedema, these investigative platforms afford the ability not only to identify the elements of disease development, but also to study the effects of putative pharmacotherapy to manipulate those mediators. In particular, the ability of therapeutic lymphangiogenesis with recombinant VEGF-C administration to surmount the pathological processes has been demonstrated recently.[122] The vascular endothelial growth factor receptor VEGFR3 and corresponding ligands, primarily VEGF-C, appear to be pivotal in both pathological and therapeutic pathways. Hence, the moderation of these factors may be instrumental in promoting homeostasis in the face of unremitting insult. The role of lymphangiogenesis in the setting of the inflammatory processes observed in acquired lymphedema, however, remains an area of investigation.
Although the proliferation of lymphatic vessels during inflammation was described very early,[125] the mechanism of this observation has only recently been studied. In the context of inflammation, VEGF-C expression is provided, at least in part, by macrophages which, when activated, secrete the growth factor alongside several other angiogenic and lymphangiogenic factors.[71,126] Inflammation induces the expression of VEGF-C and VEGFR3 in dendritic cells, possibly through the intermediary of pro-inflammatory cytokines.[127] Pro-inflammatory cytokines induce transcription of VEGF-C mRNA in tissue culture,[128] presumably through nuclear factor kappaB (NF-κB)-mediated promoter activation. These cytokines may, thus, help regulate lymphatic vessel growth during inflammatory challenge.[129] One such cytokine, tumor necrosis factor-α (TNFα) is particularly interesting in this regard. TNFα is expressed at sites of inflammation and is a known angiogenic factor, albeit indirectly[130] and, thus, may help bridge the simultaneous observation of inflammation and lymphangiogenesis in the setting of lymphatic insufficiency. Macrophages and dendritic cells observed histologically in animal models of lymphedema, while orchestrating the destructive acute inflammatory processes that belie the acute disease, may participate in repair mechanisms that while insufficient pathologically, represent an area of possible attenuation by targeted treatment. Suppression of the underlying derangement of innate immune function may, therefore, be an effective therapeutic strategy for acquired lymphedema, alone or in concert with pro-lymphangiogenic factors.
Analogous to proposed angiogenic treatment strategies for diseases of the peripheral and coronary blood vasculature, molecular approaches may ultimately provide a therapeutic window to reverse the pathology of both primary and secondary lymphatic insufficiency.[25,54,131–133] Initial experimental observations indicate that gene- and growth factor-mediated therapeutic lymphangiogenesis with VEGF-C holds promise for the treatment of lymphatic insufficiency, harnessing the regenerative capacity of the lymphatic vascular system.[25,28,70,122] Amelioration of other self-perpetuating components of the disease process, such as acute and chronic inflammation, may, however, also be necessary to attain complete amelioration of disease.
In summary, within the last decade, substantial advances have accrued in the identification of the processes that contribute to lymphatic vascular development in health and disease. The relationship of these processes to the identification and pathogenesis of heritable disorders of the lymphatic vasculature, acquired lymphatic vascular insufficiency, and the propagation of malignancy through lymphatic channels, suggests that much can be accomplished to mitigate the impact of disease. In all of these endeavors, the identification of biomarkers of the disease and its responsiveness to therapeutic intervention will represent a signal advance.
References
Beilhack A, Rockson SG. Immune traffic: a functional overview. Lymphat Res Biol 2003; 1(3): 219–34
Johnson LA, Clasper S, Holt AP, et al. An inflammation-induced mechanism for leukocyte transmigration across lymphatic vessel endothelium. J Exp Med 2006; 203(12): 2763–77
Saharinen P, Tammela T, Karkkainen MJ, et al. Lymphatic vasculature: development, molecular regulation and role in tumor metastasis and inflammation. Trends Immunol 2004; 25(7): 387–95
Gerli R, Solito R, Weber E, et al. Specific adhesion molecules bind anchoring filaments and endothelial cells in human skin initial lymphatics. Lymphology 2000; 33(4): 148–57
Ristevski B, Becker H, Cybulsky M, et al. Lymph, lymphocytes, and lymphatics. Immunol Res 2006; 35(1–2): 55–64
Harvey NL, Srinivasan RS, Dillard ME, et al. Lymphatic vascular defects promoted by Prox 1 haploinsufficiency cause adult-onset obesity. Nat Genet 2005; 37(10): 1072–81
Rockson SG. Lymphedema. Am J Med 2001; 110(4): 288–95
Stacker SA, Achen MG, Jussila L, et al. Lymphangiogenesis and cancer metastasis. Nat Rev Cancer 2002; 2(8): 573–83
Stacker SA, Baldwin ME, Achen MG. The role of tumor lymphangiogenesis in metastatic spread. FASEB J 2002; 16(9): 922–34
Schoppmann SF. Lymphangiogenesis, inflammation and metastasis. Anticancer Res 2005; 25(6C): 4503–11
Achen MG, Stacker SA. Tumor lymphangiogenesis and metastatic spread: new players begin to emerge. Int J Cancer 2006; 119(8): 1755–60
KriehuberE, Breiteneder-Geleff S, Groeger M, et al. Isolation and characterization of dermal lymphatic and blood endothelial cells reveal stable and functionally specialized cell lineages. J Exp Med 2001; 194(6): 797–808
Makinen T, Veikkola T, Mustjoki S, et al. Isolated lymphatic endothelial cells transduce growth, survival and migratory signals via the VEGF-C/D receptor VEGFR-3. EMBO J 2001; 20(17): 4762–73
Podgrabinska S, Braun P, Velasco P, et al. Molecular characterization of lymphatic endothelial cells. Proc Natl Acad Sci U S A 2002; 99: 16069–74
Hirakawa S, Hong YK, Harvey N, et al. Identification of vascular lineage-specific genes by transcriptional profiling of isolated blood vascular and lymphatic endothelial cells. Am J Pathol 2003; 162(2): 575–86
Shin WS, Szuba A, Rockson SG. Animal models for the study of lymphatic insufficiency. Lymphat Res Biol 2003; 1(2): 159–69
Karkkainen MJ, Ferrell RE, Lawrence EC, et al. Missense mutations interfere with VEGFR-3 signalling in primary lymphoedema. Nat Genet 2000; 25(2): 153–9
Tabibiazar R, Cheung L, Han J, et al. Inflammatory manifestations of experimental lymphatic insufficiency. PLoS Med 2006; 3(7): e254
Rutkowski JM, Moya M, Johannes J, et al. Secondary lymphedema in the mouse tail: lymphatic hyperplasia, VEGF-C upregulation, and the protective role of MMP-9. Microvasc Res 2006; 72(3): 161–71
Alitalo K, Tammela T, Petrova TV. Lymphangiogenesis in development and human disease. Nature 2005; 438(7070): 946–53
Ji RC. Lymphatic endothelial cells, tumor lymphangiogenesis and metastasis: new insights into intratumoral and peritumoral lymphatics. Cancer Metastasis Rev 2006 Dec; 25(4): 677–94
Ji RC. Characteristics of lymphatic endothelial cells in physiological and pathological conditions. Histol Histopathol 2005; 20(1): 155–75
Kato S, Shimoda H, Ji RC, et al. Lymphangiogenesis and expression of specific molecules as lymphatic endothelial cell markers. Anat Sci Int 2006; 81(2): 71–83
Cueni LN, Detmar M. New insights into the molecular control of the lymphatic vascular system and its role in disease. J Invest Dermatol 2006; 126(10): 2167–77
Tammela T, Saaristo A, Lohela M, et al. Angiopoietin-1 promotes lymphatic sprouting and hyperplasia. Blood 2005; 105(12): 4642–8
Sato TN, Tozawa Y, Deutsch U, et al. Angiopoietin-2 is required for postnatal angiogenesis and lymphatic patterning, and only the latter role is rescued by Angiopoietin-1. Dev Cell 2002; 3(3): 411–23
Makinen T, Adams RH, Bailey J, et al. PDZ interaction site in ephrinB2 is required for the remodeling of lymphatic vasculature. Genes Dev 2005; 19(3): 397–410
Kriederman BM, Myloyde TL, Witte MH, et al. FOXC2 haploinsufficient mice are a model for human autosomal dominant lymphedema-distichiasis syndrome. Hum Mol Genet 2003; 12(10): 1179–85
Petrova TV, Karpanen T, Norrmen C, et al. Defective valves and abnormal mural cell recruitment underlie lymphatic vascular failure in lymphedema distichiasis. Nat Med 2004 Sep; 10(9): 974–81
Kajiya K, Hirakawa S, Ma B, et al. Hepatocyte growth factor promotes lymphatic vessel formation and function. EMBO J 2005; 24: 2885–95
Huang XZ, Wu JF, Ferrando R, et al. Fatal bilateral chylothorax in mice lacking the integrin α9β1. Mol Cell Biol 2000; 20: 5208–15
Ayadi A, Zheng H, Sobieszczuk P, et al. Net-targeted mutant mice develop a vascular phenotype and up-regulate EGR-1. EMBO J 2001; 20: 5139–52
Yuan L, Moyon D, Pardanaud L, et al. Abnormal lymphatic vessel development in neuropilin 2 mutant mice. Development 2002; 129: 4797–806
Schacht V, Ramirez MI, Hong YK, et al. Tlalpha/podoplanin deficiency disrupts normal lymphatic vasculature formation and causes lymphedema. EMBO J 2003; 22: 3546–56
Wigle JT, Oliver G. Prox 1 function is required for the development of the murine lymphatic system. Cell 1999; 98(6): 769–78
Pennisi D, Gardner J, Chambers D, et al. Mutations in Sox18 underlie cardiovascular and hair follicle defects in ragged mice. Nat Genet 2000; 24: 434–7
Abtahian F, Guerriero A, Sebzda E, et al. Regulation of blood and lymphatic vascular separation by signaling proteins SLP-76 and Syk. Science 2003; 299: 247–51
Jeltsch M, Kaipainen A, Joukov V, et al. Hyperplasia of lymphatic vessels in VEGF-C transgenic mice. Science 1997; 276(5317): 1423–5
Karkkainen MJ, Haiko P, Sainio K, et al. Vascular endothelial growth factor C is required for sprouting of the first lymphatic vessels from embryonic veins. Nat Immunol 2004; 5: 74–80
Dumont DJ, Jussila L, Taipale J, et al. Cardiovascular failure in mouse embryos deficient in VEGF receptor-3. Science 1998; 282(5390): 946–9
Karkkainen MJ, Saaristo A, Jussila L, et al. A model for gene therapy of human hereditary lymphedema. Proc Natl Acad Sci U S A 2001; 98(22): 12677–82
Aselli G. De lactibus sive lacteis venis quarto vasorum mesaraicorum genere, novo invento Gaspariis Asellii Cremonensis anatomici Ticinensis dissertatio, quasententiae anatomicae multae, vel perperam receptae conuelluntur, vel parum perceptae illustrantur. Mediolani: apud Jo. Baptistam Bidellium, 1627
Sabin FR. On the origin of the lymphatic system from the veins and the development of the lymph hearts and thoracic duct in the pig. Am J Anat 1902; 1: 367–91
Oliver G. Lymphatic vasculature development. Nat Rev Immunol 2004; 4(1): 35–45
Petrova T, Makinen T, Makela T, et al. Lymphatic endothelial reprogramming of vascular endothelial cells by the Prox-1 homeobox transcription factor. EMBO J 2002; 16(9): 922–34
Jackson DG. Biology of the lymphatic marker LYVE-1 and applications in research into lymphatic trafficking and lymphangiogenesis. APMIS 2004; 112(7–8): 526–38
Banerji S, Ni J, Wang SX, et al. LYVE-1, a new homologue of the CD44 glycoprotein, is a lymph-specific receptor for hyaluronan. J Cell Biol 1999; 144(4): 789–801
Prevo R, Banerji S, Ferguson DJ, et al. Mouse LYVE-1 is an endocytic receptor for hyaluronan in lymphatic endothelium. J Biol Chem 2001; 276(22): 19420–30
Pure E, Cuff CA. A crucial role for CD44 in inflammation. Trends Mol Med 2001 May; 7(5): 213–21
Jackson DG, Prevo R, Clasper S, et al. LYVE-1, the lymphatic system and tumor lymphangiogenesis. Trends Immunol 2001; 22(6): 317–21
Gale NW, Prevo R, Espinosa J, et al. Normal lymphatic development and function in mice deficient for the lymphatic hyaluronan receptor LYVE-1. Mol Cell Biol 2007; 27(2): 595–604
Mouta Carreira C, Nasser SM, di Tomaso E, et al. LYVE-1 is not restricted to the lymph vessels: expression in normal liver blood sinusoids and down-regulation in human liver cancer and cirrhosis. Cancer Res 2001; 61(22): 8079–84
Oliver G, Detmar M. The rediscovery of the lymphatic system: old and new insights into the development and biological function of the lymphatic vasculature. Genes Dev 2002; 16(7): 773–83
Ferrara N, Alitalo K. Clinical applications of angiogenic growth factors and their inhibitors. Nat Med 1999; 5(12): 1359–64
Carmeliet P. Mechanisms of angiogenesis and arteriogenesis. Nat Med 2000; 6(4): 389–95
Veikkola T, Karkkainen M, Claesson-Welsh L, et al. Regulation of angiogenesis via vascular endothelial growth factor receptors. Cancer Res 2000; 60(2): 203–12
Kaipainen A, Korhonen J, Mustonen T, et al. Expression of the fms-like tyrosine kinase 4 gene becomes restricted to lymphatic endothelium during development. Proc Natl Acad Sci U S A 1995; 92(8): 3566–70
Joukov V, Pajusola K, Kaipainen A, et al. A novel vascular endothelial growth factor, VEGF-C, is a ligand for the Flt4 (VEGFR-3) and KDR (VEGFR-2) receptor tyrosine kinases. EMBO J 1996; 15(7): 1751
Achen MG, Jeltsch M, Kukk E, et al. Vascular endothelial growth factor D (VEGF-D) is a ligand for the tyrosine kinases VEGF receptor 2 (Flk1) and VEGF receptor 3 (Flt4). Proc Natl Acad Sci U S A 1998; 95(2): 548–53
Partanen TA, Arola J, Saaristo A, et al. VEGF-C and VEGF-D expression in neuroendocrine cells and their receptor, VEGFR-3, in fenestrated blood vessels in human tissues. FASEB J 2000; 14(13): 2087–96
Luttun A, Tjwa M, Carmeliet P. Placental growth factor (P1GF) and its receptor Flt1 (VEGFR-1): novel therapeutic targets for angiogenic disorders. Ann N Y Acad Sci 2002; 979: 80–93
Suto K, Yamazaki Y, Morita T, et al. Crystal structures of novel vascular endothelial growth factors (VEGF) from snake venoms: insight into selective VEGF binding to kinase insert domain-containing receptor but not to fms-like tyrosine kinase-1. J Biol Chem 2005; 280(3): 2126–31
Jussila L, Alitalo K. Vascular growth factors and lymphangiogenesis. Physiol Rev 2002; 82(3): 673–700
Wigle JT, Harvey N, Detmar M, et al. An essential role for Prox1 in the induction of the lymphatic endothelial cell phenotype. EMBO J 2002; 21(7): 1505–13
Paavonen K, Puolakkainen P, Jussila L, et al. Vascular endothelial growth factor receptor-3 in lymphangiogenesis in wound healing. Am J Pathol 2000; 156(5): 1499–504
Kaipainen A, Korhonen J, Pajusola K, et al. The related FLT4, FLT1, and KDR receptor tyrosine kinases show distinct expression patterns in human fetal endothelial cells. J Exp Med 1993; 178(6): 2077–88
Oh SJ, Jeltsch MM, Birkenhager R, et al. VEGF and VEGF-C: specific induction of angiogenesis and lymphangiogenesis in the differentiated avian chorioallantoic membrane. Dev Biol 1997; 188(1): 96–109
Enholm B, Karpanen T, Jeltsch M, et al. Adenoviral expression of vascular endothelial growth factor-C induces lymphangiogenesis in the skin. Circ Res 2001; 88(6): 623–9
Saaristo A, Veikkola T, Tammela T, et al. Lymphangiogenic gene therapy with minimal blood vascular side effects. J Exp Med 2002; 196: 719–30
Szuba A, Skobe M, Karkkainen MJ, et al. Therapeutic lymphangiogenesis with human recombinant VEGF-C. FASEB J 2002; 16(14): 1985–7
Skobe M, Hawighorst T, Jackson DG, et al. Induction of tumor lymphangiogenesis by VEGF-C promotes breast cancer metastasis. Nat Med 2001; 7(2): 192–8
Maisonpierre PC, Suri C, Jones PF, et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science 1997; 277(5322): 55–60
Sato TN, Tozawa Y, Deutsch U, et al. Distinct roles of the receptor tyrosine kinases Tie-1 and Tie-2 in blood vessel formation. Nature 1995; 376(6535): 70–4
Suri C, Jones PF, Patan S, et al. Requisite role of angiopoietin-1, a ligand for the TIE2 receptor, during embryonic angiogenesis. Cell 1996; 87(7): 1171–80
Gale N, Thurston G, Hackett S, et al. Angiopoietin-2 is required for postnatal angiogenesis and lymphatic patterning, and only the latter role is rescued by angiopoietin-1. Dev Cell 2002; 3: 411–23
Weninger W, Partanen TA, Breiteneder-Geleff S, et al. Expression of vascular endothelial growth factor receptor-3 and podoplanin suggests a lymphatic endothelial cell origin of Kaposi’s sarcoma tumor cells. Lab Invest 1999; 79(2): 243–51
Breiteneder-Geleff S, Soleiman A, Kowalski H, et al. Angiosarcomas express mixed endothelial phenotypes of blood and lymphatic capillaries: podoplanin as a specific marker for lymphatic endothelium. Am J Pathol 1999; 154(2): 385–94
Oliver G, Harvey N. A stepwise model of the development of lymphatic vasculature. Ann N Y Acad Sci 2002; 979: 159–65
Hong Y, Harvey N, Noh Y, et al. Prox1 is a master control gene in the program specifying lymphatic endothelial cell fate. Dev Dyn 2002; 225: 351–7
Chen H, Chedotal A, He Z, et al. Neuropilin-2, a novel member of the neuropilin family, is a high affinity receptor for the semaphorins Sema E and Sema IV but not Sema III. Neuron 1997; 19(3): 547–59
Soker S, Takashima S, Miao HQ, et al. Neuropilin-1 is expressed by endothelial and tumor cells as an isoform-specific receptor for vascular endothelial growth factor. Cell 1998; 92(6): 735–45
Grainger RM. Embryonic lens induction: shedding light on vertebrate tissue determination. Trends Genet 1992; 8(10): 349–55
van der Putte SC. The early development of the lymphatic system in mouse embryos. Acta Morphol Neer1 Scand 1975 Dec; 13(4): 245–86
Kunstfeld R, Hirakawa S, Hong YK, et al. Induction of cutaneous delayed-type hypersensitivity reactions in VEGF-A transgenic mice results in chronic skin inflammation associated with persistent lymphatic hyperplasia. Blood 2004; 104(4): 1048–57
Mandriota SJ, Jussila L, Jeltsch M, et al. Vascular endothelial growth factor-C-mediated lymphangiogenesis promotes tumour metastasis. EMBO J 2001; 20(4): 672–82
Stacker SA, Caesar C, Baldwin ME, et al. VEGF-D promotes the metastatic spread of tumor cells via the lymphatics. Nat Med 2001; 7(2): 186–91
He Y, Kozaki K, Karpanen T, et al. Suppression of tumor lymphangiogenesis and lymph node metastasis by blocking vascular endothelial growth factor receptor 3 signaling. J Natl Cancer Inst 2002; 94(11): 819–25
Makinen T, Jussila L, Veikkola T, et al. Inhibition of lymphangiogenesis with resulting lymphedema in transgenic mice expressing soluble VEGF receptor-3. Nat Med 2001; 7(2): 199–205
Van Trappen PO, Steele D, Lowe DG, et al. Expression of vascular endothelial growth factor (VEGF)-C and VEGF-D, and their receptor VEGFR-3, during different stages of cervical carcinogenesis. J Pathol 2003; 201(4): 544–54
Zeng Y, Opeskin K, Baldwin ME, et al. Expression of vascular endothelial growth factor receptor-3 by lymphatic endothelial cells is associated with lymph node metastasis in prostate cancer. Clin Cancer Res 2004; 10(15): 5137–44
Clarijs R, Schalkwijk L, Hofmann UB, et al. Induction of vascular endothelial growth factor receptor-3 expression on tumor microvasculature as a new progression marker in human cutaneous melanoma. Cancer Res 2002; 62(23): 7059–65
Shields JD, Borsetti M, Rigby H, et al. Lymphatic density and metastatic spread in human malignant melanoma. Br J Cancer 2004; 90(3): 693–700
Dadras SS, Lange-Asschenfeldt B, Velasco P, et al. Tumor lymphangiogenesis predicts melanoma metastasis to sentinel lymph nodes. Mod Pathol 2005; 18(9): 1232–42
Pepper MS, Tille JC, Nisato R, et al. Lymphangiogenesis and tumor metastasis. Cell Tissue Res 2003; 4(1): 167
He Y, Rajantie I, Unionen M, et al. Preexisting lymphatic endothelium but not endothelial progenitor cells are essential for tumor lymphangiogenesis and lymphatic metastasis. Cancer Res 2004; 64(11): 3737–40
Hirakawa S, Kodama S, Kunstfeld R, et al. VEGF-A induces tumor and sentinel lymph node lymphangiogenesis and promotes lymphatic metastasis. J Exp Med 2005; 201(7): 1089–99
Hirakawa S, Brown LF, Kodama S, et al. VEGF-C-induced lymphangiogenesis in sentinel lymph nodes promotes tumor metastasis to distant sites. Blood 2007; 109(3): 1010–7
Asahara T, Murohara T, Sullivan A, et al. Isolation of putative progenitor endothelial cells for angiogenesis. Science 1997; 275(5302): 964–7
Shi Q, Rafii S, Wu MH, et al. Evidence for circulating bone marrow-derived endothelial cells. Blood 1998; 92(2): 362–7
Kerjaschki D, Huttary N, Raab I, et al. Lymphatic endothelial progenitor cells contribute to de novo lymphangiogenesis in human renal transplants. Nat Med 2006; 12(2): 230–4
Schledzewski K, Falkowski M, Moldenhauer G, et al. Lymphatic endotheliumspecific hyaluronan receptor LYVE-1 is expressed by stabilin-l+, F4/80+, CD11b+ macrophages in malignant tumours and wound healing tissue in vivo and in bone marrow cultures in vitro: implications for the assessment of lymphangiogenesis. J Pathol 2006; 209(1): 67–77
Meige H. Dystophie oedematoeuse hereditaire. Presse Med 1898; 6: 341–3
Milroy W. An undescribed variety of hereditary oedema. NY Med J 1892; 56: 505–8
Ferrell RE, Levinson KG, Esman JH, et al. Hereditary lymphedema: evidence for linkage and genetic heterogeneity. Hum Mol Genet 1998; 7(13): 2073–8
Irrthum A, Devriendt K, Chitayat D, et al. Mutations in the transcription factor gene SOX18 underlie recessive and dominant forms of hypotrichosis-lymphedema-telangiectasia. Am J Hum Genet 2003; 72(6): 1470–8
Fang J, Dagenais SL, Erickson RP, et al. Mutations in FOXC2 (MFH-1), a forkhead family transcription factor, are responsible for the hereditary lymphedema-distichiasis syndrome. Am J Hum Genet 2000; 67(6): 1382–8
Szuba A, Rockson SG. Lymphedema: classification, diagnosis and therapy. Vasc Med 1998; 3(2): 145–56
Olszewski WL, Engeset A, Romaniuk A, et al. Endothelial reprogramming of vascular endothelial cells by the Prox-1 homeobox. Lymphology 1990; 23(1): 23–33
Piller NB. Lymphedema, macrophages and benzopyrones. Lymphology 1980; 13: 109–19
Piller NB. Macrophage and tissue changes in the developmental phases of secondary lymphoedema and during conservative therapy with benzopyrone. Arch Histol Cytol 1990; 53: 209–18
Schirger A, Harrison EG, Janes JM. Idiopathic lymphedema: review of 131 cases. JAMA 1962; 182: 124–32
Maunsell E, Brisson J, Deschenes L. Arm problems and psychological distress after surgery for breast cancer. Can J Surg 1993; 36(4): 315–20
Passik SD, McDonald MV. Psychosocial aspects of upper extremity lymphedema in women treated for breast carcinoma. Cancer 1998; 83 (12 Suppl. American): 2817–20
Velanovich V, Szymanski W. Quality of life of breast cancer patients with lymphedema. Am J Surg 1999; 177(3): 184–7
Rockson SG. Addressing the unmet needs in lymphedema risk management. Lymphat Res Biol 2006 Spring; 4(1): 42–6
Rockson SG, Miller LT, Senie R, et al. American Cancer Society Lymphedema Workshop. Workgroup III: diagnosis and management of lymphedema. Cancer 1998; 83 (12 Suppl. American): 2882–5
Clodius L, Kohnlein H, Piller NB. Chronic limb lymphoedema produced solely by blocking the lymphatics in the subcutaneous compartment. Br J Plast Surg 1977; 30(2): 156–60
Casley-Smith JR, Clodius L, Foldi-Borcsok E, et al. The effects of chronic cervical lymphostasis on regions drained by lymphatics and by prelymphatics. J Pathol 1978; 124(1): 13–7
Foldi M. Anatomical and physiological basis for physical therapy of lymphedema. Experientia 1978; 33 Suppl.: 15–8
Olszewski WL. The treatment of lymphedema of the extremities with microsurgical lympho-venous anastomoses. Int Angiol 1988; 7(4): 312–21
Yoon YS, Murayama T, Gravereaux E, et al. VEGF-C gene therapy augments postnatal lymphangiogenesis and ameliorates secondary lymphedema. J Clin Invest 2003; 111(5): 717–25
Cheung L, Han J, Beilhack A, et al. An experimental model for the study of lymphedema and its response to therapeutic lymphangiogenesis. Biodrugs 2006; 20(6): 363–70
Ny A, Koch M, Schneider M, et al. A genetic Xenopus laevis tadpole model to study lymphangiogenesis. Nat Med 2005; 11(9): 998–1004
Kuchler AM, Gjini E, Peterson-Maduro J, et al. Development of the zebrafish lymphatic system requires VEGFC signaling. Curr Biol 2006; 16(12): 1244–8
Pullinger D, Florey H. Proliferation of lymphatics in inflammation. J Pathol Bacteriol 1937; 45: 157–70
Schoppmann SF, Birner P, Stockl J, et al. Tumor-associated macrophages express lymphatic endothelial growth factors and are related to peritumoral lymphangiogenesis. Am J Path 2002; 161: 947–56
Hamrah P, Chen L, Zhang Q, et al. Novel expression of vascular endothelial growth factor receptor (VEGFR)-3 and VEGF-C on corneal dendritic cells. Am J Pathol 2003; 163(1): 57–68
Ristimaki A, Narko K, Enholm B, et al. Proinflammatory cytokines regulate expression of the lymphatic endothelial mitogen vascular endothelial growth factor-C. J Biol Chem 1998; 273(14): 8413–8
Mouta C, Heroult M. Inflammatory triggers of lymphangiogenesis. Lymphat Res Biol 2003; 1(3): 201–18
Jackson JR, Seed MP, Kircher CH, et al. The codependence of angiogenesis and chronic inflammation. FASEB J 1997; 11(6): 457–65
Baumgartner I, Pieczek A, Manor O, et al. Constitutive expression of phVEGF165 after intramuscular gene transfer promotes collateral vessel development in patients with critical limb ischemia [see comments]. Circulation 1998; 97(12): 1114–23
Rivard A, Isner JM. Angiogenesis and vasculogenesis in treatment of cardiovascular disease. Mol Med 1998; 4(7): 429–40
An A, Rockson SG. The potential for molecular treatment strategies in lymphatic disease. Lymphat Res Biol 2004; 2(4): 173–81
Acknowledgments
No sources of funding were used to assist in the preparation of this review. The authors have no conflicts of interest that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nakamura, K., Rockson, S.G. Biomarkers of Lymphatic Function and Disease. Mol Diag Ther 11, 227–238 (2007). https://doi.org/10.1007/BF03256244
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03256244