
Abstract
Purpose
To understand clinicians’ perceptions regarding practice guidelines in Canadian intensive care units (ICUs) to inform guideline development and implementation strategies.
Methods
We developed a self-administered survey instrument and assessed its clinical sensibility and reliability. The survey was mailed to ICU physicians and nurses in Canada to determine local ICU guideline development and use, and to compare physicians’ and nurses’ attitudes and preferences towards guidelines.
Results
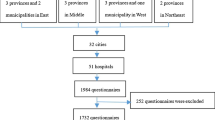
The survey was completed by 51.6% (565/1095) of potential respondents. Although less than half reported a formal guideline development committee in their ICU, 81.0% reported that guidelines were developed at their institutions. Of clinicians who used guidelines in the ICU, 70.2% of nurses and 42.6% of physicians reported using them frequently or always. Professional society guidelines (with or without local modification) were reportedly used in most ICUs, but physicians were more confident than nurses of their validity (P < 0.001). Physicians considered endorsement of guidelines by a colleague more relevant for enhancing guideline use than did nurses (P < 0.001). Nurses considered low risk of the guideline and whether the guideline is consistent with their practice (P < 0.001) to be more relevant to guideline uptake than did physicians (P < 0.001). Lack of agreement with recommendations was a more important barrier to use of guidelines for physicians than for nurses (P < 0.001).
Conclusions
Many Canadian institutions locally develop guidelines, and many ICU physicians and nurses report using them. Planning implementation strategies according to clinician preferences may increase guideline use. The nature of the differences in attitudes towards guidelines between nurses and physicians, and their impact on clinician adherence to guidelines requires further exploration.
Résumé
Objectif
Comprendre les perceptions des cliniciens quant aux guides de pratique dans les unités de soins intensifs afin d’améliorer le développement de directives et la mise en œuvre de stratégies.
Méthode
Nous avons développé un sondage auto-administré et avons évalué sa sensibilité et sa fiabilité cliniques. Le formulaire de sondage a été envoyé à des intensivistes et des infirmiers/infirmières au Canada afin de déterminer l’utilisation et le développement local de guides de pratique dans les unités de soins intensifs, et de comparer les attitudes et préférences des médecins et des infirmiers/infirmières quant aux guides de pratique.
Résultats
Le questionnaire a été rempli par 51,6 % (565/1095) des répondants potentiels. Bien que moins de la moitié aient fait état d’un comité officiel de développement d’un guide de pratique dans leur unité de soins intensifs, 81,0% rapportent que certains guides ont été développés dans leur institution. Parmi les cliniciens utilisant des guides de pratique aux soins intensifs, 70,2 % des infirmiers/infirmières et 42,6 % des médecins ont répondu les utiliser fréquemment ou toujours. Les guides de pratique de sociétés professionnelles (avec ou sans modification locale) sont, selon le sondage, utilisés dans la plupart des unités de soins intensifs, mais les médecins ont montré plus de confiance dans leur validité que les infirmiers/infirmières (P < 0,001). Les médecins ont considéré la reconnaissance du guide de pratique par un collègue comme plus influente vis-à-vis de l’observance d’un guide de pratique que les infirmiers/infirmières (P < 0,001). Les infirmiers/infirmières ont considéré qu’un guide de pratique au risque réduit et sa cohérence avec la pratique quotidienne (P < 0,001) étaient plus pertinents à l’adoption d’un guide de pratique que les médecins (P < 0,001). Le désaccord concernant les recommandations a constitué une barrière plus importante à la mise en pratique d’un guide pour les médecins que pour les infirmiers/infirmières (P < 0,001).
Conclusion
De nombreuses institutions canadiennes développent des guides de pratique localement, et de nombreux médecins et infirmiers/infirmières des soins intensifs rapportent leur utilisation. La planification de stratégies de mise en œuvre selon les préférences des cliniciens pourrait accro ître l’utilisation des directives. La nature des différences quant aux guides par les infirmiers/infirmières et les médecins, ainsi que leur impact sur l’observance en clinique des guides, nécessitent des études approfondies.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Pilon CS, Leathley M, London R, et al. Practice guideline for arterial blood gas measurement in the intensive care unit decreases numbers and increases appropriateness of tests. Crit Care Med 1997; 25:1308–13.
Pitimana-aree S, Forrest D, Brown G, Anis A Wang XH Dodek Pl. Implementation of a clinical practice guideline for stress ulcer prophylaxis increases appropriateness and decreases cost of care. Intensive Care Med 1998; 24:217–23.
McMullin J, Cook D, Griffith L, et al. Minimizing errors of omission: behavioural reenforcement of heparin to avert venous emboli: the BEHAVE study. Crit Care Med 2006; 34:694–9.
Baxter AD, Allan J, BedardJ, et al. Adherence to simple and effective measure reduces the incidence of ventilator-associated pneumonia. Can J Anesth 2005; 52:535–41.
Mascia MF, Koch M, Medicis JJ. Pharmacoeconomic impact of rational use guidelines on the provision of analgesia, sedation, and neuromuscular blockade in critical care. Crit Care Med 2000; 28:2300–6.
Brattebo G, Hofoss D, Flaatten H, Muri AK, Gjerde S,Plsek Effect of a scoring system and protocol for sedation on duration of patients’ need for ventilator support in a surgical intensive care unit. BMJ 2002; 324:1386–9.
Merlani P, Garnerin P, Diby M, Ferring M, Ricou Quality improvement report: linking guideline to regular feedback to increase appropriate requests for clinical tests: blood gas analysis in intensive care. BMJ 2001; 323:620–4.
Jain MK, Heyland DK, Dhaliwal R, et al. Dissemination of the Canadian clinical practice guidelines for nutrition support: results of a cluster randomized. controlled trial. Crit Care Med 2006; 34:2362–9.
Dodek P, Keenan S, Cook D, et al.; Canadian Critical Car Trials Group; Canadian Critical Care Society. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med 2004; 141:305–13.
Hayward RS, Guyatt GH, Moore KA, McKibbon KA,Carter Canadian physicians’ attitudes about and preferences regarding clinical practice guidelines. CMAJ 1997; 156:1715–23.
Hayward RS, Wilson MC, Tunis SR, Guyatt GH, Moore KA, Bass EB. Practice guidelines. What are we looking for? J Gen Intern Med 1996; 11:176–8.
Tunis SR, Hayward RS, Wilson MC, et al. Internists’ attitudes about clinical practice guidelines. Ann Intern Med 1994; 120:956–63.
Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999; 282:1458–65.
SinuffT, Kahnamoui K, Cook DJ, Giacomini M.Practice guidelines as multipurpose tools: a qualitative study of noninvasive ventilation. Crit Care Med 2007; 35:776–82.
Cook DJ, Meade MO, Hand LE, McMullin JP. Toward understanding evidence uptake: Semirecumbency for pneumonia prevention. Crit Care Med 2002; 30:1472–7.
FleissJL, Cohen J. The equivalence of weighted kappa and the intraclass correlation coefficient as measures of reliability. Educational and Psychological Measurement 1973; 33:613–9.
Kleinbaum DG, Kupper LL, Muller KE, Nizam A. Applied regression analysis and other multivariable methods. Toronto, Duxbury Press; 1998:118–85.
Atkins D, BestD, BrissPA, et al.; GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004; 328:1490.
Choudhry NK, Stelfox HT, Detsky AS. Relationships between authors of clinical practice guidelines and the pharmaceutical industry. JAMA 2002; 87:612–7.
Eichacker PQ, Natanson C, Danner RL. Surviving sepsis — practice guidelines, marketing campaigns, and Eli Lilly. N Engl J Med 2006; 355:1640–2.
Wachter RM. Expected and unanticipated consequences of the quality and information technology revolutions. JAMA 2006; 295:2780–3.
Streiner DL, Norman GR. Biases in Responding, Health Measurement Scales. New York, Oxford University Press; 2003: 80–101.
Feinstein AR, Josephy BR, Wells CK. Scientific and clinical problems in indexes of functional disability. Ann Intern Med 1986; 105:413–20.
Feinstein AR, Wells CK, Joyce CM, Josephy BR. The evaluation of sensibility and the role of patient collaboration in clinimetric indexes. Trans Assoc Am Physicians 1985; 98:146–9.
Cook DJ, Guyatt GH, Jaeschke R, et al. Determinants in Canadian health care workers of the decision to withdraw life support from the critically ill. Canadian Critical Care Trials Group. JAMA 1995; 273:703–8.
Aday LA. Designing and Conducting Health Surveys. San Francisco, Jossey Bass Publishers; 1989.
Zucker AR, Meadow WL. Pediatric critical care physicians’ attitudes about guidelines for the use of ribavirin in critically ill children with respiratory syncytial virus pneumonia. Crit Care Med 1995; 23: 767–72.
Author information
Authors and Affiliations
Corresponding author
Additional information
This survey was supported by the Canadian Critical Care Society and the Canadian Association of Critical Care Nurses. Sources of financial support: Hamilton Health Sciences New Investigator Fund. Dr Sinuff is supported by a Canadian Institutes for Health Research Clinician Scientist Award. Dr Cook is a Research Chair of the Canadian Institutes for Health Research.
No author has a financial relationship with a commercial entity that has an interest in the subject of this manuscript.
Rights and permissions
About this article
Cite this article
Sinuff, T., Eva, K.W., Meade, M. et al. Clinical practice guidelines in the intensive care unit: a survey of Canadian clinicians’ attitudes. Can J Anesth 54, 728–736 (2007). https://doi.org/10.1007/BF03026869
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03026869