
Abstract
Purpose
To determine if deliberate hypotension decreases blood loss and transfusion requirements in patients undergoing orthopedic surgery, a systematic review of all randomized trials addressing this issue was undertaken.
Methods
Electronic databases, citations lists and review articles were searched for potential articles. Relevant articles met the following inclusion criteria: English language, humans undergoing orthopedic surgery, deliberate hypotension used by any method, intraoperative blood loss measured as an outcome, and the trial methodology being randomized and controlled. Four outcomes were analyzed, including estimated blood loss, blood transfused, surgery duration, and quality of the surgical field. For all analyses, the random-effects model was used.
Results
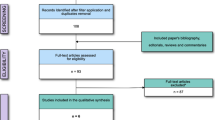
Seventeen articles met the inclusion criteria. The surgeries studied included total hip arthroplasty (seven), orthog-nathic surgery (eight), total knee arthroplasty (one) and spinal fusion (one). A total of 636 patients were randomized across all studies. For blood loss, the overall weighted mean difference favoured treatment, with a savings of about 287 mL of blood [95% confidence interval (CI): -447, -127]. The mean differences also showed a statistically significant benefit for deliberate hypotension in reducing transfusion requirements (-667 mL of blood transfused; 95% CI: -963, -370). Deliberate hypotension was not shown to reduce the duration of surgery (-1.9 min of surgery; 95% CI: -7.2, 3.5) or improve surgical conditions (surgical field quality rating -0.5; 95% CI: -1.1, 0.2).
Conclusion
This review provides some support for the use of deliberate hypotension in reducing blood loss and transfusion requirements in orthopedic surgery, but these results are tempered by the small sample sizes and poor methodological quality of published studies.
Résumé
Objectif
Afin de déterminer si l’hypotension délibérée réduit les pertes sanguines et l’incidence transfusionnelle chez les patients subissant une chirurgie orthopédique, un compte-rendu systéma-tique de toutes les études randomisées traitant de cette question a été entrepris.
Méthode
Les bases de données électroniques, listes de citations et articles de compte-rendu ont été consultés afin de trouver des articles potentiellement pertinents. Les articles pertinents ont répondu aux critères suivants: langue anglaise, êtres humains subissant une chirurgie orthopédique, utilisation d’une méthode d’hypotension délibérée, quelle qu’elle soit, pertes sanguines pero-pératoires mesurées en tant que résultat, et méthodologie d’étude randomisée et contrôlée. Quatre évolutions ont été analysées, notamment les pertes sanguines estimées, le sang transfusé, la durée de la chirurgie et la qualité de l’hémostase chirurgicale. Un modèle à effets aléatoires a été utilisé pour toutes les analyses.
Résultats
Dix-sept articles ont répondu aux critères d’inclusion. Les chirurgies évaluées comprenaient: arthroplasties totales de la hanche (sept), chirurgies orthognathes (huit), arthroplastie totale du genou (une) et spondylodèse (une). Un total de 636 patients ont été randomisés dans ces études. En ce qui a trait à la perte sanguine, la différence moyenne pondérée totale a montré un résultat en faveur du traitement, avec une diminution des pertes sanguines d’environ 287 mL [95 % intervalle de confiance (IC) : 447, -127]. Les différences moyennes ont également montré que l’hypotension délibérée présente des bienfaits statistiquement si-gnificatifs dans la réduction de l’incidence transfusionnelle (-667 mL de sang transfusé; 95 % IC: -963, -370). L’hypotension délibérée n’a pas eu d’influence sur la durée de chirurgie (-1,9 min de chirurgie; 95 % IC: -7,2, 3,5) ou sur l’ amélioration des conditions chirurgicales (évaluation de la qualité de l’hémostase chirurgicale -0,5 ;95%IC:-1,1, 0,2).
Conclusion
Ce compte-rendu soutient dans une certaine mesure l’utilisation de l’hypotension délibérée pour réduire les pertes sanguines et l’incidence transfusionnelle lors de chirurgie ortho-pédique; toutefois, ces résultats sont mitigés par les petites tailles d’échantillons et la pauvreté méthodologique des études publiées.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Sollevi A. Hypotensive anesthesia and blood loss. Acta Anaesthesiol Scand Suppl 1988; 89:39–43.
Lawson NW, Thompson DS, Nelson CL, Flacke JW, North ER. Sodium nitroprusside-induced hypotension for supine total hip replacement. Anesth Analg 1976; 55:654–62.
Safar P. A study of deliberate hypotension in anesthesia, with special consideration of surgical blood loss in comparable groups of normotensive and hypotensive anesthesia. Surgery 1955; 37:1002–18.
Little DM. Induced hypotension during anesthesia and surgery. Anesthesiology 1955; 16:320–32.
Eckenhoff JE. Deliberate hypotension. Anesthesiology 1978; 48:87–8.
Hampton LJ, Little DM. Complications associated with the use of controlled hypotension in anesthesia. AMA Arch Surg 1953; 67:549–56.
Dolman RM, Bentley KC, Head TW, English M. The effect of hypotensive anesthesia on blood loss and operative time during Le Forte I osteotomies. J Oral Maxillofac Surg 2000; 58:834–9.
Larson AG. Deliberate hypotension. Anesthesiology 1964; 25:682–706.
Ditzler JW, Eckenhoff JE. A comparison of blood loss and operative time in certain surgical procedures completed with and without controlled hypotension. Ann Surg 1956; 143:289–93.
Van Aken H, Miller ED Jr. Deliberate hypotension.In: Miller RD (Ed.). Anesthesia, 5th ed. NY: Churchill Livingston; 2000: 1470–90.
Rohling R, Zimmermann AP, Biro P, Haers PE, Sailer HF. Alternative methods for reduction of blood loss during elective orthognathic surgery. Int J Adult Orthodon Orthognath Surg 1999; 14:77–82.
Enlund MG, Ahlstedt BL, Andersson LG, Krekmanov LI. Induced hypotension may influence blood loss in orthognathic surgery, but it is not crucial. Scand J Plast Reconstr Surg Hand Surg 1997; 31:311–7.
Shapira Y, Gurman G, Artru AA, et al. Combined hemodilution and hypotension monitored with jugular bulb oxygen saturation, EEC, and ECG decreases transfusion volume and length of ICU stay for major orthopedic surgery. J Clin Anesth 1997; 9:643–9.
Hartmann T, Winkler M, Preis C, Germann P, Donner A, Muller C. Critical evaluation of blood-saving measures for high-risk patients. Acta Anaesthesiol Scand Suppl 1997; 111:207–9.
Precious DS, Splinter W, Bosco D. Induced hypotensive anesthesia for adolescent orthognathic surgery patients. J Oral Maxillofac Surg 1996; 54:680–3.
Hack H, Mitchell V. Hypotensive anaesthesia. Br J Hosp Med 1996; 55:482–5.
Gombotz H, Stubenvoll E. Avoiding homologous blood and blood products in the perisurgical setting. Acta Anaesthesiol Scand Suppl 1996; 109:138–9.
Schindler I, Andel H, Leber J, Kimla T. Moderate induced hypotension provides satisfactory operating conditions in maxillofacial surgery. Acta Anaesthesiol Scand 1994; 38:384–7.
Sharrock NE, Mineo R, Urquhart B, Salvati EA. The effect of two levels of hypotension on intraoperative blood loss during total hip arthroplasty performed under lumbar epidural anesthesia. Anesth Analg 1993; 76:580–4.
Tate DE, Friedman RJ. Blood conservation in spinal surgery. Review of current techniques. Spine 1992; 17:1450–6.
Blau WS, Kafer ER, Anderson JA. Esmolol is more effective than sodium nitroprusside in reducing blood loss during orthognathic surgery. Anesth Analg 1992; 75:172–8.
An HS, Mikhail WE, Jackson WT, Tolin B, Dodd GA. Effects of hypotensive anesthesia, nonsteroidal antiinflammatory drugs, and polymethylmethacry-late on bleeding in total hip arthroplasty patients. J Arthroplasty 1991; 6:245–50.
Goldberg ME, McNulty SE, Azad SS, et al. A comparison of labetalol and nitroprusside for inducing hypotension during major surgery. Anesth Analg 1990; 70:537–42.
Fahmy NR, Bottros MR, Charchaflieh J, Matta EB, Sunder N. A randomized comparison of labetalol and nitroprusside for induced hypotension. J Clin Anesth 1989; 1:409–13.
Porter SS, Asher M, Fox DK. Comparison of intravenous nitriprusside, nitroprusside-captopril, and nitro-glycerin for deliberate hypotension during posterior spine fusion in adults. J Clin Anesth 1988; 1:87–95.
Simpson DL, MacRae WR, Wildsmith JA, Dale BA. Acute beta-adrenoreceptor blockade and induced hypotension. Anaesthesia 1987; 42:243–8.
Gallagher DM, Milliken RA. Induced hypotension for orthognathic surgery. J Oral Surg 1979; 37:47–51.
Mostarlic O, Reiger V, Lazarevic Z. Controlled hypo tension induced by sodium nitroprusside. A practical approach. Acta Anaesthesiol Belg 1976; 27 Suppl:55–66.
Phillips W, Hensinger RN. Control of blood loss during scoliosis surgery. Clin Orthop Relat Res 1988; 229:88–93.
Bunker JP. Anesthetic effects on surgical blood loss. Ann NY Acad Sci 1964; 115:418–21.
Anderson JA. Deliberate hypotensive anesthesia for orthognatic surgery: controlled pharmacological manipulation of cardiovascular physiology. Int J Adult Orthodon Orthognath Surg 1986; 1:133–59.
Sharrock NE, Salvati EA. Hypotensive epidural anesthesia for total hip arthroplasty: a review. Acta Orthop Scand 1996; 67:91–107.
Fahmy NM. Indications and contraindications for deliberate hypotension with a review of of its cardiovascular effects. Int Anesthesiol Clin 1979; 17:175–87.
Kashimoto S, Nakamura T, Yamaguchi T. Prostoglandin E1 reduces blood loss during and after resection of lumbar herniated disc. J Anesth 1992; 6:294–6.
Oxman AD, Guyatt GH. Guidelines for reading literature reviews. CMAJ 1988; 138:697–703.
Haynes RB, Wilczynski N, McKibbon KA, Walker CJ, Sinclair JC. Developing optimal search strategies for detecting clinically sound studies in MEDLINE. J Am Med Infrom Assoc 1994; 1:447–58.
Jadad AM, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996; 17:1–12.
Sackett DL, Haynes RB, Tugwell P, Guyatt G. Clinical Epidemiology: A Basic Science for Clinical Medicine, 2nd ed. Lippincott Williams & Wilkins; 1991.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986; 7:177–88.
Barbier-Bohm G, Desmonts JM, Couderc E, Moulin D, Prokocimer P, Oliver H. Comparative effects of induced hypotension and normovolaemic haemodilution on blood loss in total hip arthroplasty. Br J Anaesth 1980; 52:1039–43.
Chan W, Smith DE, Warer WH. Effects of hypotensive anesthesia in anterior maxillary osteotomy. J Oral Surg 1980; 38:504–8.
Felfernig-Bœhm D, Salat A, Kinstner C, et al. Influence of hypotensive and normotensive anesthesia on platelet aggregability and hemostatic markers in orthognathic surgery. Thromb Res 2001; 103:185–92.
Fromme GA, MacKenzie RA, Gould AB, Lund BA, Offord KP. Controlled hypotension of orthognathic surgery. Anesth Analg 1986; 65:683–6.
Fukusaki M, Maekawa T, Yamaguchi K, Matsumoto M, Shibata O, Sumikawa K. Combined effects of prolonged prostaglandin E1-induced hypotension and haemodilution on human hepatic function. Eur J Anaesthesiol 1997; 14:157–63.
Grundy BL, Nash CL, Brown RH. Deliberate hypotension for spinal fusion: prospective randomized study with evoked potential monitoring. Can Anaesth Soc J 1982; 29:452–62.
Juelsgaard P, Larsen UT, Sorensen JV, Madsen F, Soballe K. Hypotensive epidural anethesia in total knee replacement without tourniquet: reduced blood loss and transfusion. Reg Anesth Pain Med 2001; 26:105–10.
Lessard MR, Trepanier CA, Baribault JP. Isoflurane-induced hypotension in orthognathic surgery. Anesth Analg 1989; 69:379–83.
Niemi TT, Pitkanen M, Syrjala M, Rosenberg PH. Comparison of hypotensive epidural anaesthesia and spinal anaesthesia on blood loss and coagulation during and after total hip arthroplasty. Acta Anaesthesiol Scand 2000; 44:457–64.
Praveen K, Narayanan V, Muthusekhar MR, Baig MF. Hypotensive anaesthesia and blood loss in orthognathic surgery: a clinical study. Br J Oral Maxillofac Surg 2001; 39:138–40.
Qvist TF, Skovsted P, Bredgaard Sorensen M. Moderate hypotensive anaesthesia for reduction of blood loss during total hip replacement. Acta Anaesthesiol Scand 1982; 26:351–3.
Rosberg B, Fredin H, Gustafson C. Anesthetic techniques and surgical blood loss in total hip arthroplasty. Acta Anaesthesiol Scand 1982; 26:189–93.
Thompson GE, Miller RD, Stevens WC, Murray WR. Hypotensive anesthesia for total hip arthroplasty: a study of blood loss and organ function (brain, heart, liver and kidney). Anesthesiology 1978; 48:91–6.
Yukioka H, Asada K, Fujimori M, Shimazu A. Prostoglandin E1 as a hypotensive drug during general anesthesia for total hip replacement. J Clin Anesth 1993; 5:310–4.
Oxman AD, Cook DJ, Guyatt GH. User’s guides to the medical literature. VI. How to use an overview. Evidenced-Based Medical Working Group. JAMA 1994; 272:1367–71.
Pogue J, Yusuf S. Overcoming the limitations of current meta-analysis of randomised controlled trials. Lancet 1998; 351:47–52.
Thornton A, Lee P. Publication bias in meta-analysis: its causes and consequences. J Clin Epidemiol 2000; 53:207–16.
American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Anesthesiology 2006; 105:198–208.
Enderby GE. A report on mortality and morbidity following 9,107 hypotensive anaesthetics. Br J Anaesth 1961; 33:109–13.
Arbous MS, Grobbee DE, van Kleef JW, et al. Mortality associated with anaesthesia: a qualitative analysis to identify risk factors. Anaesthesia 2001; 56:1141–53.
Kawashima Y, Takahashi S, Suzuki M, et al. Anesthesia-related mortality and morbidity over a 5-year period in 2,363,038 patients in Japan. Acta Anaesthesiol Scand 2003; 47:809–17.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial support: Hamilton Health Sciences, Department of Anesthesia Academic Fund.
Rights and permissions
About this article
Cite this article
Paul, J.E., Ling, E., Lalonde, C. et al. Deliberate hypotension in orthopedic surgery reduces blood loss and transfusion requirements: A meta-analysis of randomized controlled trials. Can J Anesth 54, 799–810 (2007). https://doi.org/10.1007/BF03021707
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021707