
Abstract
Background: The Bonfils intubation fibrescope (BIF), a rigid, straight and reusable fibreoptic device, is being used increasingly to facilitate endotracheal intubation after direct laryngoscopy has failed. We tested the hypothesis that, with the BIF compared to direct laryngoscopy, the rate of failed endotracheal intubation could be reduced in patients with a difficult airway, simulated by means of a rigid cervical immobilization collar.
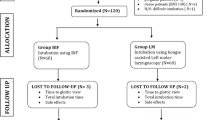
Methods: Seventy-six adults undergoing elective gynecological surgery under general anesthesia were randomly assigned to have endotracheal intubation, facilitated with either a standard size 3 Macintosh laryngoscope blade, or the BIF. A rigid cervical immobilization collar was used to simulate a difficult airway, by reducing mouth opening and limiting neck extension. If endotracheal intubation could not be achieved within two attempts, the cervical collar was removed, and direct laryngoscopy was performed thereafter, using a Macintosh blade in all subjects. The success rate of endotracheal tube placement was the primary outcome variable.
Results: Patient characteristics were similar in the two groups. After neck immobilization, the inter-incisor distance was reduced to 2.6±0.7 cm (Macintosh) and 2.6±0.8 cm (BIF). Tube placement was successful in 15/38 (39.5%) patients with a Macintosh blade, and in 31/38 patients with the BIF (81.6%;P=0.0003). Time required for tube placement was 53±22 sec (Macintosh) and 64±24 sec (BIF;P=0.15). Conclusion: The Bonfils intubation fibrescope is a more effective intubating device for patients with immobilized cervical spine and significantly limited inter-incisor distance, when compared to direct laryngoscopy.
Résumé
Contexte: Le fibroscope d’intubation Bonfils (BIF) est un appareil fibroscopique rigide, droit et réutilisable qui est de plus en plus utilisé pour faciliter l’intubation endotrachéale lors de l’échec d’une laryngoscopie directe. Nous avons testé l’hypothèse que lorsque le BIF est comparé à la laryngoscopie directe, le taux d’échec de l’intubation endotrachéale pouvait tre réduit chez des patients présentant des voies aériennes difficiles, lesquelles ont été simulées gr?ce à un collier d’immobilisation cervicale rigide.
Méthode: Soixante-seize adultes devant subir une chirurgie gynécologique programmée sous anesthésie générale ont été randomisées à recevoir une intubation endotrachéale, facilitée soit par une lame de laryngoscope Macintosh de taille standard 3 ou par le BIF. Un collier d’immobilisation cervicale rigide a été placé pour simuler des voies aériennes difficiles en réduisant l’ouverture de la bouche et en limitant l’extension du cou. Si l’intubation trachéale ne réussissait pas après deux essais, le collier cervical était retiré et une laryngoscopie directe réalisée ensuite à l’aide d’une lame Macintosh chez toutes les patientes. Le critère d’efficacité principal était le taux de positionnement correct de la sonde endotrachéale.
Résultats: Les caractéristiques des patientes étaient similaires dans les deux groupes. Après immobilisation du cou, l’espace entre les incisives a été réduit à 2,6±0,7 cm (Macintosh) et 2,6±0,8 cm (BIF). La sonde a été placée correctement chez 15/38 (39,5%) patientes avec une lame Macintosh et chez 31/38 patientes avec le BIF (81,6%; P=0,0003). Le temps requis pour le positionnement de la sonde était de 53±22 sec (Macintosh) et 64±24 sec (BIF; P=0,15).
Conclusion: Comparé à la laryngoscopie directe, le fibroscope d’intubation Bonfils est un appareil d’intubation plus efficace pour les patients ayant la colonne cervicale immobilisée et un espace entre les incisives considérablement limité.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2003; 98: 1269–77.
Brain AI, Verghese C, Addy EV, Kapila A, Brimacombe J. The intubating laryngeal mask. II: A preliminary clinical report of a new means of intubating the trachea. Br J Anaesth 1997; 79: 704–9.
Huang WT, Huang CY, Chung YT. Clinical comparisons between GlideScope video laryngoscope and Trachlight in simulated cervical spine instability. J Clin Anesth 2007; 19: 110–4.
Agro F, Barzoi G, Mantecchia F. Tracheal intubation using a Macintosh laryngoscope or a GlideScope in 15 patients with cervical spine immobilization. Br J Anaesth 2003; 90: 705–6.
Bonfils P. Difficult intubation in Pierre-Robin children, a new method: the retromolar route (German). Anaesthesist 1983; 32: 363–7.
Bein B, Yan M, Tonner PH, Scholz J, Steinfath M, Dorges V. Tracheal intubation using the Bonfils intubation fibrescope after failed direct laryngoscopy. Anaesthesia 2004; 59: 1207–9.
Bein B, Worthmann F, Scholz J, et al. A comparison of the intubating laryngeal mask airway and the Bonfils intubation fibrescope in patients with predicted difficult airways. Anaesthesia 2004; 59: 668–74.
Langeron O, Masso E, Huraux C, et al. Prediction of difficult mask ventilation. Anesthesiology 2000; 92:1229–36.
Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984; 39: 1105–11.
Yentis SM, Lee DJ. Evaluation of an improved scoring system for the grading of direct laryngoscopy. Anaesthesia 1998; 53: 1041–4.
Bellhouse CP, Dore C. Criteria for estimating likelihood of difficulty of endotracheal intubation with the Macintosh laryngoscope. Anaesth Intensive Care 1988;16: 329–37.
Heath KJ. The effect on laryngoscopy of different cervical spine immobilisation techniques. Anaesthesia 1994; 49: 843–5.
Laurent SC, de Melo AE, Alexander-Williams JM. The use of the McCoy laryngoscope in patients with simulated cervical spine injuries. Anaesthesia 1996; 51:74–5.
Smith CE, Pinchak AB, Sidhu TS, Radesic BP, Pinchak AC, Hagen JF. Evaluation of tracheal intubation difficulty in patients with cervical spine immobilization: fiberoptic (WuScope) versus conventional laryngoscopy. Anesthesiology 1999; 91: 1253–9.
Wakeling HG, Nightingale J. The intubating laryngeal mask airway does not facilitate tracheal intubation in the presence of a neck collar in simulated trauma. Br J Anaesth 2000; 84: 254–6.
Komatsu R, Nagata O, Kamata K, Yamagata K, Sessler DI, Ozaki M. Intubating laryngeal mask airway allows tracheal intubation when the cervical spine is immobilized by a rigid collar. Br J Anaesth 2004; 93:655–9.
Author information
Authors and Affiliations
Corresponding author
Additional information
Conflict of interest: The Bonfils intubation fibrescopes were provided on a complimentary basis by Karl Storz GmbH and Co. KG, Tuttlingen, Germany. There were no other sources of funding. None of the authors has any conflicts of interest related to the products and/or companies mentioned in the manuscript.
Rights and permissions
About this article
Cite this article
Byhahn, C., Nemetz, S., Breitkreutz, R. et al. Brief report: Tracheal intubation using the Bonfils intubation fibrescope or direct laryngoscopy for patients with a simulated difficult airway. Can J Anesth 55, 232–237 (2008). https://doi.org/10.1007/BF03021507
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021507