
Abstract
Purpose
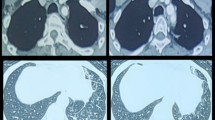
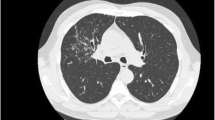
To report acute upper airway obstruction due to cricoarytenoid arthritis, a well known but uncommon complication of rheumatoid arthritis.
Clinical features
We report the case of a 70-yr-old female scheduled for a colostomy who had been suffering from rheumatoid arthritis for 17 years. Preoperative history and physical examination revealed no cardiopulmonary compromise. Anesthesia was induced while an assistant immobilized the cervical spine and an atraumatic intubation was performed. Surgery was uneventful. Muscle paralysis was reversed, demonstrated by normalization of the train-of-four response, and the patient was extubated awake. Shortly postextubation, the patient developed inspiratory stridor, which disappeared after a second dose of neostigmine. The patient was transported to the postanesthesia care unit. Just prior to arrival the patient once again developed inspiratory stridor, became distressed, and oxygen saturation decreased. Direct laryngoscopy followed by a nasal fibreoptic examination of the larynx was performed. Cricoarytenoid arthritis secondary to rheumatoid arthritis with airway compromise was diagnosed. An uneventful awake tracheostomy was performed. The patient was discharged on day ten with a colostomy and a tracheostomy in place. One month postdischarge the patient’s trachea was decannulated. On follow-up, a normal voice and mobile cords were observed.
Conclusion
Cricoarytenoid arthritis is an infrequent complication of rheumatoid arthritis. Athorough history and physical examination are necessary to recognize signs and symptoms of cricoarytenoid arthritis. Prompt recognition of airway obstruction due to cricoarytenoid arthritis is essential for appropriate management.
Résumé
Objectif
Présenter un cas d’obstruction des voies respiratoires supérieures provoquée par l’arthrite crico-aryténoïdienne, une complication rare, mais bien connue, de l’arthrite rhumatoïde.
Éléments cliniques
Il s’agit d’une femme de 70 ans, souffrant d’arthrite rhumatoïde depuis 17ans, qui devait subir une colostomie. Lanamnèse préopératoire et l’examen physique n’ont révélé aucune atteinte cardiopulmonaire. Lanesthésie a été induite pendant l’immobilisation de la colonne cervicale par un assistant, puis l’intubation atraumatique a été réalisée, L’intervention chirurgicale s’est bien déroulée. La paralysie musculaire a été renversée, prouvée par la normalisation de la réponse en trainde-quatre, et l’extubation vigile a été pratiquée. Peu après, un stridor s’est développé et a disparu à la suite d’une seconde dose de néostigmine. La patiente a été transportée à la salle de réveil. Juste avant l’arrivée, le stridor est apparu de nouveau, accompagné de détresse et d’une baisse de la saturation en oxygène. On a procédé à une laryngoscope directe suivie d’un examen fibroscopique nasal du larynx. Larthrite cricoaryténoïdienne secondaire à l’arthrite rhumatoïde, avec obstruction des voies respiratoires, a été diagnostiquée. Une trachéotomie vigile a été faite, sans incident. La patiente a quitté l’hôpital au dixième jour avec une colostomie et une trachéostomie en place. La canule trachéale a été enlevée un mois après. La voix était normale et les cordes vocales mobiles lors du suivi.
Conclusion
L’arthrite cricoaryténoïdienne est une complication rare de l’arthrite rhumatoïde. Une anamnèse fouillée et un examen minutieux sont nécessaires pour en reconnaître les signes et les symptômes. Le diagnostic rapide d’obstruction des voies aériennes causée par l’arthrite cricoaryténoïdienne est essentiel au traitement approprié.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Brazeau-Lamontagne L, Charlin B, Levesque RY, Lussier A. Cricoarytenoiditis: CT assessment in rheumatoid arthritis. Radiology 1986; 158: 463–6.
Skues MA, Welchew EA. Anaesthesia and rheumatoid arthritis. Anaesthesia 1993; 48: 989–97.
Jenkins LC, McGraw RW. Anaesthetic management of the patient with rheumatoid arthritis. Can Anaesth Soc J 1969; 16: 407–15.
Matti MV, Sharrock NE. Anesthesia on the rheumatoid patient. Rheum Dis Clin North Am 1998; 24: 19–34.
Phelps JA. Laryngeal obstruction due to cricoarytenoid arthritis. Anesthesiology 1966; 27: 518–22.
Kandora TF, Gilmore IM, Sorber JA, Kose FB, Matta II. Cricoarytenoid arthritis presenting as cardiopulmonary arrest. Ann Emerg Med 1985; 14: 700–2.
Bamshad M, Rosa U, Padda G, Luce M. Acute upper airway obstruction in rheumatoid arthritis of the cricoarytenoid joints. South Med J 1989; 82: 507–11.
Lofgren RH, Montgomery WW. Incidence of laryngeal involvement in rheumatoid arthritis. N Engl J Med 1962; 267: 193–5.
Bienenstock H, Ehrlich GE, Freyberg RH. Rheumatoid arthritis of the cricoarytenoid joint: a clinicopathologic study. Arthritis Rheum 1963; 6: 48–63.
Polisar IA. The crico-arytenoid joint: a diarthrodial articulation subject to rheumatoid arthritic involvement. Laryngoscope 1959; 69: 1129–64.
Grossman A, Martin JR, Root HS. Rheumatoid arthritis of the crico-arytenoid joint. Laryngoscope 1961; 71: 530–44.
Montgomery WW. Cricoarytenoid arthritis. Laryngoscope 1963; 73: 801–36.
Sellars I, Sellars S. Cricoarytenoid joint structure and function. J Laryngol Otol 1983; 97: 1027–34.
von Leden H, Moore P. The mechanics of the cricoarytenoid joint. Arch Otolaryngol 1961; 73: 63–72.
Bridger MWM, Jahn AF, van Nostrand AWP. Laryngeal rheumatoid arthritis. Laryngoscope 1980; 90: 296–303.
Woldorf NM, Pastore PN, Terz J. Rheumatoid arthritis of the cricoarytenoid joint. Arch Otolaryngol 1971; 93: 623–7.
Leicht MJ, Harrington TM, Davis DE. Cricoarytenoid arthritis: a cause of larygneal obstruction. Ann Emerg Med 1987; 16: 885–8.
Lynch JP III, Quint LE. Tracheobronchial and esophageal manifestations of systemic diseases.In: Cummings CW (Ed.). Otolaryngology Head and Neck Surgery, 3rd ed. Missouri: Mosby-Year Book, Inc., 1998: 2343–67.
Jurik AG, Pedersen U. Rheumatoid arthritis of the crico-arytenoid and crico-thyroid joints: a radiological and clinical study. Clin Radiol 1984; 35: 233–6.
Funk D, Raymon F. Rheumatoid arthritis of the cricoarytenoid joints: an airway hazard. Anesth Analg 1975; 54: 742–5.
Gardner DL, Holmes F. Anaesthetic and postoperative hazards in rheumatoid arthritis. Br J Anaesth 1961; 33: 258–64.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kolman, J., Morris, I. Cricoarytenoid arthritis: a cause of acute upper airway obstruction in rheumatoid arthritis. Can J Anesth 49, 729–732 (2002). https://doi.org/10.1007/BF03017454
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03017454