
Abstract
Purpose
This study assessed difficult airway management, training and equipment availability among Canadian anesthesiologists.
Methods
A postal survey of active members of the Canadian Anesthesiologists’ Society was conducted in 2000. Respondents chose an induction condition and intubation technique for each often difficult airway scenarios. Availability of airway devices in their workplaces was assessed. Chi square analyses were used to compare groups. A P value of < 0.05 was considered statistically significant.
Results
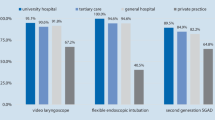
Eight hundred and thirty-three of 1702 (49%) surveys were returned. Staff comprised 88%, and residents 12%. Fifty-five percent had attended a difficult airway workshop within five years and 30% received mannequin airway training during residency. Direct laryngoscopy (48%) or fibreoptic bronchoscopy (34%) were the preferred techniques for intubation. For laryngeal, subglottic and unstable cervical spine scenarios, awake intubation with fibreoptic bronchoscope was most widely chosen. Asleep intubation with direct laryngoscopy was most commonly selected for trauma scenarios. Availability of difficult airway equipment varied between regions and types of hospital. Cricothyroidotomy equipment and difficult airway carts were not universally available.
Conclusions
Our survey assessed current preferences, training and equipment availability for the difficult airway amongst Canadian anesthesiologists. Direct laryngoscopy and fibreoptic bronchoscopy were the preferred technique for intubation despite widespread availability of newer airway equipment. Lack of certain essential airway equipment and difficult airway training should be addressed.
Résumé
Objectif
Évaluer la gestion de l’intubation difficile, la formation et la disponibilité du matériel auprès des anesthésiologistes canadiens.
Méthode
Une enquête postale a été réalisée en 2000 auprès des membres actifs de la Société canadienne des anesthésiologistes. Les répondants ont choisi une condition d’induction et une technique d’intubation pour chacun des dix scénarios d’intubation difficile présentés. La disponibilité des instruments d’intubation dans leur milieu de travail a été évaluée. Des analyses du khi carré ont été utilisées pour comparer les groupes. Une valeur de P < 0,05 a été considérée comme significative.
Résultats
Huit cent trente-trois des 1702 formulaires ont été renvoyés. On comptait 88 % de spécialistes et 12 % de résidents. Cinquante-cinq pour cent avaient assisté à un atelier sur l’intubation difficile pendant les cinq dernières années et 30 % avaient reçu une formation avec un mannequin pendant la résidence. La laryngoscopie directe (48) ou la fibroscopie bronchique (34 %) ont été préférées. Lintubation vigile avec un fibroscope bronchique a été largement choisie pour des scénarios laryngés, sous-glottique et d’instabilité de la colonne cervicale. L’intubation sous anesthésie générale avec une laryngoscope directe a été couramment sélectionnée pour les traumatismes. La disponibilité du matériel pour l’intubation difficile variait selon les régions et les types d’hôpitaux. Le matériel de cricothyroïdotomie et les chariots pour intubation difficile n’étaient pas disponibles partout.
Conclusion
Notre enquête a évalué les préférences des anesthésiologistes canadiens, la formation et la disponibilité du matériel concernant l’intubation difficile. La laryngoscope directe et la fibroscopie bronchique ont été les techniques préférées malgré la disponibilité répandue de nouveau matériel d’intubation. Il faudrait pallier les lacunes d’un certain matériel essentiel et de la formation à l’intubation difficile.
Article PDF
Similar content being viewed by others
Avoid common mistakes on your manuscript.
References
Caplan RA, Benumof JL, Berry FA, et al. Practice guidelines for management of the difficult airway. A report by the American Society of Anesthesiologists Task Force on management of the difficult airway. Anesthesiology 1993; 78: 597–602.
Benumof JL. Laryngeal mask airway and the ASA difficult airway algorithm. Anesthesiology 1996; 84: 686–99.
Rosenblatt WH, Wagner PJ, Ovassapian A, Kain ZN. Practice patterns in managing the difficult airway by anesthesiologists in the United States. Anesth Analg 1998; 87: 153–7.
Crosby ET, Cooper RM, Douglas MJ, et al. The unanticipated difficult airway with recommendations for management. Can J Anaesth 1998; 45: 757–76.
Rose DK, Cohen MM. The airway: problems and predictions in 18,500 patients. Can J Anaesth 1994; 41: 372–83.
Finucane B. The difficult airway — a Canadian perspective (Editorial). Can J Anaesth 1998; 45: 713–8.
Koppel JN, Reed AP. Formal instruction in difficult airway management. A survey of anesthesiology residency programs. Anesthesiology 1995; 83: 1343–6.
Slotnick HB. How doctors learn: physicians’ self-directed learning episodes. Acad Med 1999; 74: 1106–7.
Davis D, O’Brien MAT, Freemantle N, Wolf FM, Mazmanian P, Taylor-Vaisey A. Impact of formal continuing medical education. Do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes? JAMA 1999; 282: 867–74.
McGuire GP, Wong DT. Airway management: contents of a difficult intubation cart. Can J Anesth 1999; 46: 190–1.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was supported in part by the Department of Anesthesia, Toronto Western Hospital, University of Toronto and Vitaid Inc., Toronto, Ontario, Canada.
An erratum to this article is available at http://dx.doi.org/10.1007/BF03018663.
Rights and permissions
About this article
Cite this article
Jenkins, K., Wong, D.T. & Correa, R. Management choices for the difficult airway by anesthesiologists in Canada. Can J Anesth 49, 850–856 (2002). https://doi.org/10.1007/BF03017419
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03017419