
Abstract
Purpose
Our objective was to demonstrate that preemptive vessel dilator cricothyrotomy may be useful when managing the patient with airway obstruction.
Methods
An Institutional Review Board approved retrospective study was undertaken in 88 patients for whom this technique was selected. The anesthesiologists and surgeons identified as authors were directly involved in the care of these patients. All vessel dilator cricothyrotomies were performed in the operating rooms of University Hospital, UAB, Medical Center. The patients selected for this airway management technique were afflicted with some type of supraglottic lesion, usually squamous cell carcinoma, which was obstructing their airways to an extent that complete airway obstruction during induction of anesthesia was a significant possibility.
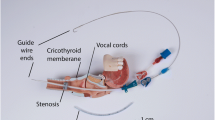
Prior to induction of anesthesia, the vessel dilator was inserted into the tracheal lumen through the cricothyroid membrane as described. Oxygenation was maintained with jet ventilation from a Sanders jetting device. Age, sex, weight, initial and lowest O2 saturation, first recorded ETCO2, blood pressure and duration of jet ventilation were recorded.
Results
The airways were successfully managed in all 88 patients with this technique. There were no deaths, and no postoperative hypoxic sequelae; also complications were minor.
Conclusion
Vessel dilator cricothyrotomy as a preemptive procedure in the management of patients with significant supraglottic airway obstruction may be a useful addition to the anesthesiologists’ armamentarium of airway management devices.
Résumé
Objectif
Démontrer que la crico-thyrotomie préventive avec un dilatateur vasculaire peut aider la prise en charge ďune obstruction des voies respiratoires.
Méthode
Le comité ďexamen a approuvé notre étude rétrospective auprès de 88 patients soumis à cette technique. Les anesthésiologistes et les chirurgiens, auteurs du présent article, ont été directement appelés à participer. Toutes les crico-thyrotomies avec dilatateur vasculaire ont été réalisées dans les salles ďopération du University Hospital, UAB, Medical Center. Les patients choisis présentaient une lésion oropharyngée, habituellement un épithéliome malpighien, qui obstruait les voies respiratoires de façon tellement étendue qu’une obstruction complète des voies aériennes était à craindre pendant ľinduction de ľanesthésie. Avant ľinduction, le dilatateur vasculaire a été inséré dans la lumière de la trachée par la membrane cricotyroïdienne. ľoxygénation a été maintenue avec la ventilation en jet par un appareil à jet Sanders. ľâge, le poids, la saturation initiale en O2 et la plus faible saturation, la première ETCO2 enregistrée, la tension artérielle et la durée de la ventilation en jet ont été notés.
Résultats
Les voies aériennes ont été bien protégées chez tous les patients. Il n’y a pas eu de décès ni de séquelles hypoxiques postopératoires, seulement des complications mineures.
Conclusion
La crico-thyrotomie avec dilatateur vasculaire, utilisée comme technique préventive chez des patients qui présentent une obstruction oropharyngée, peut s’ajouter avantageusement aux appareils de prise en charge des voies aériennes par les anesthésiologistes.
Article PDF
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
References
Caplan RA, Benumof JL, Berry FA, et al. Practice guidelines for management of the difficult airway. An updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2003; 98: 1269–77.
Gillespie MB, Eisele DW. Outcomes of emergency surgical airway procedures in a hospital-wide setting. Laryngoscope 1999; 109: 1766–9.
Yarrington CT, Fraser JP. Complications of tracheotomy. Arch Surg 1965; 91: 652–5.
Boyce JR, Peters G. Vessel dilator cricothyrotomy for transtracheal jet ventilation. Can J Anaesth 1989; 36: 350–3.
Lang SA, Duncan PG, Shephard DA, Ha HC. Pulmonary oedema associated with airway obstruction. Can J Anaesth 1990; 37: 210–8.
Caplan RA, Posner KL, Ward RJ, Cheney FW. Adverse respiratory events in anesthesia: a closed claims analysis. Anesthesiology 1990; 72: 828–33.
Schwartz DE, Matthay MA, Cohen NH. Death and other complications of emergency airway management in critically ill adults. Anesthesiology 1995; 82: 367–76.
Simoni P, Peters GE, Magnuson JS, Carroll WR. Use of the endoscopic microdebrider in the management of airway obstruction from laryngotracheal carcinoma. Ann Otol Rhinol Laryngol 2003; 112: 11–3.
Jacoby JJ, Hamelberg W, Ziegler CH, Flory FA, Jones JR. Transtracheal resuscitation. JAMA 1956; 162: 625–8.
Porter Reed J, Kemph JP, Hamelberg W, Hitchcock FA, Jacoby J. Studies with transtracheal artificial respiration. Anesthesiology 1954; 153: 28–41.
Carden E, Becker G, Hamood H. Percutaneous jet ventilation. Ann Otol Rhinol Laryngol 1976; 85: 652–5.
Weymuller EA, Pavlin EG, Paugh D, Cummings CW. Management of difficult airway problems with percuta neous transtracheal ventilation. Ann Otol Rhinol Laryngol 1987; 96: 34–7.
Spoerel WE, Narayanan PS, Singh NP. Transtracheal ventilation. Br J Anaesth 1971; 43: 932–40.
Wong DT, McGuire GP. Subcutaneous emphysema following trans-cricothyroid membrane injection of local anesthetic. Can J Anesth 2000; 47: 165–8.
Benumof JL, Scheller MS. The importance of transtracheal jet ventilation in the management of the difficult airway. Anesthesiology 1989; 71: 769–78.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boyce, J.R., Peters, G.E., Carroll, W.R. et al. Preemptive vessel dilator cricothyrotomy aids in the management of upper airway obstruction. Can J Anesth 52, 765–769 (2005). https://doi.org/10.1007/BF03016567
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016567