
Abstract
Background
Acute renal failure (ARF) occurs in up to 10% of critically ill patients, with significant associated morbidity and mortality. The optimal mode of renal replacement therapy (RRT) remains controversial. This retrospective study compared continuous renal replacement therapy (CRRT) and intermittent hemodialysis (IHD) for RRT in terms of intensive care unit (ICU) and hospital mortality, and renal recovery.
Methods
We reviewed the records of all patients undergoing RRT for the treatment of ARF over a 12-month period. Patients were compared according to mode of RRT, demographics, physiologic characteristics, and outcomes of ICU and hospital mortality and renal recovery using the Chi square, Student’s t test, and multiple logistic regression as appropriate.
Results
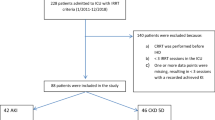
I 16 patients with renal insufficiency underwent RRT during the study period. Of these, 93 had ARF. The severity of illness of CRRT patients was similar to that of IHD patients using APACHE II (25.1 vs 23.5, P = 0.37), but they required significantly more intensive nursing (therapeutic intervention scale 47.8 vs 37.6, P = 0.0001 ). Mortality was associated with lower pH at presentation (P = 0.003) and increasing age (P = 0.03). Renal recovery was significantly more frequent among patients initially treated with CRRT (21/24 vs 5/14, P = 0.0003). Further investigation to define optimal timing, dose, and duration of RRT may be beneficial.
Conclusions
Although further study is needed, this study suggests that renal recovery may be better after CRRT than IHD for ARF. Mortality was not affected significantly by RRT mode.
Résumé
Objectif
L’insuffisance rénale aigu ë (IRA) se manifeste chez près de 10 % des grands malades, avec une morbidité et une mortalité accentuées. Le mode optimal de thérapie continue de remplacement rénal (TCRR) reste controversé. Notre étude rétrospective a comparé la TCRR et l’hémodialyse intermittente (HDI) en termes de morbidité et de mortalité à l’unité des soins intensifs (USI) et à l’hôpital de même que la récupération rénale.
Méthode
Pour notre étude rétrospective, nous examiné les dossiers de tous les patients traités par TCRR pour l’IRA au cours de 12 mois. Nous avons comparé les patients selon le mode de TCRR, les caractéristiques démographiques et physiologiques, l’évolution à l’USI, la mortalité à l’hôpital et la récupération rénale en utilisant le test du chi deux et le test t de Student et une régression logistique multiple selon le cas.
Résultats
Pendant la période étudiée, 116 patients atteints d’insuffisance rénale, dont 93 avaient une IRA, ont reçu une TCRR. La sévérité de la maladie des patients sous TCRR était comparable à celle des patients sous HDI d’après le score APACHE II (25,1 vs 23,5, P = 0,37), mais nécessitait des soins infirmiers significativement plus intensifs (échelle d’intervention thérapeutique 47,8 vs 37,6, P = 0,0001). La mortalité était plus fréquente avec un pH plus bas au moment de l’admission (P = 0,003) et avec l’âge (P = 0,03). La récupération rénale était significativement plus fréquente chez les patients traités initialement avec une TCRR (21/24 vs 5/14, P = 0,0003). Une recherche plus poussée visant à définir le moment optimal, la dose et la duré de la TCRR est souhaitable.
Conclusion
La présente recherche indique que la récupération peut être meilleure après une TCRR qu’une HDI pour l’IRA. Le mode de TCRR ne modifie pas significativement la mortalité.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Levy EM, Viscoli CM, Horwitz RI. The effect of acute renal failure on mortality. A cohort analysis. JAMA 1996; 275:1489–94.
Chertow GM, Christiansen CL, Cleary PD, Munro C, Lazarus JM. Prognostic stratification in critically ill patients with acute renal failure requiring dialysis. Arch Intern Med 1995; 155:1505–11.
Liano F, Pascual J. Epidemiology of acute renal failure: a prospective, multicenter, community-based study. Madrid Acute Renal Failure Study Group. Kidney Int 1996; 50:811–8.
Brivet FG, Kleinknecht DJ, Loirat P, Landais PJ. Acute renal failure in intensive care units — causes, outcome, and prognostic factors of hospital mortality: a prospective, multicenter study. French Study Group on Acute Renal Failure. Crit Care Med 1996; 24:192–8.
Silvester W, Bellomo R, Cole L. Epidemiology, management, and outcome of severe acute renal failure of critical illness in Australia. Crit Care Med 2001; 29:1910–5.
Metnitz PG, Krenn CG, Steltzer H, et al. Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit Care Med 2002; 30:2051–8.
Kelleher SP, Robinette JB, Miller F, Conger JD. Effect of hemorrhagic reduction in blood pressure on recovery from acute renal failure. Kidney Int 1987; 31:725–30.
Conger JD, Robinette JB, Hammond WS. Differences in vascular reactivity in models of ischemic acute renal failure. Kidney Int 1991; 39:1087–97.
Kramer P, Kaufhold G, Grone HJ, et al. Management of anuric intensive-care patients with arteriovenous hemofiltration. Int J Artif Organs 1980; 3:225–30.
Davenport A, Will EJ, Davidson AM. Improved cardiovascular stability during continuous modes of renal replacement therapy in critically ill patients with acute hepatic and renal failure. Crit Care Med 1993; 21:328–38.
van Bommel EF,Bouvy ND, So KL, et al. Acute dialytic support for the critically ill: intermittent hemodialysis versus continuous arteriovenous hemodiafiltration. Am J Nephrol 1995; 15:192–200.
Cosentino F, Chaff C, Piedmonte M. Risk factors influencing survival in ICU acute renal failure. Nephrol Dial Transplant 1994; 9(Suppl IV):179–82.
Bellomo R, Parkin G, Love J, Boyce N. A prospective comparative study of continuous arteriovenous hemodiafiltration and continuous venovenous hemodiafiltration in critically ill patients. Am J Kidney Dis 1993; 21:400–4.
Bellomo R, Mansfield D, Rumble S, Shapiro J, Parkin G, Boyce N. A comparison of conventional dialytic therapy and acute continuous hemodiafiltration in the management of acute renal failure in the critically ill. Ren Fail 1993; 15:595–602.
Bellomo R, Farmer M, Boyce N. A prospective study of continuous hemodiafiltration in the management of severe acute renal failure in critically ill surgical patients. Ren Fail 1994; 16:759–66.
Kruczynski K, Irvine-Bird K, Toffelmire EB, Morton AR. A comparison of continuous arteriovenous hemofiltration and intermittent hemodialysis in acute renal failure patients in the intensive care unit. ASAIO J 1993; 39:M778–81.
Kierdorf HP, Sieberth HG. Continuous renal replacement therapies versus intermittent hemodialysis in acute renal failure: what do we know? Am J Kidney Dis 1996; 28(Suppl 3):590–6.
Misset B, Timsit JF, Chevret S, Renaud B, Tamion F, Carlet J. A randomized cross-over comparison of the hemodynamic response to intermittent hemodialysis and continuous hemofiltration in ICU patients with acute renal failure. Intensive Care Med 1996; 22:742–6.
Swartz RD, Messana JM, Orzol S, Port FK. Comparing continuous hemofiltration with hemodialysis in patients with severe acute renal failure. Am J Kidney Dis 1999; 34:424–32.
Mehta RL, McDonald B, Gabbai FB, et al. A randomized clinical trial of continuous versus intermittent dialysis for acute renal failure. Kidney Int 2001; 60:1154–63.
Guerin C, Girard R, Selli JM, Ayzac L. Intermittent versus continuous renal replacement therapy for acute renal failure in intensive care units: results from a multicenter prospective epidemiological survey. Intensive Care Med 2002; 28:1411–8.
Kellum JA, Angus DC, Johnson JP, et al. Continuous versus intermittent renal replacement therapy: a meta- analysis. Intensive Care Med 2002; 28:29–37.
Tonelli M, Manns B, Feller-Kopman D. Acute renal failure in the intensive care unit: a systematic review of the impact of dialytic modality on mortality and renal recovery. Am J Kidney Dis 2002; 40:875–85.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985; 13:818–29.
Keene AR, Cullen DJ. Therapeutic intervention scoring system: update 1983. Crit Care Med 1983; 11:1–3.
Simmons EM, Himmelfarb J, Sezer MT, et al. Plasma cytokine levels predict mortality in patients with acute renal failure. Kidney Int 2004; 65:1357–65.
Kresse S, Schlee H, Deuber HJ, Koall W, Osten B. Influence of renal replacement therapy on outcome of patients with acute renal failure. Kidney Int 1999; 56(Suppl 72):S75–8.
Gettings LG, Reynolds HN, Scalea T. Outcome in post- traumatic acute renal failure when continuous renal replacement therapy is applied early vs. late. Intensive Care Med 1999; 25:805–13.
Paganini EP, Tapolyai M, Goormastic M, et al. Establishing a dialysis therapy/patient outcome link in intensive care unit acute dialysis for patients with acute renal failure. Am J Kidney Dis 1996; 28(Suppl 3):S81–9.
Uchino S, Bellomo R, Ronco C. Intermittent versus continuous renal replacement therapy in the ICU: impact on electrolyte and acid-base balance. Intensive Care Med 2001; 27:1037–43.
Manns B, Doig CJ, Lee H, et al. Cost of acute renal failure requiring dialysis in the intensive care unit: clinical and resource implications of renal recovery. Crit Care Med 2003; 31:449–55.
Merkus MP, Jager KJ, Dekker FW, Boeschoten EW, Stevens P, Krediet RT. Quality of life in patients on chronic dialysis: self-assessment 3 months after the start of treatment. The Necosad Study Group. Am J Kidney Dis 1997; 29:584–92.
de Wit GA, Ramsteijn PG, de Charro FT. Economic evaluation of end stage renal disease treatment. Health Policy 1998; 44:215–32.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jacka, M.J., Ivancinova, X. & Gibney, R.T.N. Continuous renal replacement therapy improves renal recovery from acute renal failure. Can J Anesth 52, 327–332 (2005). https://doi.org/10.1007/BF03016071
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016071