
Abstract
Purpose
The multiple organ dysfunction (MOD) score and sequential organ failure assessment (SOFA) score are measures of organ dysfunction and have been validated based on the association of these scores with mortality. We sought to compare the performance of the SOFA and MOD scores in a large cohort of consecutive multisystem intensive care unit (ICU) patients.
Methods
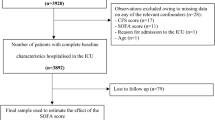
Prospective automated daily measurements of MOD and SOFA scores were performed in 1,436 patients admitted to a multisystem ICU in the Calgary Health Region over a one-year period. Logistic regression modeling techniques were used to describe the association of SOFA and MODS with mortality. Receiver operator characteristic (ROC) curves were used to assess the model’s discriminatory ability.
Results
For ICU and hospital mortality, there was very little practical difference between the SOFA and MOD scores in their ability to discriminate outcome as determined by the area under the ROC. However, compared to previous literature, the discriminatory ability of both scores in this population was weak. As well, the calibration of the models was poor for both scores. The SOFA cardiovascular component score performed better than the MOD cardiovascular component score in the discrimination of both ICU and hospital mortality.
Conclusions
SOFA and MOD scores had only a modest ability to discriminate between survivors and non-survivors. These results question the appropriateness of using organ dysfunction scores as a ’surrogate’ for mortality in clinical trials and suggest further work is necessary to better understand the temporal relationship and course of organ failure with mortality.
Résumé
Objectif
Le score de défaillance multiviscérale (DMV) et le score de SOFA (Sequential Organ Failure Assessment) mesurent la dysfonction organique et ont été validés sur leur association avec la mortalité. Nous avons comparé leur performance chez des patients successivement admis à l’unité des soins intensifs (USI) pour une atteinte multiviscérale. Méthode : Les mesures quotidiennes, prospectives et automatisés des scores de DMV et de SOFA ont été faites chez 1 436 patients admis à une USI multiviscéraux dans la région de Calgary pendant une année. Une modélisation de régression logistique a servi à décrire l’association des scores de SOFA et de DMV à la mortalité. La capacité discriminatoire du modèle a été évaluée par les courbes ROC (Receiver Operator Characteristic).
Résultats
Concernant la mortalité à l’USI et à l’hôpital, les scores de SOFA et de DMV présentaient une très petite différence pratique de capacité à distinguer les résultats comme l’a montré l’aire sous la courbe ROC. Comparée aux données des publications antérieures, la capacité discriminatoire des deux scores était faible pour la population évaluée. Aussi, le calibrage des modèles était pauvre pour les deux scores. Le score de la composante cardiovasculaire du SOFA a présenté une meilleure performance que celui de la DMV quant à la détermination de la mortalité à l’USI et à l’hôpital.
Conclusion
Les scores de SOFA et de DMV n’ont qu’une faible capacité à distinguer les patients qui vont survivre ou non. Cela remet en question la pertinence d’utiliser des scores de dysfonction organique comme «substitut» à la mortalité dans les essais cliniques et incite à chercher à découvrir la relation temporelle entre l’évolution de la défaillance organique et la mortalité.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Baue AE. Multiple, progressive, or sequential systems failure. A syndrome of the 1970s (Editorial). Arch Surg 1975; 110:779–81.
Beal AL, Cerra FB. Multiple organ failure syndrome in the 1990s. Systemic inflammatory response and organ dysfunction. JAMA 1994; 271:226–33.
Baue AE. Multiple organ failure, multiple organ dysfunction syndrome, and systemic inflammatory response syndrome. Why no magic bullets? Arch Surg 1997; 132:703–7.
Deitch EA. Multiple organ failure. Pathophysiology and potential future therapy. Ann Surg 1992; 216:117–34.
Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis- Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996; 22:707–10.
Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med 1995; 23:1638–52.
Bernard GR, Vincent JL, Laterre PF, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 2001; 344:699–709.
Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345:1368–77.
Antonelli M, Moreno R, Vincent JL, et al. Application of SOFA score to trauma patients. Sequential Organ Failure Assessment. Intensive Care Med 1999; 25:389–94.
Vincent JL, de Mendonca A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems ”of the European Society of Intensive Care Medicine. Crit Care Med 1998; 26:1793–800.
Moreno R, Vincent JL, MatosR, et al. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Working Group on Sepsis related Problems of the ESICM. Intensive Care Med 1999; 25:686–96.
Metnitz PG, Lang T, Valentin A, Steltzer H, Krenn CG, Le Gall JR. Evaluation of the logistic organ dysfunction system for the assessment of organ dysfunction and mortality in critically ill patients. Intensive Care Med 2001; 27:992–8.
Hosmer D, Lemeshow S. A goodness -of-fit test for the multiple logistic regression model. Communications in Statistics 1980; A10:1043–69. $$$
Cook R, Cook D, Tilley J, Lee K, Marshall J; Canadian Critical Care Trials Group. Multiple organ dysfunction: baseline and serial component scores. Crit Care Med 2001; 29:2046–50.
Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. N Engl J Med 1998; 338:791–7.
Pettila V, Pettila M, Sarna S, Voutilainen P, Takkunen O. Comparison of multiple organ dysfunction scores in the prediction of hospital mortality in the critically ill. Crit Care Med 2002; 30:1705–11.
Peres Bota D, Melot C, Lopes Ferreira F, Nguyen Ba V, Vincent JL. The multiple organ dysfunction score (MODS) versus the sequential organ failure assessment (SOFA) score in outcome prediction. Intensive Care Med 2002; 28:1619–24.
Suistomaa M, Kari A, Ruokonen E, Takala J. Sampling rate causes bias in APACHE II and SAPS II scores. Intensive Care Med 2000; 26:1773–8.
Bosman RJ, Oudemane van Straaten HM, Zandstra DF. The use of intensive care information systems alters outcome prediction. Intensive Care Med 1998; 24:953–8.
Hammond J, Ward CG, Johnson M, Varas R, Marcial E. The computerized burn unit: experience with a patient data management system. Int J Clin Monit Comput 1989; 6:87–9.
Reich DL, Wood RK Jr,Mattar R, et al. Arterial blood pressure and heart rate discrepancies between handwritten and computerized anesthesia records. Anesth Analg 2000; 91:612–6.
Taylor DE, Whamond JS. Reliability of human and machine measurements in patient monitoring. Eur J Intensive Care Med 1975; 1:53–9.
Lemeshow S, Le Gall JR. Modeling the severity of illness of ICU patients. A systems update. JAMA 1994; 272:1049–55.
Randolph AG, Guyatt GH, Richardson WS. Prognosis in the intensive care unit: finding accurate and useful estimates for counseling patients. Crit Care Med 1998; 26:767–72.
Markgraf R, Deutschinoff G, Pientka L, Scholten T, Lorenz C. Performance of the score systems acute physiology and chronic health evaluation II and III at an interdisciplinary intensive care unit, after customization. Crit Care 2001; 5:31–6.
Moreno R, Apolone G. Impact of different customization strategies in the performance of a general severity score. Crit Care Med 1997; 25:2001–8.
Nathens AB, Marshall JC. Sepsis, SIRS, and MODS: what’s in a name? World J Surg 1996; 20:386–91.
Author information
Authors and Affiliations
Corresponding author
Additional information
Support: Dr. Zygun was supported by the Meredith Graduate Masters Scholarship funded by the Workers Compensation Board of Alberta. Dr. Laupland was supported by the 2000 Bayer Healthcare/Canadian Institutes of Health Research/Canadian Infectious Diseases Society Research Fellowship and a clinical fellowship award from the Alberta Heritage Foundation for Medical Research (AHFMR). Funding for this work was supported in part by grants from the Alberta Heritage Foundation for Medical Research Health Research Fund, and the Calgary Regional Health Authority Special Competition Fund.
Rights and permissions
About this article
Cite this article
Zygun, D.A., Laupland, K.B., Fick, G.H. et al. Neuroanesthesia and Intensive Care Limited ability of SOFA and MOD scores to discriminate outcome: a prospective evaluation in 1,436 patients. Can J Anesth 52, 302–308 (2005). https://doi.org/10.1007/BF03016068
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016068